
Abstract
Objectives
To examine costs of care from a healthcare sector perspective within 1 year before death in patients with non-cancer diseases and patients with cancer.
Methods
This nationwide registry-based study identified all Danish citizens dying from major non-cancer diseases or cancer in 2010–2016. Applying the cost-of-illness method, we included costs of somatic hospitals, including hospital-based specialist palliative care, primary care, prescription medicine and hospice expressed in 2022 euros. Costs of patients with non-cancer diseases and cancer were compared using regression analyses adjusting for sex, age, comorbidity, residential region, marital/cohabitation status and income level.
Results
Within 1 year before death, mean total healthcare costs were €27,185 [95% confidence interval (CI) €26,970–27,401] per patient with non-cancer disease (n = 109,723) and €51,348 (95% CI €51,098–51,597) per patient with cancer (n = 108,889). The adjusted relative total healthcare costs, i.e. the ratio of the mean costs, of patients with non-cancer diseases was 0.64 (95% CI 0.63–0.66) at 12 months before death and 0.91 (95% CI 0.90–0.92) within 30 days before death compared with patients with cancer.
Mean costs of hospital-based specialist palliative care and hospice in the year leading up to death were €17 (95% CI €13–20) and €90 (95% CI €77–102) per patient with non-cancer disease but €1552 (95% CI €1506–1598) and €3411 (95% CI €3342–3480) per patient with cancer.
Conclusions
Within 1 year before death, total healthcare costs, mainly driven by hospital costs, were substantially lower for patients with non-cancer diseases compared with patients with cancer. Moreover, the costs of hospital-based specialist palliative care and hospice were minimal for patients with non-cancer diseases.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
In this nationwide study, conducted within a healthcare system offering universal coverage, it was observed that costs to the public healthcare sector gradually increased on a monthly basis during the year preceding death, irrespective of the underlying disease. However, costs were markedly lower for patients with non-cancer diseases than for patients with cancer, and costs of hospital-based specialist palliative care and hospice were minimal in patients suffering from non-cancer diseases. |
These findings indicate the need for political strategies and considerations on how to achieve a better balance and prioritisation of end-of-life healthcare resources, particularly among patients with non-cancer diseases. |
1 Introduction
Accounting for 71% of all deaths globally, chronic disease is the leading cause of death, with cancer being the most dominant cause, followed by ischaemic heart disease, stroke, chronic obstructive pulmonary disease and diabetes [1]. Terminally ill patients suffering from chronic diseases require an increased level of care as death approaches, resulting in considerable healthcare costs [2]. Thus, previous studies have estimated that approximately 8.5–11.2% of healthcare budgets in high-income countries are spent in the last year of life [3,4,5,6].
Ageing populations have translated into a rising proportion of individuals dying from chronic diseases [2,3,4,5]. Therefore, the share of gross domestic product spent on care at the end of life may rise in the coming years [7]. This trend poses challenges to existing health policies that aim to control healthcare costs and prioritise resources effectively. Additionally, research indicates that healthcare costs at the end of life vary depending on the specific chronic disease causing death, with patients dying from non-cancer diseases generally incurring lower healthcare costs compared with those dying from cancer [6, 8,9,10,11,12,13,14,15]. This disparity may be attributed to variations in high-intensity healthcare services, such as chemotherapy and inpatient hospital care, particularly towards the end of life [6, 8,9,10,11,12,13,14,15]. However, access to palliative care during the final stages of life has been associated with a reduction in high-intensity interventions [16,17,18,19,20], lower healthcare costs [17, 18, 21,22,23,24] and improved quality of life [16, 25,26,27,28], but it is primarily offered to patients with cancer [29,30,31,32]. Nonetheless, only few studies can be identified that have explored the patterns of various healthcare costs according to the disease causing death in the months preceding death [8,9,10]. Furthermore, most studies adopted mixed economic perspectives when examining costs related to care at the end of life, covering costs from a healthcare sector perspective, while also including some, but not all, public sector costs [6, 11, 13, 14, 33, 34]. This mixed methodological approach limits the usefulness in informing resource prioritisation within the healthcare sector. Therefore, knowledge is warranted that identifies the patterns of costs of care as death approaches within a healthcare system with universal coverage, comparing patients dying from non-cancer diseases and patients dying from cancer, while also considering potential confounding factors. By applying a cost-of-illness method and adopting a healthcare sector perspective, it is possible to quantify the economic burden of end-of-life healthcare services and illustrate allocation of resources by the underlying disease causing death. This knowledge can inform future healthcare planning, particularly in systems aiming to ensure equity in healthcare utilisation and increase financial sustainability within the healthcare sector [35, 36].
Therefore, in this nationwide study from a healthcare system with universal coverage, the costs of providing healthcare services in the year leading up to death in patients dying from non-cancer diseases and patients dying from cancer were estimated. Adopting a healthcare sector perspective, we aimed to include all costs to the healthcare sector, encompassing costs of primary care, prescription medicine, somatic hospitals, including hospital-based specialist palliative care, and hospice care.
2 Methods
2.1 Study Design and Setting
We conducted this nationwide study including all adult Danish citizens dying from one of seven major non-cancer diseases or from cancer between 1 January 2010 and 31 December 2016.
The study applied a cost-of-illness method to estimate the value of the resources used for providing healthcare services related to care at the end of life in Denmark [37, 38]. Adopting a healthcare sector perspective, we aimed to include all costs to the healthcare sector each month during decedents’ last year of life as this 12 month time period aligns with the estimation practices of other activities in the public sector and annual budget expenditures always form the budget framework for prioritisation discussions in Denmark and many other countries. Relevant healthcare costs included costs of somatic hospitals (inpatient admissions, outpatient specialist clinic visits and emergency room visits), including hospital-based specialist palliative care, primary care (general practitioners, practicing medical specialists and other health professionals, e.g. physiotherapists), prescription medicine and hospice care.
