
Abstract
Purpose
The positive end-expiratory pressure (PEEP) level with best respiratory system compliance (Crs) is frequently used for PEEP selection in acute respiratory distress syndrome (ARDS) patients. On occasion, two similar best Crs (where the difference between the Crs of two PEEP levels is < 1 ml/cm H2O) may be identified during decremental PEEP titration. Selecting PEEP under such conditions is challenging. The aim of this study was to provide supplementary rationale for PEEP selection by assessing the global and regional ventilation distributions between two PEEP levels in this situation.
Methods
Eight ARDS cases with similar best Crs at two different PEEP levels were analyzed using examination-specific electrical impedance tomography (EIT) measures and airway stress index (SIaw). Five Crs were measured at PEEP values of 25 cm H2O (PEEP25), 20 cm H2O (PEEP20), 15 cm H2O (PEEPH), 11 cm H2O (PEEPI), and 7 cm H2O (PEEPL). The higher PEEP value of the two PEEPs with similar best Crs was designated as PEEPupper, while the lower designated as PEEPlower.
Results
PEEPH and PEEPI shared the best Crs in two cases, while similar Crs was found at PEEPI and PEEPL in the remaining six cases. SIaw was higher with PEEPupper as compared to PEEPlower (1.06 ± 0.10 versus 0.99 ± 0.09, p = 0.05). Proportion of lung hyperdistension was significantly higher with PEEPupper than PEEPlower (7.0 ± 5.1% versus 0.3 ± 0.5%, p = 0.0002). In contrast, proportion of recruitable lung collapse was higher with PEEPlower than PEEPupper (18.6 ± 4.4% versus 5.9 ± 3.7%, p < 0.0001). Cyclic alveolar collapse and reopening during tidal breathing was higher at PEEPlower than PEEPupper (34.4 ± 19.3% versus 16.0 ± 9.1%, p = 0.046). The intratidal gas distribution (ITV) index was also significantly higher at PEEPlower than PEEPupper (2.6 ± 1.3 versus 1.8 ± 0.7, p = 0.042).
Conclusions
PEEPupper is a rational selection in ARDS cases with two similar best Crs. EIT provides additional information for the selection of PEEP in such circumstances.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Background
Tidal volume and positive end-expiratory pressure (PEEP) are two cardinal parameters in ventilator therapy of acute respiratory distress syndrome (ARDS) patients. Though the use of low tidal volume is well established, determining the optimal PEEP for selection remains challenging. A few available indicators are useful for selecting PEEP [1, 2], with the best respiratory system compliance (Crs) being a popular option [3]. The best Crs can usually be selected during the PEEP titration process, with or without recruitment maneuvers [3,4,5]. Similar best Crs (where the difference between the Crs of two PEEP levels < 1 cm H2O) can be identified at several PEEP levels sometimes. Selecting PEEP under such circumstances is challenging [3, 4]. A higher PEEP with addition of 2 cm H2O was adopted in the Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial (ART) trial [3], while another trial selected a lower PEEP [4] but indicated no clear reasoning behind this selection. Electrical impedance tomography (EIT) is a noninvasive imaging technique that has the potential to provide new information for the ventilator management of ARDS patients [6]. Several examination-specific EIT measures have been developed to estimate the collapse/hyperdistension or recruitment/cyclic alveolar collapse proportion [7,8,9]. These EIT measures, which have been successfully applied to several animal and human studies, could facilitate the optimal selection of PEEP [5, 8, 10,11,12].
EIT has been employed at our hospital for PEEP choice in selected ARDS patients since 2014 and we have published a brief article discussing the issue of best PEEP level and recruitable lung volume [13]. We have also identified a few patients with two similar best Crs during decremental PEEP titration within the same study population. The aim of this study was to apply examination-specific EIT measures for regional ventilation analysis in ARDS patients with two similar Crs but different PEEP levels. In this study, the airway stress index (SIaw) [14, 15] was also calculated based on the shape of the airway pressure curve as a constant flow was used, and the lung volume was measured using the nitrogen washin-washout (NWI-WO) technique [16]. Our objective was to enable a rational selection of PEEP using examination-specific EIT measures and SIaw.
