
Abstract
Background
Daily care procedures provoke breakthrough pain and anxiety in palliative situations. Dexmedetomidine may be an alternative to opioids during nursing procedures for older patients.
Objective
We aimed to compare the efficacy of intranasal dexmedetomidine with subcutaneous opioids on the intensity of pain and anxiety during comfort management procedures.
Methods
We conducted a randomized, active-controlled, double-blind, crossover trial (NCT03151863). Patients aged ≥ 65 years were randomized to receive, 45 min before nursing care, either intranasal dexmedetomidine together with subcutaneous placebo or intranasal placebo together with a subcutaneous opioid. Each of these two interventions were administered in a cross-over design and spaced out over a 24- or 48-h period. The primary outcome was the number of patients with an Elderly Caring Pain Assessment score > 5. Secondary outcomes included pain, sedation score, and vital signs.
Results
Because of difficult recruitment, the trial was interrupted after the inclusion of 24 patients. Three patients withdrew after randomization, leaving 21 patients undergoing 42 complete sessions for descriptive analyses. Of the 21 patients, 12 (57.1%) were women, and their median age was 84 years, interquartile range (75–87 years). Nine (42.9%) patients presented an Elderly Caring Pain Assessment score > 5 when receiving subcutaneous opioids, and seven (33.3%) with intranasal dexmedetomidine. Hypoxemia occurred in a single patient receiving subcutaneous opioids. No episode of bradycardia was observed.
Conclusions
Intranasal dexmedetomidine is feasible in elderly patients and may be an alternative to opioids to ensure comfort during nursing care. Future studies are needed to confirm the efficacy and safety of this procedure.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Finding an easy, effective, and safe procedural pain management approach could help many older patients improve their end-of-life palliative care with reduced side effects. |
Intranasal dexmedetomidine administration is feasible in elderly patients and may have the potential to provide better short-term analgesia, anxiolysis, and light-to-mild sedation during daily nursing care than subcutaneous opioids. |
Future similar trials should consider less restrictive inclusion criteria and including the next-of-kin in a patient and public involvement approach to ensure sufficient enrollment. |
1 Background
Nursing care at the end of life is part of the strategy for enhancing a patient’s comfort. However, even simple procedures may increase pain intensity and lead to breakthrough pain [1, 2]. Procedural pain prevalence ranges from 12 and 20% in adults [1, 3]. Most breakthrough pain episodes induced by care procedures are related to daily comfort care, which was shown to remain painful despite the administration of preventive analgesia in four of ten patients at end-of-life [4]. Comfort management includes both non-pharmacological and pharmacological interventions, the choice of which is based on a patient’s situation, procedures, and care setting. Ideal pharmacological agents should produce anxiolytic, sedative, and analgesic effects, while being conveniently administered through non-invasive painless routes, and with an excellent safety profile [2]. In daily practice, opioids are often used for this indication, but they are associated with a high risk of adverse effects.
Dexmedetomidine (DEX) is a new-generation, G-protein-coupled, α2 receptor agonist with sedative and analgesic properties. The α2 receptors are widely distributed in the central nervous system. By binding to the pre-synaptic receptors, DEX inhibits the release of norepinephrine, therefore terminating the propagation of pain signals and attenuating central nervous system excitation [5]. The main sites for its analgesic and sedative effect are the spinal cord and locus coeruleus of the brain stem, respectively [6]. Compared with clonidine, DEX is eight to ten times more selective towards α2-adrenergic receptors, producing a stronger intrinsic activity and a better cardiovascular profile and no or minimal respiratory depression [7].
Therefore, the sedative, anesthetic, anxiolytic, and analgesic properties of DEX offer an attractive alternative to opioids. Although some adverse effects may be expected following both opioids and DEX (i.e., dizziness, confusion, dry mouth), the latter is associated with a better safety profile and a lower risk of bradycardia and hypotension, which are mostly observed when DEX is administered intravenously [8,9,10,11,12,13]. In this context, an interest for intranasal (IN) DEX for sedation has emerged because of its convenient and pain-free administration and its lack of clinically significant adverse effects, particularly following a single dose [14,15,16,17,18,19,20,21,22,23,24,25,26]. Dexmedetomidine could therefore decrease pain intensity during daily nursing care, thus enhancing comfort in palliative older patients. However, there is a paucity of studies reporting IN DEX use in elderly patients and/or palliative situations.
Indeed, most of the studies reporting on IN DEX use focused on neonates, children, or young healthy adults [12], whose responses to drugs differ from older adults [27]. Thus, this study fills an important knowledge gap regarding IN DEX administration in older and frail patients.
1.1 Objective
The purpose of this study was to determine whether IN DEX could decrease pain and anxiety better than subcutaneous (SC) opioids in elderly patients during daily nursing care.
2 Methods
To report this study, we followed the 2010 Consolidated Standards of Reporting Trials (CONSORT) reporting guidelines [28].
2.1 Trial Design
The INDEX trial was designed as a randomized, superiority, cross-over, double-blind, active-controlled trial. It was stopped early because of recruitment failure and a shortage of staff during the COVID pandemic. A descriptive analysis is provided below.