To ensure equity in access to primary care, hospitals and hospices in Denmark, these healthcare services are tax-funded and provided free of charge to all citizens [39].
However, medicine costs for medication out of hospital are only partly subsidised. Thus, for all prescription medicines sold in Danish pharmacies, a fixed co-payment scheme is in place with an annual maximum of DKK 4320 per patient (2022 level) [40]. Even so, terminally ill patients with a life expectancy of weeks to months may be granted drug reimbursement and receive all prescription medicine free of charge [41]. Although drug reimbursement due to terminal illness is accessible for all patients with a short life expectancy, it is offered mainly to patients with cancer [42, 43].
Based on individual-level data from population-based medical and administrative registries in Denmark, we obtained information on each Danish citizen using their unique civil personal register (CPR) number. The CPR number is a personal identification number assigned to all Danish citizens at birth or immigration, enabling accurate and unambiguous linkage across the various Danish registries [44].
The study was reported to the Danish Data Protection Agency (record number 2015-57-0002) by registration at Aarhus University (Aarhus University record number 2016-051-000001/977). Under Danish law, approvals from ethics committees and consent from patients are not required for non-interventional registry-based studies.
2.2 Decedents
We identified all adult Danish citizens registered with one of seven selected non-cancer diseases or cancer as the cause of their death using the Danish Registry of Causes of Death. From death certificates for all Danish decedents, the Danish Registry of Causes of Death encompasses information on cause of death and date of death with a completeness of approximately 97% [45]. In accordance with the Dartmouth Atlas Projects of end-of-life care, the selected non-cancer diseases causing death included dementia, diabetes, heart failure, ischaemic heart disease, stroke, chronic liver disease or chronic obstructive pulmonary disease [46].
The Danish Civil Registration System, an administrative registry with individual-level information on all Danish citizens, was used to obtain data on decedents’ age at death, sex, residential region and marital/cohabitation status [47].
From Statistics Denmark, the central authority of Danish statistics, we obtained data on decedents’ mean annual household income during the 5 years leading up to death, that is, excluding the year of death [48]. Household income was grouped into three levels according the national medians of household income in the year of death, obtained from Statistics Denmark [49]. The income levels encompassed: low income level (< 50% of national median), middle income level (50–100% of national median) and high income level (> 100% of national median).
We computed a comorbidity score for comorbidities at time of death according to the Charlson Comorbidity Index. The comorbidity score was calculated from weights of 19 selected diagnoses in relation to hospitalisation and outpatient visits during the last 10 years leading up to death, excluding the disease causing death [50, 51]. Data on diagnoses were obtained from the Danish National Registry of Patients, a nationwide registry with information from inpatient and outpatient hospital contacts since 1995, including patients’ discharge diagnoses [52].
2.3 Somatic Hospital Costs
We computed direct costs of somatic hospital care, encompassing costs of inpatient hospital admissions, including medicine given during hospital admissions and medicine handed out by the hospital during outpatient specialist clinic visits, emergency room visits and hospital-based specialist palliative care utilisation. These costs were computed using the Diagnosis Related Group (DRG) and Danish Ambulatory Grouping System (DAGS) tariffs within the Danish National Patient Registry. The registry has served as basis for the payment of public and private hospitals via the DRG/DAGS tariffs since 2002 [53]. The DRG/DAGS tariffs are determined at the national administrative level and reflect average costs of treatments of patients across Danish hospitals, covering all hospital costs [53].
2.4 Primary Care Costs
Data on the costs of primary care at the end of life were obtained from the Danish National Health Service Registry. Since 1990, the National Health Service Registry has been effective, and it includes a weekly gross fee for primary care services from private practicing health professionals reimbursed by the National Health Insurance. Primary care costs included all services in private practice, covering contacts with general practitioners, practicing medical specialists, physiotherapists, chiropractors, psychologists, dentists and chiropodists.
In addition to the gross fee directly linked to services in general practice, Statistics Denmark computes a special estimate adding capitation payment for patients affiliated with the general practitioners and clinical practice cost fees, corresponding to approximately one-third of the costs [54, 55].
Since information on services in the National Health Service Registry is based on payments reimbursed by the National Health Insurance, the completeness is assumed to be good [56].
Costs associated with services not reimbursed by the National Health Insurance are not included in the analyses as they are not registered in the National Health Service Registry, e.g. physiotherapist and dental treatments without subsidy.
2.5 Prescription Medicine Costs
The Danish National Prescription Registry was used to identify costs of out-of-hospital prescription medicine dispensed from all Danish pharmacies, including the pharmacy selling price, dispensing fee and patients’ co-payment. In the present study, costs were modified by subtracting the patients’ co-payment from the dispensing fee, aiming to accurately reflect costs to the healthcare sector. Since 1995, the Danish National Prescription Registry has contained individual-level information on all prescriptions dispensed at Danish pharmacies [57].
2.6 Hospice Care Costs
The five Danish regions are the administrative bodies responsible for the costs of hospice care, but these are not included in the DRG/DAGS system. According to a daily bed charge determined by the regions, the hospices’ costs are reimbursed directly from the regions. We retrieved the daily bed charge from each of the five Danish regions for each of the years from 2010 to 2016 and used the Danish National Registry of Patients to obtain information on total days spent in hospice.
2.7 Statistical Analysis
Descriptive statistics were used to describe the cohort of included patients dying from non-cancer disease and from cancer. For patients with non-cancer diseases and patients with cancer, we computed mean monthly and annual costs per patient of somatic hospitals, including hospital-based specialist palliative care, primary care, prescription medicine and hospice care. Additionally, we estimated mean total costs of all the included healthcare services per patient by month and as a total within the last year of life. The mean monthly costs per patient were plotted by the underlying cause of death in the year leading up to death. For costs of hospital-based specialist palliative care and hospice, however, the mean monthly costs per patient were presented in graphs by the underlying disease causing death in the last 3 months of life. Furthermore, we estimated the proportion of patients accessing the services of hospital-based specialist palliative care and hospice care in the year leading up to death as well as the mean monthly costs of these particular patients.
