
Abstract
Objectives
Children with autism spectrum disorder experience communication difficulties that can make it challenging to engage in conversations. Their caregivers also often struggle with finding ways to support the child’s communication. Parent-implemented interventions and visual supports are evidence-based practices to support the communication skills of children with autism.
Method
A multi-method design (single-case multiple probe and qualitative) was used to evaluate the effects of family photographs, training, and telecoaching on parental implementation of communication strategies. Three parents and their children with and at risk for autism participated.
Results
Results indicate that the use of photographs increased the communication strategies used by all parents. Telecoaching further increased the overall strategy use for two parents. Interviews with the parents indicate spontaneous generalization and maintenance of strategy use.
Conclusion
Family photos and naturalistic developmental behavior intervention approaches have the potential to improve communication about past events between parents and children with and at risk for ASD.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Autism spectrum disorder (ASD) is often characterized by difficulties in social communication skills (American Psychiatric Association, 2013). Common social communication challenges experienced by children with ASD include differences in joint attention and social reciprocity (Leekam & Ramsden, 2006). In addition, expressive communication, or the ability to communicate wants and needs, make comments, and answer questions during conversations, is often challenging for children with ASD (Chiang & Lin, 2008). These social communication struggles, coupled with the caregiver’s struggles with successfully supporting the child’s communication needs, may negatively affect the quality of the relationships of children with ASD with others, including their families (Hall & Graff, 2011; McDonnell et al., 2021).
Young children learn language during natural family routines such as playing with family members, going on walks, and visiting relatives. Through the predictability and repetition of these routines and conversations with parents, children are exposed to new vocabulary and begin to learn concepts relevant to their environment. In addition to everyday routines, children learn through special and non-routine events such as birthday parties and family vacations. For example, after the first trip to a beach, a child may learn new vocabulary such as sandcastle, starfish, and shell that they would otherwise not learn within their typical daily routines.
Parents of typically developing children often start engaging their children in these conversations about past events around the age of two (Kulkofsky & Koh, 2009). These conversations help increase the child’s speech and language skills, serve as the building blocks for more advanced literacy and memory skills (Gauvreau, 2015; Leech & Rowe, 2021; Ornstein et al., 2004), and help develop the child’s own ability to talk about past events (Leech & Rowe, 2021).
These are different reasons why conversations about past events may be challenging for autistic individuals. One theory states that parents of children with ASD may be hesitant to engage their children in these conversations due to their perceived language difficulties thus they may limit the benefits their child may get from these conversations (McDonnell et al., 2021, Nelson & Fivush, 2004). Other researchers claim that the social communication difficulties experienced by children with ASD can make their ability to discuss past events and participate in the back-and-forth of conversations a challenging activity (Caron et al., 2018; Westby & Culatta, 2016). However, most researchers agree that early caregiver training in ways to support their child’s communication and communication supports, including visual supports, for the child with ASD will enhance their ability to communicate.
Visual supports have been shown to be an effective strategy to address issues related to the communication challenges experienced by children with ASD (Rutherford et al., 2020). Visual supports are broadly described as any physical item that can enhance an individual’s understanding of their environment, social expectations and norms, or abstract concepts (Arthur-Kelly et al., 2009; Rutherford et al., 2020). Caregivers and educators have cited a lack of resources, lack of time, community attitude towards visual supports, and limited knowledge of the different types of visual supports available as barriers to the implementation of visual supports (Donato et al., 2014). Given that photographs are easy to personalize, regularly accessible, widely used, and cost-effective, they have the potential to be an effective visual tool to support communication.
Despite the widespread use of photographs to communicate and share information and life events with family and friends (Villi, 2012), there is little research on the use of photographs as visual supports for children with ASD. To date, only two studies have investigated the use of family photographs during conversations about past events between children with ASD and family members (Gauvreau, 2015; Yang, 2018).
In the first study, Gauvreau (2015) investigated the effects of photos taken with mobile technology on the accuracy of retelling of events of three young children with ASD. Results indicated that photo supports effectively increased the accuracy of the information reported by children with ASD about their school day during conversations with their parents. In the second study, Yang (2018) reported that the use of photos supported a more comprehensive range of interactions between children with ASD and their grandparents. These conversations included recent events shared by the grandparent and the child and events in the more distant past that had only been experienced by the grandparent. Both evaluations show promise in the use of photographs as communication support for children with ASD. It is important to note, however, that just providing caregivers with visual support is not enough. In order to fully harness the benefits of visual supports, their introduction should be paired with training on different ways they can be used during naturally occurring routines (Rutherford et al., 2020).
Naturalistic Developmental Behavioral Interventions (NDBI) are a group of interventions that combine developmental and behavioral approaches. These interventions are conducted in the child’s natural setting and utilize behavioral strategies and natural contingencies (Schreibman et al., 2015). NDBIs include antecedent-based strategies (e.g., modeling, prompting) and consequence-based strategies (e.g., contingent responses and verbal expansions of child utterances; Ruppert et al., 2016). Research on NDBIs and NDBI-based interventions (i.e., naturalistic interventions) suggests that parents can implement them with high levels of fidelity as interventionists (Schreibman et al., 2015). However, for many parents, coaching (i.e., follow-up feedback) is required to fully implement all elements of the intervention (Meadan et al., 2016).
Although parent-implemented interventions are effective, parents have reported a need for training to be more accessible (Raulston et al., 2019). To address this issue, interventions implemented at a distance (i.e., telepractice) have been recommended (Raulston et al., 2019). Telepractice is an umbrella term used to describe services, typically in medical and educational settings, delivered at a distance (Knutsen et al., 2016). For caregivers residing in rural areas (Akamoglu et al., 2020) and for families looking for more flexible options (Raulston et al., 2019), telepractice-delivered interventions are an ideal delivery option. Recent parent-implemented naturalistic studies (Akamoglu & Meadan, 2019; Meadan et al., 2016; Wainer & Ingersoll, 2015) have been conducted via telepractice with success.