2 Methods
2.1 Study Population
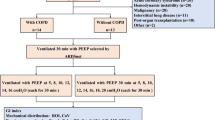
In this study, ventilated patients over 18 years who fulfilled the diagnostic criteria of ARDS with a FiO2 requirement of ≥ 50% at our intensive care unit and PEEP > 8 cm H2O were screened for suitability between October 2014 and Febuary 2016. The exclusion criteria included (1) patients with metallic materials in the body (including wires, pins or implanted electrical devices); (2) patients with cutaneous diseases which prohibited the application of electrode leads to the body; (3) severe chronic obstructive pulmonary diseases or idiopathic pulmonary fibrosis; (4) hemodynamically unstable; (5) proved barotrauma (including pneumothorax or pneumomediastinum or subcutaneous emphysema); (6) pregnancy; (7) terminal malignancy or evidently irreversible diseases; (8) the use of extracorporeal membrane oxygenation (ECMO); (9) patients or family members who refused to participate in the study. The ethics committee of our hospital had approved this study (NCKUH-10403009). All patients who fulfilled the diagnostic criteria of ARDS received standard low tidal volume ventilator therapy (6–8 ml/Kg ideal body weight).
2.2 Instrument and Measurement
Air flow and airway pressure were measured using a pneumotachograph (PN 155,362, Hamilton Medical, Bonaduz, Switzerland) and differential pressure transducers (P/N 113,252, Model 1110A, Hans Rudolph, Shawnee, KS, USA), respectively. The flow sensor was positioned between the endotracheal tube and Y-piece of the ventilator. Tidal volume was calculated by integrating the flow signal. All signals were sampled and digitized at 100 Hz, and the data were stored in a data-acquisition system (AcqKnowledge, Biopac MP150, Goleta, CA, USA). End-expiratory lung volume (EELV) was measured using the NWI-WO technique available via the GE Carestation ventilator (GE Healthcare, Chicago, Ill, USA) [16]. The airway plateau pressure 1 s after airway occlusion was denoted by Ppl. PEEPt represented the total PEEP obtained with end-expiratory airway occlusion. We calculated △P = Ppl − PEEPt, while Crs was calculated to equal the tidal volume (Vt)/△P.
In this study, we employed a commercial EIT monitor (PulmoVista 500, Dräger Medical GmbH, Lubeck, Germany). PulmoVista 500 displays functional EIT images (i.e. relative impedance changes), which includes measurements of the tidal ventilation and changes in the end-expiratory lung impedance (EELI). The EIT data was registered at 20 Hz, low-pass filtered (35 per minute), and stored for offline analysis during the study.
2.3 Lung Recruitment Protocol
We standardized the lung volume history using the extended sigh method for alveolar recruitment [17] prior to performing the lung recruitment assessments. PEEP was sequentially increased from baseline to 15, 20, and 25 cm H2O (every 30 s, from the baseline PEEP to a PEEP level of 25 cm H2O, twice). Vt was reduced by 25% from the previous baseline Vt during the incremental phase, while it was increased by 25% during the decremental phase. The upper limit of the peak airway pressure during this recruitment maneuver was 50 cm H2O. Ppl was determined at a PEEP of 25 cm H2O (PEEP25) and 20 cm H2O (PEEP20) during the second recruitment maneuver and following EELV determination using the NWI-WO method at a PEEPH, PEEPI, and PEEPL of 15 cm H2O, 11 cm H2O, and 7 cm H2O, respectively. The recruited lung volume (Vrec) was calculated as the difference between the EELVs at PEEPH and PEEPL or PEEPI and PEEPL, after subtracting the minimal deformable lung volume that was obtained by multiplying the Crs at PEEPL with the PEEP difference [18]. The arterial blood gas was determined at the end of PEEPH, PEEPI, and PEEPL, with the EIT images simultaneously recorded.
2.4 Stress Index Calculations from the Airway Pressure–Time Curve Profile Under Constant Flow
The equation used to fit the airway pressure–time (Paw-t) curve is given by airway pressure (Paw) = a * time (second)b + c, where coefficient a represents the slope of the Paw-t relationship, and the coefficient c is the value of Paw at beginning (time0) and dimentionless coefficient b (SIaw) depicts the shape of the Paw-t curve. These coefficients were obtained using the Levenberg–Marquardt algorithm [15]. The shape of the Paw-t curve could indicate the tidal recruitment and hyperinflation. Ten tidal breaths were averaged and only the constant flow section was selected to ensure a good flow and airway pressure signal. We added 50 ms offsets at both ends of the constant flow section to further reduce its width [14, 15]. The above-detailed equation was also used to fit the selected time interval of the Paw-t curve. The three calculated SIaws were averaged at each PEEP level.