We computed relative monthly costs of patients with non-cancer diseases when compared with patients with cancer. The relative monthly costs were adjusted for potential confounding factors that are common causes of both the underlying disease and healthcare service costs, including sex, age at death, comorbidity, residential region, marital/cohabitation status and income level. The adjustment was performed using a Poisson regression with a gamma function in the denominator. This approach accounts for the continuous nature of the outcome on a positive semi-definite scale. The standard error was estimated using a robust variance estimator to relax the assumption of Poisson distributed outcome. The adjusted relative monthly costs of hospital-based specialist palliative care and hospice, however, were graphed by months before death during the 3 months leading up to death.
Additionally, all analyses were repeated after restriction to patients dying from chronic obstructive pulmonary disease and patients dying from lung cancer as recent data suggest comparable levels of symptom burden and palliative care needs in these two patient populations [58, 59].
Finally, we made supplemental analyses examining a potential shift in the distribution of total end-of-life healthcare costs according to decedents’ age at death, as this has previously been suggested [9].
All costs were expressed in 2022 euros and we inflated past costs using the net price index reported by Statistics Denmark [60].
The statistical analyses were conducted on a secure remote server hosted by the Statistics Denmark using Stata 17 software (StataCorp. 2021. Stata Statistical Software: Release 17. College Station, TX: StataCorp LLC).
3 Results
We included 109,723 patients dying from one of the seven selected non-cancer diseases (dementia, diabetes, heart failure, ischaemic heart disease, stroke, chronic liver disease or chronic obstructive pulmonary disease) and 108,889 patients dying from cancer in the period from 1 January 2010 to 31 December 2016 (Supplementary Table 1). The demographic data showed that patients dying from non-cancer diseases were older, were more likely to live alone and had a lower income level than patients dying from cancer (Supplementary Table 1).
3.1 Healthcare Costs
The mean total costs of the included healthcare services were €27,185 [95% confidence interval (CI) €26,970–27,401] per patient with non-cancer disease and €51,348 (95% CI €51,098–51,597) per patient with cancer in the year leading up to death (Table 1). Hospital costs contributed 91.7% to total costs in patients with non-cancer diseases and 89.1% in patients with cancer.
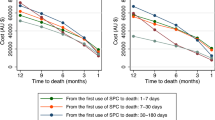
Mean monthly total healthcare costs per patient with non-cancer disease increased from €1038 (95% CI €1014–1063) at month 12 before death to €11,320 (95% CI €11,197–11,443) within 30 days before death. Accordingly, for patients with cancer, this increased from €2103 (95% CI €2073–2133) at 12 months before death to €15,254 (95% CI €15,136–15,371) within 30 days before death (Fig. 1, Supplementary Table 2).

Mean monthly costs per patient for primary care, prescription medicine, somatic hospitals and total healthcare costs in the year leading up to death for patients dying from non-cancer diseases and for patients dying from cancer
When compared with patients with cancer, the adjusted relative total healthcare costs of patients with non-cancer diseases stayed relatively stable in the months leading up to death, until the last month in which it increased (Fig. 2). Thus, at 12 months before death, the adjusted relative total healthcare costs was 0.64 (95% CI 0.63–0.66) for patients with non-cancer diseases when compared with patients cancer. This decreased to 0.53 (95% CI 0.52–0.55) at four months before death and increased to 0.91 (95% CI 0.90–0.92) within 30 days before death (Fig. 2).

Adjusted relative costs of primary care, prescription medicine, somatic hospitals and total healthcare costs in the year leading up to death for patients with non-cancer diseases compared with patients with cancer
In the subgroup analyses of patients dying from chronic obstructive pulmonary disease and from lung cancer, we found less pronounced differences in total end-of-life healthcare costs (Figs. 3, 4). Compared with patients dying from lung cancer, the adjusted relative total healthcare costs of patients dying from chronic obstructive pulmonary disease was 1.10 (95% CI 1.04–1.17) at 12 months before death, decreasing to 0.75 (95% CI 0.72–0.78) at 2 months before death and then increasing to 1.12 (95% CI 1.09–1.16) within 30 days before death (Fig. 4).

Mean monthly costs per patient of primary care, prescription medicine, somatic hospitals and total healthcare costs in the year leading up to death for patients dying from chronic obstructive pulmonary disease and for patients dying from lung cancer

Adjusted relative costs of primary care, prescription medicine, somatic hospitals and total healthcare costs in the year leading up to death for patients with chronic obstructive pulmonary disease compared with patients with lung cancer
In supplementary analyses, in patients with non-cancer diseases and patients with cancer alike, we found that the pattern of total end-of-life healthcare costs shifted when stratifying on age at death, i.e. the higher age, the lower costs. The adjusted relative estimates of total healthcare costs showed decreasing difference with increasing age group (Supplementary Fig. 1).
3.2 Hospital-Based Specialist Palliative Care and Hospice Care Costs
Hospital-based specialist palliative care and hospice care were mainly utilised in the last month of life and provided predominantly for patients with cancer. Thus, 0.6% of patients with non-cancer diseases and 27.6% of patients with cancer received hospital-based specialist palliative care in the year leading up to death, whereas 0.5% of patients with non-cancer diseases and 18.4% of patients with cancer were admitted to hospice.
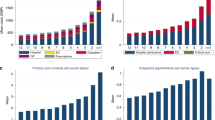
Within the last 30 days leading up to death, the mean costs of hospital-based specialist palliative care were €9 (95% CI €7–11) per patient with non-cancer disease and €771 (95% CI €751–791) per patient with cancer (Fig. 5). Accordingly, the mean costs of hospice were €57 (95% CI €47–66) per patient with non-cancer disease and €2868 (95% CI €2808–2928) per patient with cancer (Fig. 5).