Although there is growing evidence that parents can be taught naturalistic interventions via telepractice, to our knowledge, there have been no published investigations of parent-implemented interventions delivered via telepractice aimed at increasing the communication of children with and at risk for ASD during conversations about past events.
In the present study, we used multi-method methodology (i.e., single case and qualitative analyses) to investigate the impact of the use of photographs and photographs paired with parent training and coaching in naturalistic approaches to answer the following research questions:
(1) Is there a functional relation between the use of family photos and the average number of communication strategies implemented by parents?; (2) Is there a functional relation between the use of family photos combined with parent training and coaching on NDBI approaches and the average number of communication strategies implemented by parents?; and (3) Do parents rate the intervention as socially valid?
Method
Participants
Participants were recruited via flyers distributed at local schools and posted on social media pages for parents and professionals working with children with developmental disabilities and/or speech impairments. Parents were eligible to participate in this study if they were (a) 18 years of age or older, (b) able to speak and read English, and (c) willing to share family photos and information about the child’s social and adaptive skills. Children were eligible to participate if per parent report they (a) were between 3 and 10 years old; (b) were diagnosed or had a special education eligibility of a developmental disability (e.g., ASD) or speech impairment; (c) experienced difficulty talking about past events; (d) used more than 10 expressive words, signs, gestures, or augmentative and alternative communication (AAC) symbols that were easily understandable by others; (e) were able to recognize photos of people or objects; and (f) had hearing and vision within normal range.
Three dyads completed the study in two (Dyad 1) to 3 months (Dyads 2 and 3). All the children who qualified for the current study attended the same special education preschool designed for children with moderate developmental disabilities, where they received speech and occupational therapy services.
Dyad 1 consisted of Diana and her son Grayson. Grayson was diagnosed with ASD by a psychologist. He spoke English in one- to three-word utterances and often engaged in vocal stereotypy. Grayson answered what, where, and who questions per parent report.
Dyad 2 consisted of Lauren and her son David. The family also had an older daughter who was occasionally present during the sessions. David qualified for special education services under the category of speech impairment and was considered at-risk for ASD. At the time of the study, he was on a waitlist for a medical autism evaluation. He spoke English in short sentences, and when motivated, in sentences with utterances greater than five words in length. Lauren reported that it could be difficult for her to understand her son’s speech, which caused David to become frustrated. He was able to answer what, where, who, why, and how questions per parent report.
Dyad 3 was made up of Hai and her daughter Elsa. Elsa was identified with ASD by an early intervention specialist after a doctor referral. Elsa and her mother spoke English and Mandarin at home and was able to answer what, where, who, and why questions per parent report. She used an iPad loaded with the LAMP Words for Life™ application as an augmentative communication system to communicate at school. Elsa spoke English fluently at home with her mom during all sessions. The adults at home (father, mother, and grandmother) spoke Mandarin among each other. Hai reported that Elsa also spoke Mandarin; however, her level of fluency is unknown (Table 1).
Procedure
A single-case multiple probe design was employed across three parent–child dyads (Ledford & Gast, 2018), as well as qualitative methodologies (Merriam & Tisdell, 2015) were utilized to investigate the effects of the intervention. A multiple probe design was selected as the experimental design allows the investigation of non-reversible behaviors, while reducing the strain on participants due to a long baseline (Ledford & Gast, 2018). All session lasted 3 min. Sessions that took place more than 7 days apart are represented through disconnected dots. Sessions that took place more than 10 days after the previous session are represented by the two slash (i.e., //) symbol. Social validity interviews were conducted with parents after the intervention to collect data. A thematic analysis (Merriam & Tisdel, 2015) approach was used to examine the qualitative data.
Zoom video conference software (V.5.0.5) was used throughout the current study to support video conferences between the families and lead researcher. Parents were free to choose the area of the home for all sessions. Parents used personal mobile phones or tablet computers to video conference with the researcher. An additional personal device was used to view the family photographs in the photos-only phase (i.e., B phase) and the post-training and coaching phase (i.e., B2 phase). Sessions were recorded and stored in a secure online cloud. Prior to baseline, dyads were provided with an extendable selfie stick, tripod stand holder for cellphones, and a single head clip-on lapel microphone to support the video conference sessions. Between the B and B2 phases and before the training, the researcher delivered two laminated half-sheet summaries of the target strategies. All deliveries were conducted in-person but contactless. At the beginning of each session, the researcher started by confirming that the location of the dyad, as well as the positioning of the audio and camera, allowed both the parent and child to be visible and heard. Parents then were asked to try and stay seated with their child, so that they would remain visible to the camera, and to bring their child back to the area if they moved out of the camera’s view at any time during the session. The researcher would then set a 3-min timer followed my muting herself and stopping her video to minimize distraction. The researcher did not interrupt any ongoing session if the child moved from their original position. After 3 min of dyadic interaction, the researcher unmuted, turned on her camera, and told the parent the time was up.
Before baseline, the researcher asked parent participants to identify past events that they believed would be of interest to their child and for which they had photos available. Selected events included holidays (e.g., Christmas, Easter, Halloween), family vacations, teatime, visiting family members, and outdoor activities. Parents selected a variety of photos for each event, which they uploaded to a secure folder location. If the parent provided more than five photographs for an event, the researcher selected pictures that would be more appealing for the child and would create more communication opportunities (e.g., more people, positive affect).