2.5 Proportion of Recruitable Lung Collapse and Hyperdistension at Different PEEPs
The method proposed by Costa et al. [7] was used to calculate the degree of recruitable lung collapse and hyperdistension during decremental PEEP titration. The individual pixel impedance variations (△Z) between Ppl and PEEPt were computed. Pixel impedance compliance was computed as △Z/△P. The impedance compliance at five PEEP levels was determined for each pixel, and the amount of collapse or hyperdistension in the individual pixels was summed to estimate the corresponding percentages. No collapse or hyperdistension are observed at the highest and lowest PEEP levels, respectively.
2.6 Cyclic Alveolar Collapse and Reopening During Tidal Breathing at Different PEEPs
The method proposed by Liu et al. [8] was used to estimate the cyclic alveolar collapse and reopening during tidal breathing at various PEEP levels. The lung regions were identified first, which at end-expiration included all pixel values > 25% of the maximum in the image. The lung regions corresponding to tidal breathing included all pixel values > 20% of the maximum in the tidal image. Regions ventilated during tidal breathing but not at end-expiration were associated with cyclic alveolar collapse and reopening. The degree of cyclic alveolar collapse and reopening was expressed in percentage values, which were calculated by dividing the absolute number of pixels associated with cyclic alveolar collapse and reopening by the total number of lung pixels during tidal breathing.
2.7 Heterogeneity of Regional Lung Ventilation Distribution During Inspiration Using Intratidal Gas Distribution (ITV)
The method developed by Löwhagen et al. [9] was used to estimate the ITV. The inspiratory portion of the global tidal curve was divided into eight isovolumetric sections to calculate the ITV. The volume signal was first resampled and the isovolume points were calculated. Interpolation was used to obtain the corresponding EIT signals, which were divided into the nondependent (nondep) and dependent (dep) parts. The ratios of Vtnondep/Vtdep in the eight equal volume parts were subsequently averaged to obtain the ITV index [5, 10, 19]. An ITV index of one indicated an equal regional ventilation distribution. An ITV index of less than one may indicate overdistension. A flow chart describing the steps used in ITV calculation could be found in the supplement material.
2.8 Statistical Analysis
Data are presented as mean ± SD. Friedman’s analysis of variance for repeated measures was used to compare the ∆P, Vt, EELV, and arterial blood gas at the PEEPH, PEEPI, and PEEPL levels. The independent samples t-test was used to compare two groups of normally distributed variables, while the Mann–Whitney U test was used for variables with non-normal distributions. All tests were two-sided, and a p value < 0.05 was considered statistically significant. All analyses were performed using Prism software, version 5 (GraphPad Software, San Diego, CA, USA).
3 Results
3.1 Study Population
During the study period, fifty-six cases were screened and 25 patients who met the Berlin’s criteria of ARDS entered our study. The male to female ratio is 20/5 and their mean age is 61.1 ± 16.3 years. Of the 25 patients receiving EIT and EELV measurement, two cases were terminated earlier because the measured lung volume was paradoxically higher under lower PEEP. Among the 23 patients who met the Berlin’s criteria of ARDS received EIT and EELV measurement following our standarad recruitment protocol. Two similar Crs was found during decremental PEEP titration in 8 patients. The hospital mortality rate of these 8 patients was 25%. Patients’ characteristics, outcomes and respective Crs at PEEPH, PEEPI, PEEPL levels are shown in Table 1. Respiratory parameters over 5 PEEP levels, measured EELV, arterial blood gases and Vrec are shown in Table 2. For the two PEEP levels with similar Crs, the higher PEEP was designated as PEEPupper, the lower PEEP was designated as PEEPlower.
3.2 Airway Stress Index (SIaw) Between PEEPupper and PEEPlower
For PEEPupper, the SIaw ranged from 0.90 to 1.25 and SIaw was higher than 1.10 in two cases. For PEEPlower, the SIaw ranged from 0.86 to 1.14 and SIaw was higher than 1.10 in one case and lower than 0.90 in one case. The SIaw of PEEPupper was relatively higher than that of PEEPlower (Fig. 1a).

