
Key summary points
To compare the diagnostic value of relative sit-to-stand muscle power with grip strength or gait speed for identifying a history of adverse outcomes in older adults.
AbstractSection FindingsWhen compared to grip strength or gait speed, relative sit-to-stand muscle power offered slightly (but not statistically) higher diagnostic power for identifying a history of recurrent falls and fractures in older adults. However, all tests showed low diagnostic power (AUC < 0.7).
AbstractSection MessageFurther prospective cohort studies should examine the diagnostic power of relative sit-to-stand muscle power for incident falls and fractures. This information is important to evaluate if this test offers true clinical value (and benefit over grip strength or gait speed) for identifying these adverse outcomes.
Abstract
Purpose
To compare the diagnostic value of relative sit-to-stand muscle power with grip strength or gait speed for identifying a history of recurrent falls and fractures in older adults.
Methods
Data from an outpatient clinic included anthropometry (height/weight), bone density, 5 times sit-to-stand time (stopwatch and standardized chair), grip strength (hydraulic dynamometer), and gait speed (4 m). Relative sit-to-stand muscle power (W.kg−1, normalised to body mass) was calculated using a validated equation. Outcomes of falls (past 1 year) and fractures (past 5 years) were self-reported and verified by medical records wherever possible. Binary logistic regression considering for potential confounders (age, sex, BMI, Charlson comorbidity index, femoral neck bone density) and receiver operating characteristics (ROC) curves were used in statistical analysis.
Results
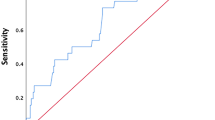
508 community-dwelling older adults (median age: 78 years, interquartile range: 72, 83, 75.2% women) were included. Compared to greater relative sit-to-stand muscle power (1.62–3.78W.kg−1 for women; 2.03–3.90W.kg−1 for men), those with extremely low relative sit-to-stand muscle power were 2.35 (95% CI 1.54, 3.60, p < 0.001) and 2.41 (95% CI 1.25, 4.65, p = 0.009) times more likely to experience recurrent falls and fractures, respectively, in fully adjusted model. Compared to grip strength or gait speed, relative sit-to-stand muscle power showed the highest area under the ROC curve for identifying recurrent falls (AUC: 0.64) and fractures (AUC: 0.62). All tests showed low diagnostic power (AUC: < 0.7).
Conclusion
Relative sit-to-stand muscle power performed slightly (but not statistically) better than grip strength or gait speed for identifying a history of recurrent falls and fractures in older adults. However, all tests showed low diagnostic power.

Similar content being viewed by others


Data availability
All data are available in this manuscript.
References
England, P.H., 2022 Falls and fractures: applying all our health, OfHIa. Disparities, Editor.
Sherrington C et al (2019) Exercise for preventing falls in older people living in the community. Coch Database Syst Rev. 1:12424
Peel NM (2011) Epidemiology of falls in older age. Can J Aging 30(1):7–19
Harvey NC et al (2021) Sarcopenia definitions as predictors of fracture risk independent of FRAX((R)), falls, and BMD in the osteoporotic fractures in men (MrOS) study: a meta-analysis. J Bone Miner Res 36(7):1235–1244
Cruz-Jentoft AJ et al (2019) Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing 48(1):16–31
Bhasin S et al (2020) Sarcopenia definition: the position statements of the sarcopenia definition and outcomes consortium. J Am Geriatr Soc 68(7):1410–1418
Kirk B et al (2021) Sarcopenia definitions and outcomes consortium (SDOC) criteria are strongly associated with malnutrition, depression, falls, and fractures in high-risk older persons. J Am Med Dir Assoc 22(4):741–745
Viccaro LJ, Perera S, Studenski SA (2011) Is timed up and go better than gait speed in predicting health, function, and falls in older adults? J Am Geriatr Soc 59(5):887–892
Alcazar J et al (2020) Relation between leg extension power and 30-s sit-to-stand muscle power in older adults: validation and translation to functional performance. Sci Rep 10(1):16337
Alcazar J et al (2021) “Fat but powerful” paradox: association of muscle power and adiposity markers with all-cause mortality in older adults from the EXERNET multicentre study. Br J Sports Med 55(21):1204–1211
