
Abstract
Background
Telavancin—a lipoglycopeptide antibacterial agent active against Gram-positive pathogens including methicillin-sensitive and -resistant Staphylococcus aureus (MRSA)—is approved in the USA for once-daily intravenous use. This registry study captured patient characteristics, prescribing patterns, and treatment outcomes associated with telavancin use in real-world clinical practice.
Objective
This prospective, multicenter, observational study will characterize current real-world practice patterns for the use of telavancin in the USA by describing demographic and clinical conditions, examining the process of care and rationale for use, and describing the clinical effectiveness and selected safety outcomes among patients treated with telavancin.
Methods
The Telavancin Observational Use Registry (TOUR™) is an observational multicenter registry study. Clinical data—including patient demographics, pathogens, telavancin dosing and treatment duration, and adverse events—along with investigators’ assessments of outcome, were collected through retrospective medical chart review.
Results
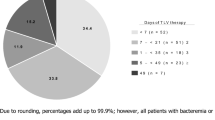
Data from 1063 patients were collected from 45 US sites. Of these patients, 29.4% were ≥ 65 years of age [mean age ± standard deviation, 55.2 ± 15.4 years; median age (interquartile range), 57.0 (46.0–66.0)], 53.4% were male, and 83.4% were White. The primary infections in these patients included complicated skin and skin-structure infection (48.7%), bone and joint infections (27.4%), bacteremia and endocarditis (14.2%), and lower respiratory tract infections (8.5%). The predominant pathogen identified was MRSA (37.7%). The mean telavancin dose and duration of treatment were 741.7 ± 194.3 mg and 17 ± 17 days, respectively. Of the 964 (90.7%) patients for whom an end-of-treatment assessment was available, 77.7% had a positive clinical response, 10.1% failed treatment, and 12.2% had indeterminate outcomes.
Conclusions
Real-world data collected from the TOUR study show once-daily telavancin is being used for the treatment of a variety of Gram-positive infections with generally positive clinical outcomes.
Similar content being viewed by others

The Telavancin Observational Use Registry (TOUR™) recorded characteristics and outcomes of telavancin use in clinical practice. |
The real-world results from TOUR™ suggest telavancin is a potential treatment option for a variety of infections due to Gram-positive pathogens. |
1 Introduction
Gram-positive infections due to Staphylococcus aureus (S. aureus) include hospital-acquired and ventilator-associated bacterial pneumonia (HABP/VABP), complicated skin and skin structure infections (cSSSI), osteomyelitis and septic arthritis, and bacteremia [1]. Serious infections caused by Gram-positive pathogens are commonly treated with glycopeptides, primarily vancomycin, or various β-lactam antibiotics. Estimated glycopeptide use in hospitalized patients in 2012 was greater than penicillin or first-/second-generation cephalosporin but comparable to β-lactam/β-lactamase inhibitor combinations [2]. Vancomycin is often dosed multiple times daily and generally requires therapeutic drug monitoring. However, vancomycin treatment is not always effective; for example, Wunderink reported clinical cure of nosocomial pneumonia following vancomycin treatment in 59/136 patients with S. aureus (43.4%) and 22/62 (35.5%) patients with methicillin-resistant S. aureus (MRSA) [3]. Furthermore, some S. aureus isolates exhibit reduced vancomycin susceptibility [4, 5]. Alternative therapies are needed for challenging S. aureus infections.
Telavancin is a once-daily, parenterally administered, optimized lipoglycopeptide antibacterial agent derived from vancomycin, with activity against susceptible Gram-positive pathogens [6]. Telavancin has potent in vitro activity against Gram-positive bacteria including methicillin-susceptible S. aureus (MSSA), MRSA, vancomycin-intermediate S. aureus (VISA), heterogenous VISA, and some S. aureus isolates nonsusceptible to linezolid and daptomycin [7,8,9]. Telavancin has 16- to 32-fold greater activity against MRSA compared with vancomycin [10]. Telavancin demonstrated high cure rates in patients with cSSSI and represents an effective alternative to vancomycin for treatment of monomicrobial S. aureus HABP/VABP, especially in patients with complications such as age > 65 years, mechanical ventilation, and isolates with vancomycin minimum inhibitory concentrations ≥ 1 µg/mL [11, 12]. In limited numbers of patients with cSSSI or HABP/VABP with concomitant bacteremia, telavancin efficacy was comparable to vancomycin [13]. Additionally, in randomized controlled trials, telavancin treatment resulted in higher cure and comparable survival rates relative to vancomycin in patients with Gram-positive pneumonia due to S. aureus [11, 14].