Airway stress index and examination-specific EIT measures between two PEEPs with similar best Crs. SIaw: airway stress index. ITV index: intratidal gas distribution index. PEEPupper: higher one of the two similar PEEPs. PEEPlower: lower one of the two similar PEEPs. a p = 0.05 b p = 0.0002 c p < 0.0001 d p = 0.046 e p = 0.042. △P driving pressure, Ppl-PEEPt. The difference between airway plateau pressure and total PEEP, △Z impedance variations. Impedance change during tidal ventilation, Crs static respiratory system compliance, EELV end-expiratory lung volume. Lung volume measured using nitrogen washin-washout method, ITV intratidal volume distribution. Quantitative measure of ventilation distribution using electrial impedance tomography, NWI-WO nitrogen washin-washout. An auxillary function for lung volume measurement in GE Carestation ventilator, Paw-t curve: airway pressure–time curve recorded at airway opeing, PEEP25 Actual total PEEP level with ventilator PEEP set at 25 cmH2O, PEEP20 Actual total PEEP level with ventilator PEEP set at 20 cmH2O, PEEPH Actual total PEEP level with ventilator PEEP set at 15 cmH2O, PEEPI Actual total PEEP level with ventilator PEEP set at 11 cmH2O, PEEPL Actual total PEEP level with ventilator PEEP set at 7 cmH2O, PEEPlower The lower PEEP in cases with two PEEPs of similar best Crs, PEEPupper The higher PEEP in cases with two PEEPs of similar best Crs, SIaw Airway stress index. Namely the dimensionless coefficient b in airway pressure–time curve equation, (Paw) = a * time (second)b + c, Vrec recruited lung volume. Calculated as the difference between the EELVs at PEEPH and PEEPL or PEEPI and PEEPL, after subtracting the minimal deformable lung volume that was obtained by multiplying the Crs at PEEPL with the PEEP difference
3.3 Recruitable Lung Collapse and Hyperdistension
Considering the PEEPupper and PEEPlower levels with similar Crs, PEEPlower was associated with minimal hyperdistension (0%–1.5%), while PEEPupper was associated with significantly higher hyperdistension (1.7%–14.1%). In contrast, PEEPlower and PEEPupper were associated with a higher (9.8%–23.6%) and much lower recruitable lung collapse (0.7%–11.0%), respectively (Fig. 1b, c).
3.4 Tidal Recruitment/Derecruitment Between PEEPupper and PEEPlower
Tidal recruitment/decruitment was associated with both PEEPupper and PEEPlower, which ranged from 10.2% to 63.8% for PEEPlower and 6.6% to 27.1% for PEEPupper. A significantly higher tidal recruitment/derecruitment was associated with PEEPlower as compared to PEEPupper (Fig. 1d).
3.5 Intratidal Gas Distribution (ITV) Index Between PEEPupper and PEEPlower
ITV index ranged from 1.2 to 5.5 in PEEPlower and 0.9 to 2.6 in PEEPupper (Fig. 1e). The ITV index was significantly higher with PEEPlower, implicating more heterogeneous ventilation distribution. The ITV index of PEEPupper was less than 1 in one case, suggesting potential overdistention occurred if PEEPupper + 2 cmH2O was selected. The PEEPupper in this case was 14.5 cmH2O.
4 Discussion
In this study, the two best Crs had significantly different ventilation distributions, under similar ventilator settings and different PEEP levels. The main findings were as follows: (1) A significantly higher proportion of recruitable collapse and tidal recruit-derecruit were linked to PEEPlower, while PEEPupper was associated with a higher proportion of hyperdistension. (2) PEEPupper might be a more appropriate selection when considering ventilation homogeneity and recruitable collapse. However, lung overdistension may be an issue in case when PEEPupper is in PEEPH range. The use of examination-specific EIT measures in these patients provided important information which may allow personalized choice of PEEP in ARDS patients.
The choice of the PEEP level in ARDS patients has always been debated. In recent years, individualized titration has been the preferred method due to the heterogeneity observed in ARDS patients [1]. A wide variation in the ventilation distribution was observed in our patients despite PEEP selection based on the best Crs, which is consistent with the current viewpoint. SIaw, which describes the time course of the airway pressure profile under constant flow conditions, is an established parameter for the appropriate selection of PEEP in ARDS patients [14]. SIaw > 1.10 and SIaw < 0.90 indicated tendencies towards lung hyperdistension and collapse, respectively [15]. SIaw tends to be higher in PEEPupper and lower in PEEPlower. SIaw was not observed in the recommended range (0.90 < SIaw < 1.10) in two PEEPupper cases and two PEEPlower cases. Thus, this indicates that either best Crs did not always ensure a safe SIaw.