Baseline A and B Phase: Photos Only
During baseline (A) sessions, all parents were asked to engage their child in a 3-min conversation about one of the five events. No photos were available for baseline sessions. After a stable baseline was established for the child behavior, the researcher organized and programmed five family photos per event (a total of 25 photos for all five events) into a Google™ Slides presentation. Each of the five events was presented with a title page, the name of the event, and five photos depicting the event. Prior to the start of the B phase for Dyad 1, the research team decided that only five sessions would be conducted for all dyads. We chose five sessions based on What Works Clearinghouse (2020) standards for minimum sessions per phase, due to time constraints, and to decrease possible disinterest as a result of the same photos being used repeatedly over several sessions. B phase procedures were identical to baseline (e.g., 3-min conversations, same instructions) except for parents being asked to use the photos on the tablet to talk about the event with their child.
Training
After five B-phase sessions, the researcher met individually with parent to complete the training portion of the study. Parents were trained in the “MORE” intervention. This intervention was created by combining various NDBI-based approaches. Parents were taught how to model (Bruinsma et al., 2020; Schreibman et al., 2015), offer opportunities (Alpert & Kaiser, 1992; Bruinsma et al., 2020; Daar et al., 2015; Soto et al., 2008), and respond and expand (Bruinsma et al., 2020; Schreibman et al., 2015; Soto et al., 2008). Training was on average 33 min (range 27–37 min) and was delivered to parents via Zoom using PowerPoint. Parents were taught to model by pointing to the picture and labeling key vocabulary as they spoke; offer opportunities by asking WH (who, what, where) questions, waiting 5 s to allow the child to respond and follow their lead, and offering binary choices if there was no response from the child, followed by waiting another 5 s; and responding and expanding the child’s utterances by praising and adding a detail about the event.
The training followed a behavior skills training approach, which consisted of instruction, modeling, rehearsal, and feedback (Nigro-Bruzzi & Sturmey, 2010; Sarokoff & Sturmey, 2004) and was delivered via Zoom. A PowerPoint® presentation was used for the instruction step. For the modeling step, sample videos and family photos were used to model and discuss how parents could use the strategies in their conversations. The researcher included individualized examples for each dyad (i.e., photographs and conversations from baseline and B phase for training opportunities). For the rehearsal and feedback components, the researcher and parent took turns playing the role of the child to practice the strategies. This procedure was repeated until the parent demonstrated correct, independent use of each strategy at least twice.
B2 Phase: Photos, Training, and Coaching
After the training, parents were once again asked to engage their child in a 3-min conversation about past events in the list using the photos on the tablet (same events from baseline and B phase). After each session, the researcher and parent discussed: (a) how the parent felt the session went, (b) which strategies the parent implemented correctly, and (c) an area of improvement. After discussing the area of improvement, a goal was set for the following session. This goal was reviewed with the parent at the beginning of the following session.
Social Validity
Following the intervention, the researcher asked parents to meet via Zoom for a follow-up meeting. First, the researcher presented parents with the preliminary results graphs and explained the progress seen in the different dependent variables for parent and child through the study. A combination of surveys and interview questions was used to examine the intervention’s social validity. This combined approach has been previously recommended to thoroughly assess social validity for caregiver-implemented telepractice interventions (Chung et al., 2020).
Interview and survey questions were developed by adapting the Treatment Acceptability Rating Form-Revised (TARF-R, Reimers & Wacker, 1988) and following the guidelines recommended by Wolf (1978) to assess social validity in single case studies and by Turan and Meadan (2011) for early intervention studies. Diana and Lauren answered all social validity questions during the interview with the researcher. Due to English being her second language, Hai requested that the questions be emailed to her in advance and that she be allowed to provide her responses in writing. The researcher then asked follow-up questions with Hai during an interview and combined the written responses with the interviews to create a complete and cohesive transcript. The researcher adapted the coding procedures recommended for qualitative interviews by Merriam and Tisdell (2015) and previously used by Raulston et al. (2019) to analyze data from interviews with parents of children with ASD.
The researcher and a research assistant, both who at the time were doctoral students in a special education program, independently examined each transcript and employed inductive analysis to extract themes from the data. Afterwards, they met to discuss and consolidate the themes. When a disagreement occurred, a discussion took place until a consensus was reached (Saldaña, 2021). The researcher and coder then pulled quotes from the text to illustrate each theme. Additionally, parent answers to each survey question were compiled and added. The answers were divided by three to calculate an average for each question (Table 3). The interview portion of the meeting took an average of 15 min to complete. All interview sessions were video recorded. Parents answered a total of 21 Likert-scale questions on a 1 to 5 scale with 1 representing a very negative experience and a 5 representing a very positive experience, and 17 open-ended questions.
Measures
In the B phase, the IV was the addition of family photographs programmed on a Google™ Slides presentation and presented on a tablet device. For the B2 phase, we implemented a treatment package that included (a) the same 25 family photographs used in phase B, (b) a parent training in the MORE strategies, and (c) parent coaching.
The conversation transcripts were examined to code the dependent variables. The primary DV was the average frequency of target strategy implementation per utterance. An utterance was defined as each subject-verb-preposition unit of text (Bergen et al., 2009; McDonnell et al., 2021) with the exception of responses which could be a subject-verb-preposition (e.g., that is right!) or a single word (e.g., yeah!). The secondary dependent variable was the total number of original WH questions (i.e., first time the parent asked that question during the conversation) the child answered correctly or attempted to answer (i.e., answered incorrectly or the answer was not intelligible).
Data Analyses
Traditional single-case design visual analysis was used to assess changes in level, trend, variability, immediacy effects, and overlapping data within and across similar phases (Kratochwill et al., 2013) to determine the influence of the independent variable on the primary dependent variable. A thematic analysis was used to analyze the qualitative data.