In the USA, telavancin is approved in adults for treatment of cSSSI caused by susceptible Gram-positive pathogens and for HABP/VABP when alternative treatments are unsuitable [6]. In Canada and Russia, telavancin is approved for treatment of patients with cSSSI and HABP/VABP caused by Gram-positive pathogens [15, 16]. Telavancin is approved in Israel for treatment of adults with nosocomial pneumonia, including ventilator-associated pneumonia, known or suspected to be caused by MRSA, where other alternatives are not suitable [17]. In the EU, telavancin was approved for treatment of nosocomial pneumonia, known or believed to be caused by MRSA, when alternative medicines are unsuitable; however, telavancin was voluntarily withdrawn from the EU market by the sponsor in March 2018 due to limited use of the product [18]. Approved dosing for telavancin for all indications is 10 mg/kg intravenously with adjustments for creatinine clearance (CrCl) described in the product information (PI). The Telavancin Observational Use Registry (TOUR™) was conducted to record population characteristics, prescription information, and real-world clinical outcomes of patients with Gram-positive infections treated with telavancin. Findings from TOUR will improve understanding of US patterns of care for telavancin-treated patients in clinical practice.
2 Methods
2.1 Study Design
TOUR was a multicenter, retrospective, observational registry study conducted at 45 US hospitals or outpatient infusion centers with clinicians routinely involved in care and treatment of bacterial infections between January 2015 and March 2017. The protocol was amended from a prospective to a retrospective design in November 2015; all previously enrolled patients were included. As such, the inclusion/exclusion criteria were limited. At the discretion of the treating physician, any patient who received at least one dose of telavancin as part of clinical care from 1 January 2015 onward was eligible for inclusion in the study. Patients who participated in an interventional research study or clinical trial involving telavancin after 1 January 2015 were excluded. All treatment decisions and clinical assessments were at the treating physician’s discretion and not mandated by registry study design or protocol. Data were obtained through retrospective medical chart review; sites were queried after completion of enrollment to resolve missing or unclear entries. Missing data were not imputed. Registry study management performed by Pharmaceutical Product Development, LLC (Wilmington, NC, USA) included recruitment, training, and management of study sites, as well as electronic data capture system and data management. Enrollment was planned for approximately 1000 patients from 50–60 inpatient or outpatient sites that were routinely involved in the treatment of patients with Gram-positive infections.
The registry study was conducted in compliance with the International Society for Pharmacoepidemiology Guidelines for Good Pharmacoepidemiology Practice, the Declaration of Helsinki and its amendments, and the Health Insurance Portability and Accountability Act (HIPAA) of 1996. Institutional Review Board waiver or approval was obtained consistent with local regulations prior to patient data collection at each site. As informed consent was not obtained, only de-identified information was collected in accordance with HIPAA Privacy Rule Section 164.514.
2.2 Patient Populations
Patients who received one or more dose of telavancin on or after 1 January 2015 were eligible for inclusion; individuals who participated in any other telavancin clinical study or trial were excluded. Population size was based on recruitment of patients over a planned period of approximately 3 years.
2.3 Data Collection and Analysis
Data of interest were obtained by medical chart review and entered into electronic case report forms by qualified personnel at each site ≥ 30 days after the last dose of telavancin was administered (see Supplementary Table 1). Clinical responses at end of treatment (EOT) were analyzed in all patients and patients with available assessment at EOT, and categorized as positive, indeterminate due to insufficient information, or failure. Positive clinical responses included patients cured or improved to step-down therapy. Cure was defined as resolution of signs and symptoms of infection and/or no need for additional antibiotic therapy, or clearance of infection as determined by negative culture. Improvement to step-down therapy was defined as partial resolution of clinical signs and symptoms of infection and/or need for additional antibiotic therapy. Failure was defined as inadequate response to therapy, where individuals were resistant to treatment, showed worsening symptoms, or demonstrated new or recurrent signs and symptoms; need to change antibiotic therapy before planned completion of telavancin treatment; or positive culture at EOT.