Recruitable lung collapse and lung hyperdistension are two undesirable conditions that may cause lung injury [20]. The method proposed by Costa et al. [7] was used to quantitatively evaluate the above-mentioned conditions. Selecting the best PEEP level with minimal lung collapse and hyperdistension is challenging due to their concomitant presence in the lung. A collapse level of up to 10–15% is an acceptable safety margin with minimal hyperdistension, which is the more undesirable condition [7, 12]. In this study, we found that 7 cases had a recruitable lung collapse above 10% and 6 cases had a recruitable lung collapse above 15% when PEEPlower was selected. In contrast, only 1 case had a recruitable lung collapse above 10% and none above 15% when PEEPupper was selected. The tidal recruited/derecruited percentage, which was calculated using the method proposed by Liu et al. [8], was significantly higher at PEEPlower. Thus, the present evidence from the EIT analysis suggests that the selection of PEEPupper may be more appropriate when considering the level of recruitable alveolar collapse. However, lung hyperdistension remains a concern, as it is understandably higher with PEEPupper. Though lung hyperdistension is minimal with PEEPlower, 3 of our cases would have an EIT-derived hyperdistension greater than 10% with PEEPupper. The level of lung hyperdistension obtained from EIT has been known to overestimate the actual hyperdistension from the CT images [7]. Thus, we additionally used the ITV index to determine the appropriate PEEP level. ITV index is an useful indicator of ventilation homogeneity. An ITV index of one indicates a homogeneous tidal volume distribution in the non-dependent and dependent lung regions. ITV index was higher at PEEPlower than that at PEEPupper, suggesting better ventilation homogeneity with PEEPupper. However, ITV index of one patient was < 1 when PEEPupper was selected, which implicated overdistention might have occurred when PEEPupper + 2 cm H2O was applied.
Our study has several limitations. First, we investigated a small sample size of patients in this study. However, these are all ARDS patients and our physiological recordings combined with EIT analysis provided significant relevant information with respect to the two similar Crs levels. These information provided additional clues in the selection of PEEP. Second, we used a limited pressure range for the recruitment maneuvers. A small fraction of lung recruitment might require higher pressures to open [21]. The EIT analysis might have differed for different recruitment maneuvers. Third, we only employed EIT and physiological measurements and did not perform a chest CT scan, which is a gold standard for assessing the collapsed and recruitable lung tissue. Furthermore, EIT measures were obtained only for a portion of the lung region. However, the reliability of EIT analysis techniques has been confirmed [6] and the results of present study were in good agreement with physiological reasoning. EIT provides valuable information on the regional ventilation, which could potentially aid our decisions in ventilator therapy [22].
In conclusion, although PEEPupper is preferred for ARDS patients with two similar best Crs but different PEEP levels from our EIT study, the use of EIT clearly revealed the heterogeneous ventilation distribution in individual ARDS patient under two similar best Crs. We recommend addition of examination-specific EIT measures in this difficult-to decision circumstances to select the most appropriate PEEP which should be of value in our ventilatory management of individual ARDS patient.
References
Gattinoni, L., et al. (2017). Positive end-expiratory pressure: How to set it at the individual level. Annals of Translational Medicine, 5(14), 288.
Gattinoni, L., Carlesso, E., & Cressoni, M. (2015). Selecting the “right” positive end-expiratory pressure level. Current Opinion in Critical Care, 21(1), 50–57.
Cavalcanti, A. B., et al. (2017). Effect of lung recruitment and titrated positive end-expiratory pressure (peep) vs. low peep on mortality in patients with acute respiratory distress syndrome: A randomized clinical trial. The Journal of the American Medical Associationc, 318(14), 1335–1345.
Pintado, M. C., et al. (2013). Individualized PEEP setting in subjects with ARDS: A randomized controlled pilot study. Respiratory Care, 58(9), 1416–1423.
Blankman, P., et al. (2014). Detection of “best” positive end-expiratory pressure derived from electrical impedance tomography parameters during a decremental positive end-expiratory pressure trial. Critical Care, 18(3), R95.