The first author, a doctoral candidate in special education and a certified special educator with more than 8 years of experience working with families of children with disabilities, served as the parent trainer and coach for all dyads. She coded all parent (primary coder) and child-dependent variables and will be hereafter referenced as the researcher. The fourth author, a doctoral candidate in special education, coded the parent use of strategies for interobserver agreement and completed the procedural fidelity coding. The sixth author, also a doctoral candidate in special education, coded the number of parent utterances and child responses for interobserver agreement.
Treatment Fidelity and Interobserver Agreement (IOA)
Total count IOA (Cooper et al., 2020) was used to calculate percentage agreement. To ensure fidelity, the researcher utilized self-monitoring task analysis during baseline, training, and coaching sessions. The fourth author watched at least 20% of randomly selected sessions for each phase and rated the procedural and treatment fidelity (100% of training sessions and 20% of the coaching sessions). The researcher trained the fourth and sixth authors on coding procedures until they achieved 90% agreement on two consecutive sessions, then completed IOA for at least 20% of randomly selected sessions across dyads for each phase(i.e., 5 sessions for baseline, 3 for the B phase, and 4 for the B2 phase). When IOA fell below 80%, the researcher retrained the coders. A coding guidebook with operational definitions of each variable, examples, and non-examples was developed to ensure coding consistency.
Strategy frequency IOA was 93% in the baseline (range 86–100%), 86.6% in the B phase (range 68.8–95.8%), and 84.5% (76.3–91.7%) in the B2 phase. The number of utterances IOA was 93.79% in the baseline (84 to 98.3%), 95.02% in the B phase (92.6–96.97), and 95.4% in the B2 phase (87 to 100%). For the child DV, IOA for WH questions answered correctly was 94.8% in the baseline (90–100%), 100% in the B phase, and 93.7% (81–100%) in the B2 phase. For WH questions attempted to answer IOA was 100% in the baseline, 76.7% in the B phase (50–100%), and 93.3% in the B2 phase (80–100%). Procedural fidelity was 100% in the baseline, 94.4% in the B phase (83–100%), and 100% in the B2 phase. Training and coaching fidelity were both 100%.
Transcripts were automatically generated through the Zoom transcription service after each session. All automatically generated transcripts were verified and corrected as needed by the researcher. Twenty percent of all researcher transcripts per phase were randomly selected to assess the researcher’s transcript reliability. The line-by-line agreement of parent utterances was completed. The number of agreements was divided by the number of agreements plus disagreements and multiplied by 100 to obtain a percentage agreement of transcript reliability. Transcript IOA was 93.5% in the baseline (81.4–100%), 96.9% in the B phase (90.7–100%), and 98.8% in the B2 phase (95.1–100%).
Results
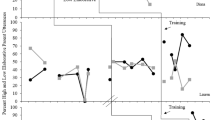
Figure 1 displays the average percentage of strategies used per parent utterance and the average percentage of WH questions the child answered or attempted to answer (out of the total number of original WH questions the parent asked) in each phase.

Parent and child dependent variable. Note. Closed circles represent parent dependent variable and open squares represent child dependent variable
Parent Behaviors
In baseline, Diana engaged in low levels of average strategy use (M = 11%; range 6–23%). Upon introduction of the B phase, there was a small increase in the level of her strategy use with a decreasing trend throughout the phase (M = 20%; range 9–25%). During the B2 phase, a small-moderate increase in the level of strategy use was observed and maintained throughout the phase (M = 34%; range 27–44%). Lauren engaged in low and stable strategy use levels with a decreasing trend (M = 17%; range 11–26%) in baseline. In the B phase, there was a slight increase in level with variability (M = 22%; range 10–33%). During the B2phase, a small-moderate increase in level with an increasing trend (M = 42%; range 21–57%) was observed. During baseline, Hai engaged in low and stable levels of strategy use (M = 24%; range 7–34%). Upon implementation of the B phase there was an immediate increase in level (M = 40%; range 26–49%), which was maintained during the B2 phase (M = 49%; range 41–59%). The mean frequency use and range of each strategy across baseline, B, and B2 phases for each dyad are presented in Table 2.
Child Behaviors
Grayson’s WH questions answered or attempted generally followed his mother’s strategy use with low levels in the baseline (M = 20%; range 10–36%) and an increase with the addition of the family photographs in the B phase (M = 32%; range 7–67%) and a small moderate increase in the B2 phase (M = 30%; range 17–56%). David’s ability to answer the questions also mostly mimicked Lauren’s strategy use and the incorporation of visual supports with low to moderate levels in the baseline (M = 37%; range 0–75%). In the B phase, the incorporation of visual supports helped David answer or attempt to answer more WH questions as we see moderate to high levels initially separate of Lauren’s strategy use; however, this did not maintain as we see a decreasing trend mimicking Lauren’s strategy use at the end of the phase (M = 49%; range 9–88%). In the B2 phase we observe a small-moderate increase in level with more stability (M = 58%; range 0–79%). Finally, in baseline Elsa mostly followed her mother’s lead with low and mostly stable levels of WH questions answered or attempted (M = 28%; range 0–71%). Upon implementation of the B phase, there was an immediate increase in level with a decreasing trend (M = 45%; range 18–67%). In the B2 phase, we initially observe an immediate change in level with a decreasing trend (M = 53%; range 29–100%).
Social Validity
Parents completed 21- Likert-scale questions and 17 open-ended questions during the qualitative interviews. The Likert-scale questions were presented using a 1 to 5 scale with a score of 1 representing a very negative experience or response and a score of 5 representing a very positive experience or response. Parents were asked to rate the feasibility of the intervention, its alignment with the parent’s goals for themselves, the intervention’s perceived effectiveness, their feelings towards the intervention components (e.g., photos, training, and coaching), the usefulness of the strategies for their child’s communication, and the level of difficulty of implementing these strategies. Mothers rated the intervention very positively with scores of 4 (i.e., positive experience) to 5 (i.e., very positive experience) in all areas, with the exception of two specific strategies, “ask WH questions” and “offer wait time” which had scores ranging from 2 (difficult) to 5 (very easy).