If a patient died, day of death was recorded as number of days after initiation of telavancin therapy. Renal function was assessed using serum creatinine values obtained ≤ 15 days prior to telavancin therapy (baseline) and at EOT. Use of concomitant antibiotics and potentially nephrotoxic concomitant medications from 2 days prior to telavancin therapy to 2 days after EOT were recorded. Collection of safety data was limited to renal adverse events (AEs), additional AEs leading to discontinuation, and events with fatal outcomes. Renal AEs were defined as any untoward medical occurrence related to the kidney, urinary tract, or renal function per the investigator’s discretion. Analysis was performed using SAS® version 9.2 or higher (SAS Institute, Cary, NC, USA). All AE and medical history verbatim terms were recorded and coded using the Medical Dictionary for Regulatory Activities (MedDRA); concomitant medications were coded using the World Health Organization Drug Dictionary. No formal hypothesis or statistical significance testing was planned. Descriptive analyses were performed and reported as mean, median, interquartile range (IQR), number, and proportion of the total population where appropriate.
3 Results
3.1 Patient Disposition, Demographics, Medical History, and Disease Characteristics
TOUR enrolled 1063 patients from 45 US sites (Table 1), of whom 964 (90.7%) had available assessments at EOT and 39/1063 (3.7%) died within 28 days of telavancin initiation; only three deaths were considered possibly treatment related. Disposition of patients with missing or undocumented EOT assessments is summarized in the Supplementary Results. The majority of patients were male (53.4%), White (83.4%), and not Hispanic or Latino (93.5%), with a mean weight of 92.8 ± 24.4 kg and mean body mass index of 31.2 ± 9.5 kg/m2 (Table 1). Mean patient age was 55.2 ± 15.4 years; 29.4% of patients were ≥ 65 years of age. Of 657 patients with reported baseline CrCl, 13 (2.0%) had CrCl < 30 mL/min and 35 (5.3%) had CrCl 30 to < 50 mL/min; 36 patients were on dialysis. Hypertension (44.8%), diabetes mellitus type 2 (31.5%), and myocardial infarction (10.3%) were the most common baseline co-morbidities (Table 1). Patients were most commonly treated for cSSSI (48.7%), followed by bone and joint infections (27.4%), bacteremia and endocarditis (14.2%), and lower respiratory tract infections (LRTIs; 8.5%).
3.2 Prescribing Patterns
Mean daily dose of telavancin was 741.7 ± 194.3 mg (median 750 mg; IQR 700–750 mg) or 8.4 ± 2.1 mg/kg (median 8.3 mg/kg; IQR 6.9–9.9 mg/kg) (Table 2). The most common average daily dose category was 750 mg in 590 (55.5%) patients, followed by < 750 mg in 290 (27.3%), 1000 mg in 63 (5.9%), > 750 to < 1000 mg in 62 (5.8%), and > 1000 mg in 58 (5.5%) patients. Mean treatment duration was 17 ± 17 days; the most common treatment duration was 7 to < 21 days in 389 (36.6%) patients, followed by < 7 days in 352 (33.1%) patients (Table 2). The mean daily dose of telavancin was lower for patients on dialysis (562.9 ± 255.2 mg) or patients with baseline CrCl < 30 mL/min (513.2 ± 227.6 mg) or 30 to < 50 mL/min (578.5 ± 169.8 mg) relative to the full population (Table 2). Treatment duration and median average daily dose per body weight were also lower for patients with CrCl 30 to < 50 mL/min relative to the overall population (Table 2), consistent with dose adjustments due to renal impairment as indicated per telavancin labeling [6].
3.3 Pathogens Isolated
Infecting pathogens were identified in 738 (69.4%) patients at baseline (see additional details in the Supplementary Results). Monomicrobial Gram-positive infections were identified in 621 (58.4%) patients, multiple Gram-positive organisms without Gram-negative organisms in 48 (4.5%) patients, and mixed Gram-positive/negative infections in 76 (7.1%) patients. The most common baseline pathogen isolated was MRSA, in 401 (37.7%) patients, followed by MSSA in 119 (11.2%) patients, and coagulase-negative Staphylococcus in 93 (8.7%) patients (Table 3).