Losa-Reyna J et al (2021) Impact of relative muscle power on hospitalization and all-cause mortality in older adults. J Gerontol A Biol Sci Med Sci 77:781
Alcazar J et al (2021) Threshold of relative muscle power required to rise from a chair and mobility limitations and disability in older adults. Med Sci Sports Exerc 53(11):2217–2224
Merchant RA et al (2020) Relationship between fear of falling, fear-related activity restriction, frailty, and sarcopenia. J Am Geriatr Soc 68(11):2602–2608
Alcazar J et al (2018) The sit-to-stand muscle power test: An easy, inexpensive and portable procedure to assess muscle power in older people. Exp Gerontol 112:38–43
Baltasar-Fernandez I et al (2021) Relative sit-to-stand power cut-off points and their association with negatives outcomes in older adults. Sci Rep 11(1):19460
Losa-Reyna J et al (2022) Impact of relative muscle power on hospitalization and all-cause mortality in older adults. J Gerontol A Biol Sci Med Sci 77(4):781–789
Alcazar J et al (2022) Letter to the editor number of chair stands should not be considered a muscle function measure, but a physical performance measure what can we do then. J Frailty Aging 11(2):245–246
Charlson ME et al (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40(5):373–383
Kirk B et al (2020) Associations between osteoporosis, the severity of sarcopenia and fragility fractures in community-dwelling older adults. Eur Geriatr Med 11(3):443–450
Alcazar J et al (2021) Relative sit-to-stand power: aging trajectories, functionally relevant cut-off points, and normative data in a large European cohort. J Cachexia Sarcopenia Muscle 12(4):921–932
Vasunilashorn S et al (2009) Use of the short physical performance battery score to predict loss of ability to walk 400 meters: analysis from the inchianti study. J Gerontol A Biol Sci Med Sci 64(2):223–229
Mandrekar JN (2010) Receiver operating characteristic curve in diagnostic test assessment. J Thorac Oncol 5(9):1315–1316
DeLong ER, DeLong DM, Clarke-Pearson DL (1988) Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics 44(3):837–845
Cawthon PM et al (2019) Strong relation between muscle mass determined by D3-creatine dilution, physical performance, and incidence of falls and mobility limitations in a prospective cohort of older men. J Gerontol A Biol Sci Med Sci 74(6):844–852
Kirk B et al (2020) Effects of exercise and whey protein on muscle mass, fat mass, myoelectrical muscle fatigue and health-related quality of life in older adults: a secondary analysis of the liverpool hope university-sarcopenia ageing trial (LHU-SAT). Eur J Appl Physiol 120(2):493–503
Alcazar J, Lopez-Moranchwl I, Losa-Reyna J, Baltasar-Fernandez I, Garcia-Garcia FJ, Alegre LM, Ara I (2021) App Review: powerfrail for the assessment of relative muscle power and frailty in older people. Br J Sports Med 11:864
Acknowledgements
The authors would like to thank the participants and the Australian Institute for Musculoskeletal Science (AIMSS) for their support throughout the study and our Fracture Liaison Nurse Mrs. Solange Bernardo for her assistance at the Falls and Fractures Clinic.
Author information
Authors and Affiliations
Contributions
BK, CF, JZ, and GD designed the study; BK, MS, CF, MG, and GD were involved in data collection; CF and BK analysed the data, which was overseen by SV (Biostatistician); BK and CF primarily wrote the paper; all authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflicts of interest
The authors have no direct conflicts of interest regarding the content of this manuscript.
Ethical approval
Ethical approval was provided by the Western Health Low Risk Ethics Panel at Sunshine Hospital (ID: QA2018.106_44499).
Informed consent
As data were collected as part of standard care, a waiver of informed consent was sought.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kirk, B., French, C., Gebauer, M. et al. Diagnostic power of relative sit-to-stand muscle power, grip strength, and gait speed for identifying a history of recurrent falls and fractures in older adults. Eur Geriatr Med 14, 421–428 (2023). https://doi.org/10.1007/s41999-023-00778-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41999-023-00778-x