The analysis of the qualitative data resulted in the identification of four themes: (1) ease and appropriateness of the intervention, (2) benefits of the intervention, (3) challenges of the intervention, and (4) generalization to other routines and activities.
Ease and Appropriateness of the Intervention
Throughout the interview, when asked their thoughts on the individual strategies and what they liked about the intervention, all three mothers commented that the strategies were easy to follow, and the training made them feel empowered to embed the strategies in conversations with their children. Additionally, parents noted that using readily available everyday materials was an advantage. For instance, all mothers mentioned that the photo made it easier to engage with the child during the conversations, and it helped evoke more memories. Hai wrote about photos: “[They are a] good reminder for talking, make it so much easier to find topics and to plan the talking. Kid talks more when looking at photos.”
Furthermore, in response to questions related to the telepractice delivery method, all mothers expressed positive feelings and explained that the use of telepractice was an enabler to accessing the intervention. For example, Hai commented that she appreciated the telepractice delivery method as it helped her and her family stay safe during the COVID-19 pandemic. Lauren stated that an additional benefit to the online delivery of the intervention was that she did not have to find childcare for her oldest daughter. Moreover, Diana and Lauren both explicitly stated that the easiness of scheduling and organization (e.g., being able to cancel sessions if the child was having a bad morning, not having to get self and the child ready) were also benefits to telepractice interventions.
Benefits of the Intervention
Interviewed mothers provided a variety of positive comments about the intervention components. They discussed how learning the strategies made them feel more prepared to support their child’s communication. All mothers described their belief that their child’s language and communication abilities had improved throughout the intervention. Diana stated:
“Since we started doing the descriptive words, you will hear him talking [more] he said ‘something had spots’ and I didn’t even know he knew [the word] spots! So, you know, so he’s describing things more too.”
Additionally, they both mentioned how excited they were when two other adults outside the household, Grayson’s grandma and Lauren’s coworker, noticed an improvement in the child’s communication skills.
Challenges of the Intervention
When asked what they perceived as the biggest challenge of the intervention, all parents mentioned boredom with the same photos and events throughout the sessions as a difficulty. For example, Diana and Lauren both pointed out that the repetitive nature of using the same five topics (and a fixed set of photos associated with the topics) made it difficult to keep their sons engaged towards the end of the intervention. Lauren and Hai also added that that baseline sessions (without photos) were the most difficult. Additionally, all parents talked about how some strategies were more challenging to implement than others (e.g., expanding on the child’s utterances, thinking of WH- questions). For instance, Hai wrote:
“[I] need to think about many things at the same time of talking. Like if my pace is good, if this is a good question, did I focus too much on details instead of the event, not fluent, wrong words, what is the next step.”
Diana also said that although the individual strategies were not difficult it was “difficult to remember it all” and that she “had a hard time thinking of things to say to him.” However, all parents agreed that, with practice, they had gained fluency with the strategy components. In addition, Lauren commented that although the coaching sessions were helpful, she would have preferred a more extended coaching session and possibly seeing herself implement the strategies (i.e., video feedback) to see her areas of improvement.
Generalization to Other Routines and Activities
Finally, the fourth theme reflected in the interviews was the generalization of the strategies to other routines and activities. Hai revealed she had continued taking photos of Elsa during walks to the park and models new language during meals. She also indicated that she had started a new bedtime routine she called “cloud traveling” where she showed Elsa videos from other countries while using the MORE strategies to engage her in conversation. When asked if she planned to use the photos and strategies again in the future, Diana replied,
“Absolutely, we already have. I think I told you, with moving, that we took all the pictures of the new house, and like have sat and talked with him about him [moving]…and now like he every day, every morning, comes in and gets the phone and wants to talk about all the pictures…and I think it’s really helped with the transition here like I feel he’s excited about it…”
She also stated,
“We had a like a zoom party for my niece and nephew last month and I took pictures of him zooming with them and the decorations we had and we talk about their birthday pretty much every day…He usually initiates it too it’s like usually him that wants to talk about it…”
Diana and Lauren also revealed that their husbands were learning the strategies from watching them and implementing them during conversations with the child. Finally, Lauren talked about how her eldest daughter likes to look through her old pictures, an activity David now enjoys with his sister (Table 3).
Discussion
In this study, we investigated the effects of family photos and the combined effects of photos, training, and coaching in the MORE (i.e., model, offer opportunities, respond, and expand) strategies on parents’ use of these communication strategies and the secondary effects on the children’s ability to answer or attempt to answer the WH- questions posed by the parents. Our findings indicate that photos alone resulted in small-moderate increases in the overall frequency of parent communication strategy use and a moderate increase in the number of WH- questions answered for all dyads. Furthermore, parents described spontaneous generalization and maintenance of the target activities and strategies. Our results are promising, albeit limited, given the lack of a functional relation.
As seen in previous parent-implemented telepractice studies (Akemoglu et al., 2020), parent training and coaching via telepractice further increased (from pre-training levels) the level of overall use of strategies for two of the three parents (Dyads 1 and 2) and accounted for additional increases in the average number of WH-questions answered correctly or attempts to answer for two children (Dyads 2 and 3). It should be noted that although the overall strategy used increased, the strategy use breakdown shows decreases in some strategies used by parents in the B2 phase (see Table 2). Possible reasons for this decrease include the implementation of the time delay strategy, which is corroborated by the reduction in the average number of utterances spoken by the parents. Additionally, because the strategies could not be implemented simultaneously, the increase in the use of some of the strategies resulted in a natural reduction in the use of other strategies. Thus, there were differential effects on the types of strategies employed by each parent. For example, in the B + phase, Diana implemented the “ask WH questions” and “respond and expand” strategies at the same average frequency as she had prior to the training. However, she implemented the “binary choices” and “modeling” strategies more often. In contrast, Lauren increased the use of all target strategies. This example speaks to the adaptability of the intervention for each dyad’s conversation style. Similar results were seen in the study by Meadan et al. (2016), where strategies were broken down one at a time to account for this effect.