3.4 Prior Antibiotic Usage
Telavancin was used as first-line therapy in 303 (28.5%) patients and second-line or greater therapy in 760 (71.5%) patients; 519 (48.8%) patients received one prior antibiotic, 188 (17.7%) received more than one, 50 (4.7%) received more than two, and ten (0.9%) received more than three prior antibiotics. The most frequently administered prior antibiotics were vancomycin (29.4%), daptomycin (8.5%), and sulfamethoxazole/trimethoprim (7.8%).
3.5 Clinical Response
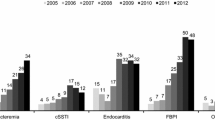
Of 964 (90.7%) TOUR patients with available assessment at EOT, 749/964 (77.7%) had positive clinical outcomes, 97/964 (10.1%) patients failed treatment, and 118/964 (12.2%) patients had indeterminate outcomes (Fig. 1). Including all 1063 patients and counting missing assessments at EOT as failures, 70.5% had a positive clinical response, 18.4% failed treatment (9.1% with documented treatment failure and 9.3% with missing or undocumented assessment), and 11.1% had indeterminate outcomes. Among patients with available EOT assessment, the overall positive clinical response rates by infection type were comparable at 74.2% in patients with bacteremia or endocarditis, 78.7% in patients with bone and joint infections, 80.1% in patients with cSSSI, and 67.1% in patients with LRTI (Fig. 1); however, these groups were not mutually exclusive or comprehensive. Outcomes by cSSSI and LRTI subtype are reported in the Supplementary Results. The positive clinical response rate was 78.8% for all infections with Gram-positive pathogens, 76.2% for MRSA, 80.7% for MSSA, 86.0% for multiple Gram-positive infecting pathogens, and 58.5% for mixed Gram-positive and Gram-negative infections. At post-treatment assessment, recurrence of infection or reinfection occurred in 19/809 patients assessed. Available data for 99 patients without EOT assessments is presented in the Supplementary Results and Supplementary Table 2; reasons for missing or undocumented assessments were not captured.

Clinical outcomes for TOUR patients available for assessment at the end of treatment for major infection types. aThe represented groups are not mutually exclusive, and not comprehensive. Positive clinical response includes cured and improved to step-down oral therapy. cSSSI complicated skin and skin-structure infections, LRTI lower respiratory tract infection, TOUR Telavancin Observational Use Registry
3.6 Location of Care and Care Setting Utilization
The majority of patients, 598/1063 (56.3%), were treated in outpatient infusion centers or clinics. A total of 429/1063 (40.4%) initiated telavancin treatment as inpatients [77 (7.2%) in an intensive care unit (ICU), 347 (32.6%) in other hospital settings, and 5/1063 (0.5%) in an emergency department].
For patients who initiated telavancin treatment in non-ICU hospital settings, the mean duration of hospitalization was 12.8 ± 14.5 days (range 1–94 days). For patients who started treatment in the ICU, the mean duration of stay was 30.1 ± 45.4 days. Mean treatment durations in outpatient infusion centers or clinics were 20.8 ± 19.3 and 17.6 ± 15.8 days, respectively. Mean duration of treatment initiated in other locations, such as home, was 32.3 ± 15.5 days.