Mean monthly costs per patient and adjusted relative costs of hospital-based specialist palliative care and hospice care in patients dying from non-cancer diseases and in patients dying from cancer
The adjusted relative costs of hospital-based specialist palliative care costs were 0.02 (95% CI 0.01–0.02) for patients with non-cancer diseases when compared with patients with cancer within 30 days before death, whereas the adjusted relative hospice costs were 0.03 (95% CI 0.02–0.03) (Fig. 5).
For the patients accessing hospital-based specialist palliative care, the mean costs of hospital-based specialist palliative care were €1360 (95% CI €1098–1622) per patient with non-cancer disease and €2794 (95% CI €2726–2863) per patient with cancer within 30 days before death. Correspondingly, for patients accessing hospice care, the mean costs of hospice were €11,624 (95% CI €9923–13,325) per patient with non-cancer disease and €15,600 (95% CI 15,337–15,863) per patient with cancer.
Overall, similar patterns of hospital-based specialist palliative care costs and hospice costs were found in the subgroup analyses of patients dying from chronic obstructive pulmonary disease compared with patients dying from lung cancer (Supplementary Fig. 2).
4 Discussion
Our nationwide study within a healthcare system with universal coverage indicates substantial variations in total healthcare costs at the end of life when comparing patients dying from non-cancer diseases with patients dying from cancer. During the last year of life, the total healthcare costs, mainly driven by hospital costs, increased irrespective of the disease causing death but were considerably lower for patients with non-cancer diseases than for patients with cancer. However, in the last months of life, relative differences were reduced although persisting.
In the year leading up to death, costs of hospital-based specialist palliative care and hospice were minimal for patients with non-cancer diseases, as these palliative care interventions were provided primarily for patients with cancer. This pattern was also found when comparing patients dying from chronic obstructive pulmonary disease with patients dying from lung cancer.
While acknowledging that there are considerable differences in the organisation and financing of healthcare systems, our findings are congruent with the few previous studies, which also adopted a healthcare sector perspective when examining healthcare costs at the end of life [8,9,10]. These studies, conducted in England and Australia, also suggested that patients with non-cancer diseases incur substantially lower total end-of-life healthcare costs than patients with cancer, and that hospital care costs were the main driver of costs [8,9,10]. Exploring healthcare service utilisation at the end of life in Denmark in a previous study, we found that the number of hospital admissions and length of stay in patients dying from non-cancer diseases do not vary considerably from those of patients dying from cancer [61]. This combination of comparable hospital activity but lower costs among patients with non-cancer diseases may be explained by a more active treatment approach among patients with cancer, often involving expensive medicine administered during hospital admission [15]. Even so, consistent with other studies, the findings from the present study showed that the relative difference in total healthcare costs among patients with non-cancer diseases and patients with cancer was reduced in the last months of life, although patients with cancer persisted to incur higher costs [8,9,10].
One possible explanation of this may relate to a relatively faster rise in the use of high-intensity treatments and potentially costly medical interventions especially in the last month of life in patients with non-cancer diseases rather than in patients with cancer. This is in accordance with findings from our previous research showing that in the 6 months leading up to death, patients dying from non-cancer diseases were twice as frequently admitted to intensive care units and had a greater risk of dying there than patients dying from cancer [62]. Overall, the present study demonstrated that healthcare costs at the end of life decreased with increasing age, as did the difference in costs between patients with non-cancer diseases and patients with cancer. These findings align with previous research that has established a correlation between age and a reduced likelihood of receiving expensive high-intensity treatments [9, 62]. Furthermore, as age increases, there is also a diminished difference in intensive care unit admissions between patients with different underlying diseases [62]. This trend may partly be explained by a different general attitude towards active or intensive interventions in older patients compared with their younger counterparts.
A mounting body of evidence describes that palliative care improves quality of life [16, 25,26,27,28] and reduces healthcare costs at the end of life [17, 18, 21,22,23,24], irrespective of the disease causing death. Moreover, some cost-effective palliative care interventions have even been presented [21, 63]. This, however, has not noticeably affected practice for patients with non-cancer diseases as palliative care is still received mainly by patients with cancer [29,30,31,32]. This is in line with the findings in the present study of extremely low average costs of hospital-based specialist palliative care and hospice care in patients with non-cancer diseases.
Considered in conjunction with previous studies, this may indicate that cancer patients receiving specialist palliative care, including hospice care, may have been spared some costly, potentially futile, high-intensity interventions at the end of life, which may have improved the quality of life for these patients and their families [16,17,18,19,20].
The findings of differences in terms of costs of hospital-based specialist palliative care and hospice care for patients with non-cancer diseases and patients with cancer were similar to the observed difference in the analyses of patients with chronic obstructive pulmonary disease and patients with lung cancer only. Thus, substantially lower costs were observed among patients with chronic obstructive pulmonary disease. This difference between patients with chronic obstructive pulmonary disease and patients with lung cancer is remarkable since both patient populations experience fairly equivalent symptoms and needs of care at the end of life [58, 59] and would most likely benefit somewhat equally from palliative care interventions [64].
The present study has some major advantages. We used a nationwide population-based design in a healthcare system with universal coverage, which enabled individual-level linkage between national and medical registries with prospectively collected data [52, 65, 66]. Additionally, we examined end-of-life healthcare costs across different healthcare settings, whereas previous studies have mostly been focusing on hospital costs [6, 8,9,10].
Using the Danish Registry of Causes of Death, which is approximately 97% complete, to identify patients dying from a non-cancer diseases or from cancer made selection bias unlikely [45]. However, some misclassification of the disease causing death may exist, which we tried to account for by including only well-defined chronic conditions in our analyses.
Data from the Danish National Health Service Registry and the Danish National Registry of Patients serve as basis for payment wherefore the coverage is assumed to be good. Thus, we expect a low risk of information bias concerning primary care costs, hospital costs and hospice costs [52, 66]. Correspondingly, data on prescription medicine costs from the Danish National Prescription Registry was considered complete and valid from 1995 [57].