For Dyad 1, there were no increases in child behavior in the B2 phase, possibly due to a lack of motivation (i.e., boredom) with the same photos by this stage. Additionally, there is a chance of a delayed effect due to Grayson’s language skills. This hypothesis is supported by the comments made by Diana during the social validity interview. She discussed how he was eager to look at photos and talk about them outside of the scheduled sessions and that she saw growth in his language skills. For Dyad 2, upon introduction of the tablet during the B phase, the child engaged in some challenging behavior. For example, during some sessions, he refused to participate and requested to watch videos on the tablet (see data points for sessions 29, 37, and 43 on the graph).
There are several reasons why there were no further increases for Dyad 3 in the B2 phase. First, unlike the other participants, Hai started timing her wait time by looking at a clock and counting exactly 5 s. Second, she provided longer statements while modeling and expanding. Finally, Elsa started asking “why” questions, which Hai answered in detail. All of these actions could explain why there was no measurable change in Hai’s behaviors. Hai’s behavior, in turn, reduced the amount of time in the limited interaction for Elsa to respond and contribute to the conversation.
During the social validity interviews, parents rated the intervention favorably and reported spontaneous generalization of the photographs and target strategies to other routines and family members. Moreover, they provided key insights into which strategies were more challenging to implement, which will inform future studies. These results add to the growing evidence base of the social validity and acceptability of naturalistic interventions (Gevarter et al., 2022; Ousley et al., 2022).
Limitations and Future Research
There are a few limitations within this study. First, although dyads could select from five different events, the participants’ boredom with and preference for specific events may have impacted by the results. These factors could be possible reasons for the variability observed in child behavior. The delayed start of the study due to the COVID-19 pandemic, reduced the amount of time available for the intervention. These time constraints resulted in a limited number of sessions in the B and B2 phases and did not allow us to collect generalization or maintenance data. Given the variability in data, it would have been beneficial to conduct more sessions and examine the long-term effects of the intervention. Additionally, the use of technology posed challenges (e.g., tablet without charge, audio and video hanging and freezing due to unstable Internet connection), resulting in a canceled session and a training session taking longer than expected. Finally, the lead researcher, who was also the coach, served as the main coder and completed the social validity questionnaire via an interview with the parents. This format could have positively skewed the data.
Analyzing our quantitative and qualitative findings together, we can see that conversing while looking at photos of family members and of fun activities, provided the participants with a chance to reminisce about fun times during the lockdowns imposed by the COVID-19 pandemic.
Anecdotally, the conversations appeared to shift from resembling an interview (e.g., the parents asking yes/no questions) to a more natural dialogue with reciprocal back-and-forth conversation exchanges supported by the photos. This type of conversational dialogue has been found to be lacking in conversations between parents and children with ASD (Goldman & DeNigris, 2015).
Moreover, all parents commented positively on the switch to the telepractice format as their children were more comfortable in their natural environment. For the researcher, the switch to telepractice allowed more flexibility when scheduling sessions with the families (i.e., the commute was no longer a consideration). We were also able to reschedule sessions at the last minute if the parent requested it. The benefits of the switch to telepractice are consistent with what has been described in previous studies (Raulston et al., 2019; Simacek et al., 2021).
Future studies should investigate the different active ingredients of packaged NDBI interventions to determine the most effective components of the intervention and, thus, improve the intervention’s efficiency (D’Agostino et al., 2023). Researchers should also investigate the effects of photos and NDBIs on children’s recollection of the events, narrative development, affective joint engagement with the parent, and reminiscing.
Overall, these results suggest that (a) family photos may be an effective visual support strategy to promote communication about past events between parents and children with and at risk for ASD; (b) family photos may naturally cue parents to engage in communication strategies (e.g., providing communication opportunities); and (c) training and coaching are necessary for some parents to implement all the target strategies during conversations.
Data Availability
Raw data for this dataset are not publicly available to protect participants’ privacy.
References
Akamoglu, Y., & Meadan, H. (2019). Parent-implemented communication strategies during storybook reading. Journal of Early Intervention, 41(4), 300–320. https://doi.org/10.1177/1053815119855007
Akamoglu, Y., Muharib, R., & Meadan, H. (2020). A systematic and quality review of parent-implemented language and communication interventions conducted via telepractice. Journal of Behavioral Education., 29(2), 282–316. https://doi.org/10.1007/s10864-01909356-3
Alpert, C. L., & Kaiser, A. P. (1992). Training parents as milieu language teachers. Journal of Early Intervention, 16(1), 31–52. https://doi.org/10.1177/105381519201600104
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.).
Arthur-Kelly, M., Sigafoos, J., Green, V., Mathisen, B., & Arthur-Kelly, R. (2009). Issues in the use of visual supports to promote communication in individuals with autism spectrum disorder. Disability and Rehabilitation, 31(18), 1474–1486. https://doi.org/10.1080/09638280802590629
Bergen, P. V., Salmon, K., Dadds, M. R., & Allen, J. (2009). The effects of mother training in emotion-rich, elaborative reminiscing on children’s shared recall and emotion knowledge. Journal of Cognition and Development, 10(3), 162–187. https://doi.org/10.1080/15248370903155825
Bruinsma, Y. E., Minjarez, M. B., Schreibman, L., & Stahmer, A. C. (2020). Naturalistic developmental behavioral interventions for autism spectrum disorder. Brookes.