3.7 Safety
Treatment-emergent AEs (TEAEs) of interest comprised renal TEAEs in 63 (5.9%) patients, including renal failure in 62 (5.8%) patients; TEAEs leading to discontinuation of telavancin in 122 (11.5%) patients; and TEAEs leading to fatal outcomes in 31 (2.9%) patients (Table 4). Serious TEAEs occurred in 44 (4.1%) patients; of these patients, 24 (2.3%) discontinued the registry study. The 31 fatal TEAEs included three deaths possibly related to telavancin and two deaths for which relationship to treatment was not recorded; the remaining fatal TEAEs were judged unrelated to telavancin. The most common TEAEs were renal failure (62/1063; 5.8%), nausea (18/1063; 1.7%), and vomiting (11/1063; 1.0%) (Table 4). Renal failure was considered possibly related to treatment in 58 (5.5%) patients and resulted in telavancin discontinuation in 37 (3.5%) patients (Table 2). Dialysis was recorded as an intervention in 11 (1.0%) patients. Renal failure resolved in 46 (4.3%) patients and led to a fatal outcome in one (0.1%) patient (Table 2). Serious renal TEAEs occurred in 15 (1.4%) patients and were considered possibly related to telavancin in 13/15 patients. Although not reported as serious AEs, nausea and vomiting were reported as possibly related to treatment in 18 (1.7%) and 11 (1.0%) patients, respectively; these events all led to discontinued treatment but eventually resolved in all patients.
Baseline and post-baseline creatinine measurements were available for approximately 43% of patients and remained generally stable throughout treatment. Change in mean serum creatinine measurements was small, from 0.96 mg/dL at baseline to 1.07 mg/dL at EOT. Likewise, mean CrCl was 127.31 mL/min at baseline and 113.72 mL/min at EOT. Among 63 patients with renal AEs, 48 (76%) received vancomycin < 2 days prior to telavancin or were taking other nephrotoxic medications concomitantly, as did 4/7 patients investigated for potentially reduced renal function. Concomitant administration of nephrotoxic medications, most commonly acetylsalicylic acid (17.8%), lisinopril (14.3%), and vancomycin (14.3%), was recorded in 349 patients. Piperacillin sodium with tazobactam was administered before telavancin in three (0.9%) patients. As vancomycin and telavancin should not be administered together, recorded concomitant vancomycin use may represent instances where the last dose of vancomycin was administered < 2 days prior to the first dose of telavancin during antibiotic switching (Supplementary Table 3).
4 Discussion
Real-world treatment results from TOUR support the use of telavancin for a variety of infections due to Gram-positive pathogens. Telavancin treatment produced positive clinical responses in the majority of patients assessed at EOT when used for the approved indications of cSSSI and HABP/VABP. Positive clinical responses also resulted from telavancin treatment for other LRTIs, bacteremia and endocarditis, or bone and joint infections. Patients were treated in a range of care settings for a typical duration of 7–21 days at a median telavancin dose of 8.3 mg/kg (IQR 6.9–9.9 mg/kg). Despite real-world use of telavancin at lower doses relative to labeling (10 mg/kg) [6], patients showed mostly positive clinical responses to treatment. Telavancin was generally well tolerated. Patients enrolled in TOUR had varying levels of renal function at baseline and were dosed accordingly. Following telavancin treatment, 62 patients (5.8%) experienced renal failure, which resolved in 46/62 patients (74.2%). Among patients who experienced renal AEs, 48/63 (76%) received other nephrotoxic medications ≤ 2 days before or during telavancin therapy, which may have contributed. These included patients who received vancomycin, which has been associated with renal toxicity in similar patients [19, 20]. Overall, telavancin produced positive clinical outcomes in at least 70% of patients and was generally well tolerated.
In phase 3 trials, telavancin was a noninferior alternative to vancomycin for the approved indications of cSSSI and HABP/VABP infections due to MRSA and MSSA. For some infections, especially cSSSI caused by MRSA and HABP/VABP due to S. aureus with a vancomycin minimum inhibitory concentration ≥ 1 μg/mL, clinical cure rates were numerically higher in patients treated with telavancin versus vancomycin [11, 12, 21]. In a retrospective analysis of the phase 3 trials, telavancin also demonstrated noninferiority to vancomycin for treatment of cSSSI and HABP/VABP with concomitant bacteremia [13]. In other studies, telavancin therapy had comparable efficacy to standard treatment (vancomycin or anti-staphylococcal penicillin) for S. aureus bacteremia [22] and achieved clinical success in 7/8 patients with end-stage renal disease with MRSA bacteremia who failed treatment with other therapies [23] and 10/14 patients with MRSA bone and joint infections [24]. Results from TOUR confirm the real-world efficacy of telavancin for treatment of the approved indications and provide evidence that clinicians are successfully using telavancin to treat additional infection types.