Analyses were adjusted for several potential confounding factors, but some influence from residual confounding may remain. Moreover, our results may be confounded from unmeasured factors on which information was not available in the present study, e.g. life style factors, that may vary between patients with non-cancer diseases and patients with cancer and influence healthcare costs. However, these factors are not likely to explain the entire difference in end-of-life healthcare costs among patients with non-cancer diseases and patients with cancer.
Several limitations need to be considered when interpreting our findings. We applied a cost-of-illness method and adopted a healthcare sector perspective aiming to include all costs to the healthcare sector. Thus, the present study does not include all types of end-of-life healthcare costs. Psychiatric hospital costs were not included, but these are expected only to be a minor part of end-of-life healthcare costs. Moreover, resources for providing municipality-based end-of-life care services were not included, covering homecare, homecare nursing and rehabilitation (i.e. services outside the public healthcare sector). However, it is not possible to trace municipal costs to individual patients in Danish registries. Furthermore, patients’ own costs (travel, patient co-payment for prescription medicine and over-the-counter medication, etc.) as well as indirect costs such as productivity loss resulting from time off employment were not included either. Broadening of the economic perspective into including these costs outside the healthcare sector might show less variation in end-of-life care costs when comparing patients with non-cancer diseases and patients with cancer. For instance, patients with non-cancer diseases receive considerably more non-medical homecare at the end of life than patients with cancer [67]. Even so, adopting a broader economic perspective would be beyond the scope of the present study, focusing on prioritisation of resources in the healthcare sector.
To estimate hospital costs, we used the DRG/DAGS tariffs, which are measures of average costs of services rather than a fee-for-service approach. While providing incentives for hospitals to limit the services per patient, the DRG/DAGS tariffs are thought to improve efficiency, but we cannot disentangle whether costs of terminally ill patients are actually reflected in the DRG/DAGS tariffs. Hence, if terminally ill patients incur more costs than accounted for in the DRG/DAGS tariffs, we are most likely to underestimate the actual costs of hospital contacts. Correspondingly, hospice costs are measured by a daily bed charge that fails to take variation in costs into account. However, in the comparison of patients dying from non-cancer diseases and from cancer, this may not introduce substantial information bias.
Furthermore, the available data in the present study only go until 2016, which may limit their usefulness for projecting future costs. Even so, we believe the findings from these data may inform resource allocation decisions for care at the end of life, since neither the capacity of specialist palliative care in Denmark nor the distribution of patients with cancer versus patients with non-cancer diseases who access specialist palliative care services have changed considerably from 2016 and onwards [68].
Simply estimating high costs using a cost-of-illness method is debated as a tool for decision making, since it does not provide information on potential inefficiencies [69,70,71]. However, we believe the findings from the present study, conducted within a healthcare system with universal coverage and specifically focusing on comparing patients dying from non-cancer diseases with those dying from cancer while accounting for potential confounding factors, provide valuable insights into the identification of patients with high healthcare costs and the understanding of resource allocation. Consequently, these findings hold the potential to contribute to political considerations focusing on ensuring appreciable interventions for patients nearing the end of life.
5 Conclusions
The present study extends our understanding of the substantial healthcare costs related to the end-of-life phase according to different underlying diseases. In the year leading up to death, total healthcare costs of patients with non-cancer diseases were substantially lower than for patients with cancer although relative differences were reduced in the last months of life. Together with the findings of minimal costs of hospital-based specialist palliative care and hospice care in patients suffering from non-cancer diseases, consideration is warranted on how to achieve a better balance and prioritisation of end-of-life healthcare resources, particularly among patients with non-cancer diseases.
References
World Health Organization. Noncommunicable diseases 2021 (accessed 06.01 2022).
Howdon D, Rice N. Health care expenditures, age, proximity to death and morbidity: Implications for an ageing population. J Health Econ. 2018;57:60–74. https://doi.org/10.1016/j.jhealeco.2017.11.001. (published Online First: 2017/11/29).
Christensen BJ, Gørtz M, Kallestrup-Lamb M. Medical Spending in Denmark. Fisc Stud. 2016;37(3–4):461–97. https://doi.org/10.1111/j.1475-5890.2016.12119.
Tanuseputro P, Wodchis WP, Fowler R, et al. The health care cost of dying: a population-based retrospective cohort study of the last year of life in Ontario, Canada. PLoS ONE. 2015;10(3): e0121759. https://doi.org/10.1371/journal.pone.0121759. (published Online First: 2015/03/27).
French EB, McCauley J, Aragon M, et al. End-of-life medical spending in last twelve months of life is lower than previously reported. Health Aff (Millwood). 2017;36(7):1211–7. https://doi.org/10.1377/hlthaff.2017.0174. (published Online First: 2017/07/07).
Polder JJ, Barendregt JJ, van Oers H. Health care costs in the last year of life–the Dutch experience. Soc Sci Med. 2006;63(7):1720–31. https://doi.org/10.1016/j.socscimed.2006.04.018. (published Online First: 2006/06/20).
European Commission D-GfEaFA. The 2021 Ageing Report: Economic and Budgetary Projections for the EU Member States (2019-2070), 2021.
Langton JM, Reeve R, Srasuebkul P, et al. Health service use and costs in the last 6 months of life in elderly decedents with a history of cancer: a comprehensive analysis from a health payer perspective. Br J Cancer. 2016;114(11):1293–302. https://doi.org/10.1038/bjc.2016.75. (published Online First: 2016/04/27).
Reeve R, Srasuebkul P, Langton JM, et al. Health care use and costs at the end of life: a comparison of elderly Australian decedents with and without a cancer history. BMC Palliat Care. 2017;17(1):1. https://doi.org/10.1186/s12904-017-0213-0. (published Online First: 2017/06/24).