2.2 Participants
The trial was conducted from November 2018 to July 2020 at Geneva University Hospitals (Geneva, Switzerland). Written informed consent was obtained from each participant, in accordance with the Declaration of Helsinki [29].
2.3 Eligibility Criteria
Inclusion criteria for patients were admission to the Geneva University Hospitals’ palliative care or geriatric rehabilitation divisions, age ≥ 65 years, requirement of opioids for pain relief on a regular basis, and undergoing, at least once a day, a nursing procedure (lasting from 15 to 30 min) that caused sufficient discomfort (either pain, anxiety, or both) as to require the administration of extra opioid doses. Patients were not considered if they were at risk of bronchial aspiration, respiratory or cardiac complications, or if they had a contraindication for nasal drug administration (for details, see Table 1).
The population targeted in this study were elderly patients, who may be considered as a “vulnerable” population. To avoid risks of coercion and anticipate severe cognitive disorders at end-of-life that would make a participant incapable of judgment, information was provided as soon as possible to patients and their relatives. Before each of the two sessions of the study, patients were asked, by a research nurse, if they were still willing to participate, and the inclusion/exclusion criteria were rechecked.
2.4 Study Interventions
Each participant underwent two nursing care sessions in a cross-over design. Both nursing care sessions took place in the morning and were spaced out over a 24- or 48-h time period. The choice of this delay was based on the elimination half-life of IN DEX, which is 2–3 h [5].
All participants received their regular ongoing opioid treatment (i.e., morphine or hydromorphone). Oral intake was allowed before nursing care. All patients received both study drugs: either IN DEX and SC placebo [NaCl 0.9%], or IN placebo [NaCl 0.9%] and SC opioid. Study drugs were administered 45 min before the start of the nursing care sessions, so that a 15- to 30-min nursing care would be covered by the peak effect of both SC opioids and IN DEX.
Subcutaneous midazolam 0.05 mg/kg (of actual body weight) was available, if required, as a rescue treatment if the total Elderly Caring Pain Assessment (ECPA) score reached 5 points, and the nursing care session was not about to end. Oxygen supplementation was provided if oxygen saturation fell below 85%. Two nurses or assistant nurses were responsible for nursing care interventions, while a research nurse or the first author oversaw assessments of outcomes.
2.5 Outcome Measures
The timing of measurement of the primary, secondary, and safety outcomes is described in Table 2.
2.6 Primary Outcome Measures
The ECPA score, assessed by a research nurse or physician, enables the measurement of both pain and anxiety related to nursing care. The ECPA is a validated tool to assess pain and anxiety and comprises eight items divided in two parts, based on the behavior of non-communicating elderly patients [30]. One to five minutes are needed to complete each part of this evaluation. The first part of the scale (score: 0–16) is used for pain assessment before nursing care, while the second part (score: 0–16) assesses pain during nursing care. The total score ranges from 0 to 32. Our primary outcome was the number of patients with an ECPA total score > 5.
2.6.1 Secondary Outcome Measures
2.6.1.1 ECPA During Nursing Care, Detailed
The four components of pain assessed with the ECPA during nursing care are described independently: (1) anxious anticipation of caregiver intervention; (2) reactions during mobilization; (3) reactions when painful parts of the body are nursed; and (4) complaints. The number of patients needing rescue midazolam because of an ECPA score > 5 during the nursing procedure was assessed.
2.6.1.2 Pain Intensity (Visual Analog Scale)
Pain intensity was assessed every 15 min from drug administration until nursing care and every 30 min after nursing care until recovery of the initial modified Observer’s Assessment of Alertness/Sedation Scale (mOAA/S), or up to 2 h following nursing care, by the patient with a visual analog scale (VAS) from 0 (no pain) to 10 cm [31]. The maximum VAS score during nursing care was also reported.
2.6.1.3 Sedation (mOAA/S)
Sedation levels were assessed with mOAA/S, which is a validated tool with seven levels [32]. One minute is enough to complete the assessment. It was assessed at the same timepoints as the VAS, from drug administration until 2 h following the end of nursing care.
2.6.2 Safety Outcomes
Because of the specific population, the only safety outcomes registered were desaturation and bradycardia. Participants were monitored for heart rate and oxygen saturation with a pulse oximeter, during the whole sessions and follow-up periods. Bradycardia was defined as a heart rate below 60 beats per minute lasting more than 30 s. Hypoxemia was defined as an oxygen saturation under 85% lasting more than 60 s. The number of patients with bradycardia or hypoxemia during nursing care is reported together with the treatment required.
2.7 Sample Size
We considered that IN DEX would make a clinically meaningful improvement if it could decrease the proportion of patients who would experience pain defined as an ECPA score > 5 by 20%. We hypothesized that the proportion of patients who would experience pain when receiving SC opioids would be 50%, and that this proportion would decrease to 30% with IN DEX. We also hypothesized that the intra-patient correlation was 0.50. To reach a power of 80% to show a difference of 20% at a significance level of 5% using a two-sided McNemar’s chi-squared test, a total of 52 patients was needed. As a 25% drop-out was expected (either because of withdrawal of consent or death before the beginning of the study or between the two sessions due to their own evolution), the sample size was increased to 66 patients. Because of a shortage in healthcare providers and challenges in recruiting during the COVID pandemic, recruitment was stopped after having randomized 24 patients.