This registry study has several limitations inherent to observational studies including being neither controlled nor blinded. Patient enrollment decisions were made by individual clinicians, potentially biasing patient selection. All data were gathered from retrospective medical chart review, limiting available information. Efficacy outcomes were based on subjective assessments of investigators at each site, thus individual interpretation could introduce bias. Additionally, patient loss to follow-up may have impacted interpretation. The microbiology data can only be considered supportive due to differing standards of care and nonsystematic collection of microbiology data across participating sites. Collection of TEAEs was limited to events of interest, and renal function results were not collected systematically. Despite these limitations, TOUR includes a large cohort of patients with a wide range of clinical characteristics and infection types and provides data on real-world use of telavancin.
5 Conclusion
Overall, TOUR documents telavancin use in clinical practice with satisfactory results. While prescribers should continue to monitor renal function closely, this registry provides data on the impact of renal toxicity in real-world prescribing. Data from TOUR supports use of telavancin for the approved indications of cSSSI and HABP/VABP while providing insight into clinician use of telavancin for additional infection types, including other LRTIs, bacteremia and endocarditis, and bone and joint infections.
References
Tong SY, Davis JS, Eichenberger E, Holland TL, Fowler VG Jr. Staphylococcus aureus infections: epidemiology, pathophysiology, clinical manifestations, and management. Clin Microbiol Rev. 2015;28(3):603–61.
Baggs J, Fridkin SK, Pollack LA, Srinivasan A, Jernigan JA. Estimating national trends in inpatient antibiotic use among US hospitals from 2006 to 2012. JAMA Intern Med. 2016;176(11):1639–48.
Wunderink RG, Rello J, Cammarata SK, Croos-Dabrera RV, Kollef MH. Linezolid vs vancomycin: analysis of two double-blind studies of patients with methicillin-resistant Staphylococcus aureus nosocomial pneumonia. Chest. 2003;124(5):1789–97.
Rotun SS, McMath V, Schoonmaker DJ, et al. Staphylococcus aureus with reduced susceptibility to vancomycin isolated from a patient with fatal bacteremia. Emerg Infect Dis. 1999;5(1):147–9.
Smith TL, Pearson ML, Wilcox KR, et al. Emergence of vancomycin resistance in Staphylococcus aureus. Glycopeptide-intermediate Staphylococcus aureus Working Group. N Engl J Med. 1999;340(7):493–501.
VIBATIV® (telavancin), USP [package insert]. South San Francisco: Theravance Biopharma US, Inc; 2016.
Karlowsky JA, Nichol K, Zhanel GG. Telavancin: mechanisms of action, in vitro activity, and mechanisms of resistance. Clin Infect Dis. 2015;61(Suppl 2):S58–68.
Mendes RE, Farrell DJ, Sader HS, Streit JM, Jones RN. Update of the telavancin activity in vitro tested against a worldwide collection of Gram-positive clinical isolates (2013), when applying the revised susceptibility testing method. Diagn Microbiol Infect Dis. 2015;81:275–9.
Saravolatz LD, Pawlak J. VISA-Daptomycin non-susceptible Staphylococcus aureus frequently demonstrate non-susceptibility to telavancin. Diagn Microbiol Infect Dis. 2019;93(2):159–61.
Duncan LR, Sader HS, Smart JI, Flamm RK, Mendes RE. Telavancin activity in vitro tested against a worldwide collection of Gram-positive clinical isolates (2014). J Glob Antimicrob Resist. 2017;10:271–6.
Rubinstein E, Lalani T, Corey GR, et al. Telavancin versus vancomycin for hospital-acquired pneumonia due to gram-positive pathogens. Clin Infect Dis. 2011;52(1):31–40.
Stryjewski ME, Graham DR, Wilson SE, et al. Telavancin versus vancomycin for the treatment of complicated skin and skin-structure infections caused by gram-positive organisms. Clin Infect Dis. 2008;46(11):1683–93.
Wilson SE, Graham DR, Wang W, Bruss JB, Castaneda-Ruiz B. Telavancin in the treatment of concurrent Staphylococcus aureus bacteremia: a retrospective analysis of ATLAS and ATTAIN studies. Infect Dis Ther. 2017;6(3):413–22.