Caron, J., Holyfield, C., Light, J., & McNaughton, D. (2018). “What have you been doing?”: Supporting displaced talk through augmentative and alternative communication video visual scene display technology. Perspectives of the ASHA Special Interest Groups, 3(12), 123–135. https://doi.org/10.1044/persp3.SIG12.123
Chiang, H. M., & Lin, Y. H. (2008). Expressive communication of children with autism. Journal of Autism and Developmental Disorders, 38(3), 538–545. https://doi.org/10.1007/s10803-007-0423-z
Chung, M. Y., Meadan, H., Snodgrass, M. R., Hacker, R. E., Sands, M. M., Adams, N. B., & Johnston, S. S. (2020). Assessing the social validity of a telepractice training and coaching intervention. Journal of Behavioral Education, 1–27. https://doi.org/10.1007/s10864-020-09372-8
Cooper, J., Heron, T., & Heward, W. (2020). Applied behavior analysis (3rd ed.). Pearson.
D’Agostino, S. R., Dueñas, A. D., Bravo, A., Tyson, K., Straiton, D., Salvatore, G. L., ... & Pellecchia, M. (2023). Toward deeper understanding and wide-scale implementation of naturalistic developmental behavioral interventions. Autism, 27(1), 253–258. https://doi.org/10.1177/13623613221121427
Daar, J. H., Negrelli, S., & Dixon, M. R. (2015). Derived emergence of WH question–answers in children with autism. Research in Autism Spectrum Disorders, 19, 59–71. https://doi.org/10.1016/j.rasd.2015.06.004
Donato, C., Shane, H. C., & Hemsley, B. (2014). Exploring the feasibility of the visual language in autism program for children in an early intervention group setting: Views of parents, educators, and health professionals. Developmental Neurorehabilitation, 17(2), 115–124. https://doi.org/10.3109/17518423.2014.880526
Gauvreau, A. N. (2015). How was your day in preschool. teaching accurate recall using mobile technologies and visual supports (Publication No. 3723991) [Doctoral dissertation, University of Washington]. ProQuest Dissertations Publishing.
Gevarter, C., Najar, A. M., Flake, J., Tapia-Alvidrez, F., & Lucero, A. (2022). Naturalistic communication training for early intervention providers and Latinx parents of children with signs of autism. Journal of Developmental and Physical Disabilities, 34(1), 147–169. https://doi.org/10.1007/s10803-016-2755-z
Goldman, S., & DeNigris, D. (2015). Parents’ strategies to elicit autobiographical memories in autism spectrum disorders, developmental language disorders and typically developing children. Journal of Autism and Developmental Disorders, 45(5), 1464–1473.
Hall, H. R., & Graff, J. C. (2011). The relationships among adaptive behaviors of children with autism, family support, parenting stress, and coping. Issues in Comprehensive Pediatric Nursing, 34(1), 4–25. https://doi.org/10.3109/01460862.2011.555270
Knutsen, J., Wolfe, A., Burke, B. L., Hepburn, S., Lindgren, S., & Coury, D. (2016). A systematic review of telemedicine in autism spectrum disorders. Review Journal of Autism and Developmental Disorders, 3(4), 330–344. https://doi.org/10.1007/s40489-016-0086-9
Kratochwill, T. R., Hitchcock, J. H., Horner, R. H., Levin, J. R., Odom, S. L., Rindskopf, D. M., & Shadish, W. R. (2013). Single-case intervention research design standards. Remedial and Special Education, 34(1), 26–38. https://doi.org/10.1177/0741932512452794
Kulkofsky, S., & Koh, J. B. K. (2009). Why they reminisce: Caregiver reports of the functions of joint reminiscence in early childhood. Memory, 17(4), 458–470. https://doi.org/10.1080/09658210902729509
Ledford, J. R., & Gast, D. L. (2018). Single case research methodology: Applications in special education and behavioral sciences. Routledge.
Leech, K. A., & Rowe, M. L. (2021). An intervention to increase conversational turns between parents and young children. Journal of Child Language, 48(2), 399–412. https://doi.org/10.1017/S0305000920000252
Leekam, S. R., & Ramsden, C. A. (2006). Dyadic orienting and joint attention in preschool children with autism. Journal of Autism and Developmental Disorders, 36(2), 185–197. https://doi.org/10.1007/s10803-005-0054-1
McDonnell, C. G., Speidel, R., Lawson, M., & Valentino, K. (2021). Reminiscing and autobiographical memory in ASD: Mother–child conversations about emotional events and how preschool-aged children recall the past. Journal of Autism and Developmental Disorders, 51(9), 3085–3097. https://doi.org/10.1007/s10803-020-04770-3
Meadan, H., Snodgrass, M. R., Meyer, L. E., Fisher, K. W., Chung, M. Y., & Halle, J. W. (2016). Internet-based parent-implemented intervention for young children with autism: A pilot study. Journal of Early Intervention, 38(1), 3–23. https://doi.org/10.1177/1053815116630327
Merriam, S. B., & Tisdell, E. J. (2015). Qualitative research: A guide to design and implementation. John Wiley & Sons.