Luta X, Diernberger K, Bowden J, et al. Healthcare trajectories and costs in the last year of life: a retrospective primary care and hospital analysis. BMJ Support Palliat Care. 2020. https://doi.org/10.1136/bmjspcare-2020-002630. (published Online First: 2020/12/04).
Tangka FK, Subramanian S, Sabatino SA, et al. End-of-life medical costs of medicaid cancer patients. Health Serv Res. 2015;50(3):690–709. https://doi.org/10.1111/1475-6773.12259. (published Online First: 2014/11/27).
Gielen B, Remacle A, Mertens R. Patterns of health care use and expenditure during the last 6 months of life in Belgium: differences between age categories in cancer and non-cancer patients. Health Policy (Amsterdam, Netherlands). 2010;97(1):53–61. https://doi.org/10.1016/j.healthpol.2010.03.002.
Sullivan SS, Li J, Wu YB, et al. Complexity of chronic conditions’ impact on end-of-life expense trajectories of medicare decedents. J Nurs Adm. 2017;47(11):545–50. https://doi.org/10.1097/NNA.0000000000000541.
Hung P, Hsu SH, Wang SY. Associations between end-of-life expenditures and hospice stay length vary by clinical condition and expenditure duration. Value Health. 2020;23(6):697–704. https://doi.org/10.1016/j.jval.2020.01.021. (published Online First: 2020/06/17).
Smith TJ, Hillner BE. Bending the cost curve in cancer care. N Engl J Med. 2011;364(21):2060–5. https://doi.org/10.1056/NEJMsb1013826. (published Online First: 2011/05/27).
Gaertner J, Siemens W, Meerpohl JJ, et al. Effect of specialist palliative care services on quality of life in adults with advanced incurable illness in hospital, hospice, or community settings: systematic review and meta-analysis. BMJ. 2017;357: j2925. https://doi.org/10.1136/bmj.j2925. (published Online First: 2017/07/06).
Ernecoff NC, Bilderback A, Bellon J, et al. Associations between Reason for Inpatient Palliative Care Consultation, Timing, and Cost Savings. J Palliat Med. 2021;24(10):1525–38. https://doi.org/10.1089/jpm.2020.0636. (published Online First: 2021/03/25).
Gonzalez-Jaramillo V, Fuhrer V, Gonzalez-Jaramillo N, et al. Impact of home-based palliative care on health care costs and hospital use: a systematic review. Palliat Support Care. 2021;19(4):474–87. https://doi.org/10.1017/s1478951520001315. (published Online First: 2020/12/10).
Skov Benthien K, Adsersen M, Petersen MA, et al. Is specialized palliative cancer care associated with use of antineoplastic treatment at the end of life? A population-based cohort study. Palliat Med. 2018;32(9):1509–17. https://doi.org/10.1177/0269216318786393. (published Online First: 2018/07/14).
Vestergaard AHS, Neergaard MA, Fokdal LU, et al. Utilisation of hospital-based specialist palliative care in patients with gynaecological cancer: temporal trends, predictors and association with high-intensity end-of-life care. Gynecol Oncol. 2023;172:1–8. https://doi.org/10.1016/j.ygyno.2023.02.019. (published Online First: 2023/03/12).
Luta X, Ottino B, Hall P, et al. Evidence on the economic value of end-of-life and palliative care interventions: a narrative review of reviews. BMC Palliat Care. 2021;20(1):89. https://doi.org/10.1186/s12904-021-00782-7. (published Online First: 2021/06/25).
Spilsbury K, Rosenwax L. Community-based specialist palliative care is associated with reduced hospital costs for people with non-cancer conditions during the last year of life. BMC Palliat Care. 2017;16(1):68. https://doi.org/10.1186/s12904-017-0256-2. (published Online First: 2017/12/09).
Seow H, Salam-White L, Bainbridge D. Community-based specialist palliative care teams and health system costs at end of life: a retrospective matched cohort study. CMAJ Open. 2019;7(1):E73-e80. https://doi.org/10.9778/cmajo.20180113. (published Online First: 2019/02/14).
May P, Normand C, Cassel JB, et al. Economics of palliative care for hospitalized adults with serious illness: a meta-analysis. JAMA Intern Med. 2018;178(6):820–9. https://doi.org/10.1001/jamainternmed.2018.0750. (published Online First: 2018/05/02).
Oluyase AO, Higginson IJ, Yi D, et al. Health Services and Delivery Research. Hospital-based specialist palliative care compared with usual care for adults with advanced illness and their caregivers: a systematic review. Southampton: NIHR Journals Library; 2021.
Quinn KL, Stukel T, Stall NM, et al. Association between palliative care and healthcare outcomes among adults with terminal non-cancer illness: population based matched cohort study. BMJ. 2020;370:m2257. https://doi.org/10.1136/bmj.m2257.
Diop MS, Rudolph JL, Zimmerman KM, et al. Palliative Care Interventions for Patients with Heart Failure: A Systematic Review and Meta-Analysis. J Palliat Med. 2017;20(1):84–92. https://doi.org/10.1089/jpm.2016.0330. (published Online First: 2016/12/03).
Veronese S, Gallo G, Valle A, et al. Specialist palliative care improves the quality of life in advanced neurodegenerative disorders: NE-PAL, a pilot randomised controlled study. BMJ Support Palliat Care. 2017;7(2):164–72. https://doi.org/10.1136/bmjspcare-2014-000788. (published Online First: 2015/07/18).
Knaul FM, Farmer PE, Krakauer EL, et al. Alleviating the access abyss in palliative care and pain relief-an imperative of universal health coverage: the Lancet Commission report. Lancet. 2018;391(10128):1391–454. https://doi.org/10.1016/s0140-6736(17)32513-8. (published Online First: 2017/10/17).
Bloom CI, Slaich B, Morales DR, et al. Low uptake of palliative care for COPD patients within primary care in the UK. Eur Respir J. 2018. https://doi.org/10.1183/13993003.01879-2017. (published Online First: 2018/02/16).