Corey GR, Kollef MH, Shorr AF, et al. Telavancin for hospital-acquired pneumonia: clinical response and 28-day survival. Antimicrob Agents Chemother. 2014;58(4):2030–7.
Theravance Biopharma Announces Marketing Authorization for VIBATIV® (Telavancin) in Russia for Treatment of Multiple Infections Caused by Gram-Positive Bacteria, Including MRSA [press release]. Dublin: Theravance Biopharma; 2015.
Theravance Biopharma Announces Health Canada Approval for VIBATIV® (telavancin) for Treatment of HAP/VAP Caused by Gram-Positive Bacteria, Including MRSA [press release]. Dublin: Theravance Biopharma; 2015.
VIBATIV 250 MG. Ministry of Health Israel Drug Directory; 2018.
Vibativ: Withdrawal of the marketing authorisation in the European Union. London: European Medicines Agency; 2018.
Contreiras C, Legal M, Lau TYY, Thalakada R, Shalansky S, Ensom MHH. Identification of risk factors for nephrotoxicity in patients receiving extended-duration, high-trough vancomycin therapy. Can J Hosp Pharm. 2014;67(2):126–32.
Marinho DS, Huff G, Ferreira BL, et al. The study of vancomycin use and its adverse reactions associated to patients of a Brazilian university hospital. BMC Res Notes. 2011;4(236):1–6.
Sandrock CE, Shorr AF. The role of telavancin in hospital-acquired pneumonia and ventilator-associated pneumonia. Clin Infect Dis. 2015;61(Suppl 2):579–86.
Stryjewski ME, Lentnek A, O’Riordan W, et al. A randomized Phase 2 trial of telavancin versus standard therapy in patients with uncomplicated Staphylococcus aureus bacteremia: the ASSURE study. BMC Infect Dis. 2014;14:289.
Britt NS, Tirmizi S, Ritchie DJ, et al. Telavancin for refractory MRSA bacteraemia in intermittent haemodialysis recipients. J Antimicrob Chemother 2017.
Harting J, Fernandez F, Kelley R, Wiemken T, Peyrani P, Ramirez J. Telavancin for the treatment of methicillin-resistant Staphylococcus aureus bone and joint infections. Diagn Microbiol Infect Dis. 2017;89(4):294–9.
Acknowledgements
The authors would like to thank the investigators and participating institutions of TOUR; Nancy Havrilla, MS, RN, for her efforts in coordinating TOUR; and Heidi Goldstein, a consultant for Theravance Biopharma R&D, Inc., for data validation and quality control. Editorial and medical writing support was provided by Judy Phillips, DVM, PhD, of AlphaBioCom, LLC, and funded by Theravance Biopharma R&D, Inc.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Funding
This work was supported by Theravance Biopharma R&D, Inc. and Cumberland Pharmaceuticals Inc.
Conflict of interest
Dr. Bressler has received fees for participating in advisory boards and speaker bureaus for the Theravance Biopharma group of companies. Dr. Hassoun has received fees for participating in advisory boards and speaker bureaus for the Theravance Biopharma group of companies. Dr. Saravolatz has previously received fees for participating in advisory boards and speaker bureaus for the Theravance Biopharma group of companies; and he has received research grants from Theravance Biopharma US, Inc., paid to Saint John Hospital and Medical Center during the course of the study. Dr. Ravenna is an employee of Theravance Biopharma US, Inc., and holds stock in Theravance Biopharma, Inc. Dr. Castaneda-Ruiz and Dr. Barnes are former employees of Theravance Biopharma US, Inc., and hold stock in Theravance Biopharma, Inc.
Data availability
Theravance Biopharma, Inc. (and its affiliates) will not be sharing individual de-identified participant data or other relevant study documents.
Additional information
Bibiana Castaneda-Ruiz and Chris Barnes are former employees of Theravance Biopharma US, Inc.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Bressler, A.M., Hassoun, A.A., Saravolatz, L.D. et al. Clinical Experience with Telavancin: Real-World Results from the Telavancin Observational Use Registry (TOUR™). Drugs - Real World Outcomes 6, 183–191 (2019). https://doi.org/10.1007/s40801-019-00165-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40801-019-00165-8