Nelson, K., & Fivush, R. (2004). The emergence of autobiographical memory: A social cultural developmental theory. Psychological Review, 111(2), 486–511. https://doi.org/10.1037/0033-295X.111.2.486
Nigro-Bruzzi, D., & Sturmey, P. (2010). The effects of behavioral skills training on mand training by staff and unprompted vocal mands by children. Journal of Applied Behavior Analysis, 43(4), 757–761. https://doi.org/10.1901/jaba.2010.43-757
Ornstein, P. A., Haden, C. A., & Hedrick, A. M. (2004). Learning to remember: Social-communicative exchanges and the development of children’s memory skills. Developmental Review, 24(4), 374–395. https://doi.org/10.1016/j.dr.2004.08.004
Ousley, C. L., Raulston, T. J., & Gilhuber, C. S. (2022). Incorporating video feedback within a parent-implemented naturalistic developmental behavioral intervention package via telepractice. Topics in Early Childhood Special Education, 42(3), 246–258. https://doi.org/10.1177/02711214221117087
Raulston, T. J., Hieneman, M., Caraway, N., Pennefather, J., & Bhana, N. (2019). Enablers ofbehavioral parent training for families of children with autism spectrum disorder. Journalof Child and Family Studies, 28(3), 693–703. https://doi.org/10.1007/s10826-018-1295-x
Reimers, T. M., & Wacker, D. P. (1988). Parents’ ratings of the acceptability of behavioral treatment recommendations made in an outpatient clinic: A preliminary analysis of the influence of treatment effectiveness. Behavioral Disorders, 14(1), 7–15.
Ruppert, T., Machalicek, W., Hansen, S. G., Raulston, T., & Frantz, R. (2016). Training parents to implement early interventions for children with autism spectrum disorders. In Early Intervention for Young Children with Autism Spectrum Disorder (pp. 219–256). Springer.
Rutherford, M., Baxter, J., Grayson, Z., Johnston, L., & O’Hare, A. (2020). Visual supports at home and in the community for individuals with autism spectrum disorders: A scoping review. Autism, 24(2), 447–469. https://doi.org/10.1177/1362361319871756
Saldaña, J. (2021). The coding manual for qualitative researchers. Sage.
Sarokoff, R. A., & Sturmey, P. (2004). The effects of behavioral skills training on staff implementation of discrete-trial teaching. Journal of Applied Behavior Analysis, 37(4), 535–538. https://doi.org/10.1901/jaba.2004.37-535
Schreibman, L., Dawson, G., Stahmer, A. C., Landa, R., Rogers, S. J., McGee, G. G., Kasari, C., Ingersoll, B., Kaiser, A., Bruinsma, Y., McNerney, E., Wetherby, A., & Halladay, A. (2015). Naturalistic developmental behavioral interventions: Empirically validated treatments for autism spectrum disorder. Journal of Autism and Developmental Disorders, 45(8), 2411–2428. https://doi.org/10.1007/s10803-015-2407-8
Simacek, J., Elmquist, M., Dimian, A. F., & Reichle, J. (2021). Current trends in telehealth applications to deliver social communication interventions for young children with or at risk for autism spectrum disorder. Current Developmental Disorders Reports, 8, 15–23. https://doi.org/10.1007/s40474-020-00214-w
Soto, G., Yu, B., & Kelso, J. (2008). Effectiveness of multifaceted narrative intervention on the stories told by a 12-year-old girl who uses AAC. Augmentative and Alternative Communication, 24(1), 76–87. https://doi.org/10.1080/07434610701740612
Turan, Y., & Meadan, H. (2011). Social validity assessment in early childhood special education. Young Exceptional Children, 14(3), 13–28. https://doi.org/10.1177/1096250611415812
Villi, M. (2012). Visual chitchat: The use of camera phones in visual interpersonal communication. Interactions: Studies in Communication & Culture, 3(1), 39–54. https://doi.org/10.1386/iscc.3.1.39_1
Wainer, A. L., & Ingersoll, B. R. (2015). Increasing access to an ASD imitation intervention via a telehealth parent training program. Journal of Autism and Developmental Disorders, 45(12), 3877–3890. https://doi.org/10.1007/s10803-014-2186-7
Westby, C., & Culatta, B. (2016). Telling tales: Personal event narratives and life stories. Language, Speech, and Hearing Services in Schools, 47(4), 260–282. https://doi.org/10.1044/2016_LSHSS-15-0073
What Works Clearinghouse. (2020). What works clearinghouse procedures and standards handbook, version 4.1. U.S. Department of education, institute of education sciences, national center for education evaluation and regional assistance (NCEE). https://ies.ed.gov/ncee/wwc/Handbooks
Wolf, M. M. (1978). Social validity: The case for subjective measurement or how applied behavior analysis is finding its heart. Journal of Applied Behavior Analysis, 11(2), 203–214. https://doi.org/10.1901/jaba.1978.11-203
Yang, X. (2018). Impact of different photo conditions on social interaction between grandparents and grandchildren with disabilities [Doctoral dissertation, University of Washington]. https://digital.lib.washington.edu/researchworks/handle/1773/43363
Acknowledgements
NB thanks Dr. David McNaughton for his feedback on the initial versions of this manuscript. We are grateful to all the families who participated in this study.
Funding
Research participants were provided subject honorarium through funding provided to the second author from the Penn State College of Education.
Author information
Authors and Affiliations
Contributions
NB: conceptualized and executed the study, conducted data analysis, and wrote the paper. TJR: assisted with study conceptualization and funding support, supervised and provided NB with training, assisted with data analysis, and provided feedback on manuscript drafts. CO: Assisted with coding, data analysis, and editing of the manuscript. AB: Assisted with coding and data interpretation.
Corresponding author
Ethics declarations
Ethics Approval
The Institutional Review Board at Penn State University provided ethical approval for this study.
Informed Consent
Prior to the beginning of the study, adult participants were provided with detailed information about the study, including risks, benefits, privacy, and their right to withdraw. Participants only proceeded with the study after providing their signed consent.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Bhana, N., Raulston, T.J., Ousley, C. et al. Photographs and Parent Training to Support Conversations about Past Events between Caregivers and Children with Autism. Adv Neurodev Disord 8, 311–323 (2024). https://doi.org/10.1007/s41252-023-00333-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41252-023-00333-6