Tobin J, Rogers A, Winterburn I, et al. Hospice care access inequalities: a systematic review and narrative synthesis. BMJ Support Palliat Care. 2022;12(2):142–51. https://doi.org/10.1136/bmjspcare-2020-002719. (published Online First: 2021/02/21).
Lau C, Meaney C, Morgan M, et al. Disparities in access to palliative care facilities for patients with and without cancer: a retrospective review. Palliat Med. 2021;35(6):1191–201. https://doi.org/10.1177/02692163211007387. (published Online First: 2021/04/16).
Kelley AS, McGarry K, Gorges R, et al. The burden of health care costs for patients with dementia in the last 5 years of life. Ann Intern Med. 2015;163(10):729–36. https://doi.org/10.7326/m15-0381. (published Online First: 2015/10/27).
Yi D, Johnston BM, Ryan K, et al. Drivers of care costs and quality in the last 3 months of life among older people receiving palliative care: a multinational mortality follow-back survey across England, Ireland and the United States. Palliat Med. 2020;34(4):513–23. https://doi.org/10.1177/0269216319896745. (published Online First: 2020/02/06).
Clabaugh G, Ward MM. Cost-of-illness studies in the United States: a systematic review of methodologies used for direct cost. Value Health. 2008;11(1):13–21. https://doi.org/10.1111/j.1524-4733.2007.00210.x. (published Online First: 2008/02/02).
Citizens TDMoHaS. The Health Legislation, § 2 2018 [Available from: https://www.retsinformation.dk/eli/lta/2018/1286#idbed2f88d-d892-4e44-b8d5-5df12be19d48. Accessed 26 Apr 2022.
Hodgson TA, Meiners MR. Cost-of-illness methodology: a guide to current practices and procedures. Milbank Mem Fund Q Health Soc. 1982;60(3):429–62.
Larg A, Moss JR. Cost-of-illness studies: a guide to critical evaluation. Pharmacoeconomics. 2011;29(8):653–71. https://doi.org/10.2165/11588380-000000000-00000. (published Online First: 2011/05/25).
Schmidt M, Schmidt SAJ, Adelborg K, et al. The Danish health care system and epidemiological research: from health care contacts to database records. Clin Epidemiol. 2019;11:563–91. https://doi.org/10.2147/clep.S179083. (published Online First: 2019/08/03).
Ehlers LH. Introduction to medical market access in Denmark: Djøf Forlag. 2019.
Møller PK. Pricing and reimbursement of drugs in Denmark. Eur J Health Econ. 2003;4(1):60–5. https://doi.org/10.1007/s10198-003-0165-6. (published Online First :2004/12/21).
Daugaard C, Neergaard MA, Vestergaard AHS, et al. Socioeconomic inequality in drug reimbursement during end-of-life care: a nationwide study. J Epidemiol Community Health. 2019;73(5):435–42. https://doi.org/10.1136/jech-2018-211580. (published Online First: 2019/02/04).
Bell C, Nielsen MK, Neergaard MA, et al. Remaining lifetime after recognition of terminal illness depends on diagnosis: a nationwide population-based cohort study. J Pain Symptom Manage. 2017;53(1):116–23. https://doi.org/10.1016/j.jpainsymman.2016.08.002. (published Online First: 2016/10/11).
Mainz J, Hess MH, Johnsen SP. The Danish unique personal identifier and the Danish Civil Registration System as a tool for research and quality improvement. Int J Qual Health Care. 2019;31(9):717–20. https://doi.org/10.1093/intqhc/mzz008. (published Online First: 2019/06/21).
Helweg-Larsen K. The Danish Register of causes of death. Scand J Public Health. 2011;39(7 Suppl):26–9. https://doi.org/10.1177/1403494811399958.
Goodman DC, Esty AR, Fisher ES, et al. A report of the Dartmouth Atlas Project: trends and variation in end-of-life care for medicare beneficiaries with severe chronic illness. The Dartmouth Institute; 2011.
Schmidt M, Pedersen L, Sorensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–9. https://doi.org/10.1007/s10654-014-9930-3.
Baadsgaard M, Quitzau J. Danish registers on personal income and transfer payments. Scand J Public Health. 2011;39(7 Suppl):103–5. https://doi.org/10.1177/1403494811405098. (published Online First: 2011/08/04).
Statistics Denmark. INDKF201: Main table for family income statistics by type of income, family type, population, price unit and unit 2004-2019. www.statistikbanken.dk/INDKF201. Accessed 22 June 2021.
Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–83.
Thygesen SK, Christiansen CF, Christensen S, et al. The predictive value of ICD-10 diagnostic coding used to assess Charlson comorbidity index conditions in the population-based Danish National Registry of Patients. BMC Med Res Methodol. 2011;11:83. https://doi.org/10.1186/1471-2288-11-83.
Schmidt M, Schmidt SA, Sandegaard JL, et al. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–90. https://doi.org/10.2147/CLEP.S91125.
Ankjaer-Jensen A, Rosling P, Bilde L. Variable prospective financing in the Danish hospital sector and the development of a Danish case-mix system. Health Care Manag Sci. 2006;9(3):259–68. https://doi.org/10.1007/s10729-006-9093-1. (published Online First: 2006/10/05).
Pedersen KM, Andersen JS, Søndergaard J. General practice and primary health care in Denmark. J Am Board Fam Med. 2012;25(Suppl 1):S34–8. https://doi.org/10.3122/jabfm.2012.02.110216. (published Online First: 2012/03/21).
Statistics D. Health Insurance Statistics 2022. https://www.dst.dk/en/Statistik/dokumentation/documentationofstatistics/health-insurance-statistics. Accessed 11 Jan 2022.
Andersen JS, Olivarius Nde F, Krasnik A. The Danish National Health Service Register. Scand J Public Health. 2011;39(7 Suppl):34–7. https://doi.org/10.1177/1403494810394718.