Frerichs, I., et al. (2017). Chest electrical impedance tomography examination, data analysis, terminology, clinical use and recommendations: Consensus statement of the Translational EIT development study group. Thorax, 72(1), 83–93.
Costa, E. L., et al. (2009). Bedside estimation of recruitable alveolar collapse and hyperdistension by electrical impedance tomography. Intensive Care Medicine, 35(6), 1132–1137.
Liu, S., et al. (2016). Identification of regional overdistension, recruitment and cyclic alveolar collapse with electrical impedance tomography in an experimental ARDS model. Critical Care, 20(1), 119.
Lowhagen, K., Lundin, S., & Stenqvist, O. (2010). Regional intratidal gas distribution in acute lung injury and acute respiratory distress syndrome assessed by electric impedance tomography. Minerva Anestesiologica, 76(12), 1024–1035.
Mauri, T., et al. (2015). Effects of sigh on regional lung strain and ventilation heterogeneity in acute respiratory failure patients undergoing assisted mechanical ventilation. Critical Care Medicine, 43(9), 1823–1831.
Mauri, T., et al. (2016). Bedside assessment of the effects of positive end-expiratory pressure on lung inflation and recruitment by the helium dilution technique and electrical impedance tomography. Intensive Care Medicine, 42(10), 1576–1587.
Franchineau, G., et al. (2017). Bedside contribution of electrical impedance tomography to setting positive end-expiratory pressure for extracorporeal membrane oxygenation-treated patients with severe acute respiratory distress syndrome. American Journal of Respiratory and Critical Care Medicine, 196(4), 447–457.
Su, P. L., et al. (2018). Positive end-expiratory pressure selection based on best respiratory system compliance or collapse/hyperdistension curves in patients with acute respiratory distress syndrome: Lack of correlation with alveolar recruitment. Intensive Care Medicine, 44(3), 389–391.
Terragni, P. P., et al. (2013). Accuracy of plateau pressure and stress index to identify injurious ventilation in patients with acute respiratory distress syndrome. Anesthesiology, 119(4), 880–889.
Grasso, S., et al. (2004). Airway pressure-time curve profile (stress index) detects tidal recruitment/hyperinflation in experimental acute lung injury. Critical Care Medicine, 32(4), 1018–1027.
Olegard, C., et al. (2005). Estimation of functional residual capacity at the bedside using standard monitoring equipment: A modified nitrogen washout/washin technique requiring a small change of the inspired oxygen fraction. Anesthesia and Analgesia, 101(1), 206–212.
Huh, J. W., et al. (2009). Efficacy of positive end-expiratory pressure titration after the alveolar recruitment manoeuvre in patients with acute respiratory distress syndrome. Critical Care, 13(1), R22.
Dellamonica, J., et al. (2011). PEEP-induced changes in lung volume in acute respiratory distress syndrome. Two methods to estimate alveolar recruitment. Intensive Care Medicine, 37(10), 1595–1604.
Blankman, P., et al. (2016). Detection of optimal PEEP for equal distribution of tidal volume by volumetric capnography and electrical impedance tomography during decreasing levels of PEEP in post cardiac-surgery patients. British Journal of Anaesthesia, 116(6), 862–869.
Suzumura, E. A., Amato, M. B. P., & Cavalcanti, A. B. (2016). Understanding recruitment maneuvers. Intensive Care Medicine, 42(5), 908–911.
Borges, J. B., et al. (2006). Reversibility of lung collapse and hypoxemia in early acute respiratory distress syndrome. American Journal of Respiratory and Critical Care Medicine, 174(3), 268–278.
Yoshida, T., et al. (2019). Regional ventilation displayed by electrical impedance tomography as an incentive to decrease PEEP. American Journal of Respiratory and Critical Care Medicine, 200(7), 933–937.
Funding
This study was supported by grants from Ministry of Science and Technology (108-2314-B006-069) and National Cheng Kung University Hospital (NCKUH-10403009).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethical approval
Protocol approved by the Research Ethics Committee, National Cheng Kung University Hospital (NCKUH-10403009).
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Su, PL., Lin, WC., Ko, YF. et al. Electrical Impedance Tomography Analysis Between Two Similar Respiratory System Compliance During Decremetal PEEP Titration in ARDS Patients. J. Med. Biol. Eng. 41, 888–894 (2021). https://doi.org/10.1007/s40846-021-00668-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40846-021-00668-2