Pottegård A, Schmidt SAJ, Wallach-Kildemoes H, et al. Data resource profile: the Danish National Prescription Registry. Int J Epidemiol. 2017;46(3):798–898. https://doi.org/10.1093/ije/dyw213. (published Online First: 2016/10/30).
Joshi M, Joshi A, Bartter T. Symptom burden in chronic obstructive pulmonary disease and cancer. Curr Opin Pulm Med. 2012;18(2):97–103. https://doi.org/10.1097/MCP.0b013e32834fa84c. (published Online First: 2012/01/21).
Weingaertner V, Scheve C, Gerdes V, et al. Breathlessness, functional status, distress, and palliative care needs over time in patients with advanced chronic obstructive pulmonary disease or lung cancer: a cohort study. J Pain Symptom Manage. 2014;48(4):569-81.e1. https://doi.org/10.1016/j.jpainsymman.2013.11.011. (published Online First: 2014/03/13).
Statistics Denmark. Net price index 1980-2021. https://www.dst.dk/en/Statistik/emner/priser-og-forbrug/forbrugerpriser/nettoprisindeks. Accessed 1 July 2021.
Vestergaard AHS, Neergaard MA, Christiansen CF, et al. Hospitalisation at the end of life among cancer and non-cancer patients in Denmark: a nationwide register-based cohort study. BMJ Open. 2020;10(6): e033493. https://doi.org/10.1136/bmjopen-2019-033493. (published Online First: 2020/07/01).
Lyngaa T, Christiansen CF, Nielsen H, et al. Intensive care at the end of life in patients dying due to non-cancer chronic diseases versus cancer: a nationwide study in Denmark. Crit Care (London, England). 2015;19:413-015-1124–1. https://doi.org/10.1186/s13054-015-1124-1.
Kaufman BG, Granger BB, Sun JL, et al. The Cost-Effectiveness of Palliative Care: Insights from the PAL-HF Trial. J Card Fail. 2021;27(6):662–9. https://doi.org/10.1016/j.cardfail.2021.02.019. (published Online First: 2021/03/19).
Henoch I, Ekberg-Jansson A, Löfdahl CG, et al. Benefits, for patients with late stage chronic obstructive pulmonary disease, of being cared for in specialized palliative care compared to hospital. A nationwide register study. BMC Palliat Care. 2021;20(1):130. https://doi.org/10.1186/s12904-021-00826-y. (published Online First: 2021/08/26).
Christiansen CF, Christensen S Fau - Johansen MB, Johansen Mb Fau - Larsen KM, et al. The impact of pre-admission morbidity level on 3-year mortality after intensive care: a Danish cohort study. (1399-6576 (Electronic))
Olivarius NF, Hollnagel H, Krasnik A, et al. The Danish National Health Service Register. A tool for primary health care research. Dan Med Bull. 1997;44(4):449–53.
Vestergaard AHS, Christiansen CF, Neergaard MA, et al. Healthcare utilisation trajectories in patients dying from chronic obstructive pulmonary disease, heart failure or cancer: a nationwide register-based cohort study. BMJ Open. 2021;11(11): e049661. https://doi.org/10.1136/bmjopen-2021-049661. (published Online First: 2021/11/26).
Jarlbæk L, Mikkelsen TB, Timm H. Kortlægning af den specialiserede palliative indsats i Danmark, 2019.
Behrens C, Henke K, et al. Cost of illness studies: no aid to decision making: Reply to Shiell et al. (Health Policy, 8 (1987) 317-323). Health Policy. 1988;10(2):137–41. https://doi.org/10.1016/0168-8510(88)90002-4. (published Online First: 1988/09/06).
Rice DP. Cost-of-illness studies: fact or fiction? Lancet. 1994;344(8936):1519–20. https://doi.org/10.1016/s0140-6736(94)90342-5. (published Online First: 1994/12/03).
Shiell A, Gerard K, Donaldson C. Cost of illness studies: an aid to decision-making? Health Policy. 1987;8(3):317–23.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The present study was supported by the Independent Research Fund Denmark (grant number 4004-00609B), Fonden af 1870 (grant number 200652), C.C. Klestrup & Hustru Henriette Klestrups Mindelegat (grant number 10761), Fabrikant Einar Willumsens Mindelegat (grant number 131 217) and Helga og Peter Kornings Fond (grant number 472123-002-40). The sponsors had no involvement in either stages of the work.
Conflicts of Interest
The authors have no conflicts of interest to declare.
Availability of Data and Material
All data sources can be obtained from Statistics Denmark, the central authority for Danish statistics.
Ethics Approval
Under Danish law, approvals from ethics committees and consent from patients are not required when conducting observational studies. An approval was obtained for use of the included data sources from the Danish Data Protection Agency (record number 2015-57-0002) by registration at Aarhus University (Aarhus University record number 2016-051-000001/977).
Consent to Participate
Not applicable
Consent for Publication (from patients/participants)
Not applicable
Code Availability
Available from the corresponding author upon request.
Author Contributions
Anne Høy Seemann Vestergaard (AHSV), Lars Holger Ehlers (LHL), Mette Asbjoern Neergaard (MAN), Christian Fynbo Christiansen (CFC), Jan Brink Valentin (JBV) and Søren Paaske Johnsen (SPJ) contributed to the conception and design of the study. Acquisition of data was done by AHSV, CFC and SPJ. AHSV performed the statistical analysis with assistance from JBV. The first draft of the manuscript was written by AHSV and all authors commented on previous versions of the manuscript. All authors read and approved the final version of the manuscript.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Vestergaard, A.H.S., Ehlers, L.H., Neergaard, M.A. et al. Healthcare Costs at the End of Life for Patients with Non-cancer Diseases and Cancer in Denmark. PharmacoEconomics Open 7, 751–764 (2023). https://doi.org/10.1007/s41669-023-00430-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41669-023-00430-1