2.8 Randomization
Randomization was generated in blocks of four by the Geneva University Hospitals’ Pharmacy to ensure blinding and concealment of allocation. Two randomization lists were generated, corresponding to each of the two opioids allowed as control treatment (i.e., morphine and hydromorphone). Randomization determined the order of administration of the two interventions. Patients were randomized to receive either IN DEX in the first nursing care session and SC opioids in the second, or SC opioids in the first and IN DEX in the second nursing care session.
2.9 Blinding
The study medications were provided by our pharmacy in prepacked sealed kits for each randomization number and for each session, labeled in a blinded manner. Two types of kits, sequentially and clearly labeled with different colors, were prepared, one for each type of opioid used (morphine and hydromorphone). Kits for both nursing care sessions were prepared in separate zip plastic bags. Each session package contained one of the study treatments.
A vial for SC administration contained either 3 mL of 20 mg/mL of morphine (or 10 mg/mL of hydromorphone) or NaCl 0.9% with similar packaging. The dosage administered corresponded to 10% of each patient’s opioid daily dose.
A vial for IN administration contained 1.2 mL of 100-µg/mL solution of DEX or NaCl 0.9%, with similar packaging. A 1-mL syringe capped with an IN mucosal atomization device (MAD300; Teleflex, Wayne, PA, USA) was used for IN administration. The investigational product administered to patients in a supine position by the IN route corresponded to 0.125 mL/10 kg of DEX (1.25 µg/kg of actual body weight) or NaCl 0.9%.
2.9.1 Statistical Methods
Because of the premature termination of the study and the obvious lack of power, the analyses provided here are descriptive, according to the cross-over design: each patient should have had the two sequences on an intention-to-treat basis. No statistical test is performed. Qualitative variables are expressed in counts and percentage. A 95% confidence interval (CI) is computed around estimates for the primary outcome. Quantitative variables are expressed in median (IQR) and range.
3 Results
3.1 Participant Flow
During the 20-month period of recruitment, 523 patients were assessed for eligibility, of whom 24 were randomized. Three randomized patients did not complete the two trial interventions. One patient showed signs of impending death and did not receive the first nursing care session in the IN DEX/SC opioid sequence, and two patients were excluded before starting the second session in the context of hypotension and septic shock in the SC opioid/IN DEX sequence. Finally, a total of 21 patients were included in the intention-to-treat analysis (Fig. 1).

Study flowchart. Dex dexmedetomidine, IN intranasal, SC subcutaneous
3.2 Recruitment
The trial was conducted from 14 November, 2018, to 27 July, 2020, and was stopped because of recruitment difficulty during the pandemic.
3.3 Baseline Data
Baseline characteristics of participants are presented in Table 3. Of the 21 patients analyzed, ten received the IN DEX/SC opioid sequence, and 11 received the SC opioid/IN DEX sequence. Two patients received hydromorphone, and 19 morphine, as SC opioids. Sex distribution was balanced (12 women and 9 men), age ranged from 65 to 93 years, and median actual body weight was 57 kg. Eight participants had a diagnosis of cancer. Their Palliative Performance Scale ranged from 20 to 50%. Nine patients had one or more wounds and five presented with a recent fracture, for which only a conservative treatment was decided. Hypoactive delirium was present in four participants.
All participants were able to rate their current level of pain with the VAS before completed interventions. Pain intensity at baseline ranged from VAS 0 to 8 cm (median 3) and their mOAA/S score range from 4 to 6 (median 5). The mean heart rate was 94 ± 17 and, mean oxygen saturation was 94 ± 2.3.
3.4 Outcomes
Outcome measures are summarized in Table 4.
3.4.1 Primary Endpoint (ECPA Score)
Before the beginning of the nursing care sessions, 45 min after study drug administration, ECPA scores were low (median 0, IQR 0–1). During the nursing care session, the ECPA scores increased in both groups (median 4, IQR 2–8). A total of 16 (38.1%) patients presented with an ECPA score > 5. Nine (42.9%, 95% CI 21.8–66.0) when receiving the SC opioids, and 7 (33.3%, 95% CI 14.6–57.0) when receiving IN DEX.
3.4.2 Secondary Endpoints
-
The ECPA during nursing care. Details of the four items of the ECPA during nursing care are reported in the Electronic Supplementary Material.
Two patients received rescue midazolam because of discomfort during nursing care, one in each treatment group.
-
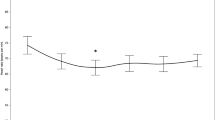
Pain intensity (VAS). Following study drug administration, VAS scores decreased progressively with time and reached a median [IQR] of 1 [0–4] after 45 min, before the start of the nursing care sessions. During the nursing care period, the maximum VAS reached a median [IQR] of 6 [4–7.5] in patients receiving SC opioids and 4 [2.5–6.5] in those receiving IN DEX. After the nursing care, VAS scores decreased in both groups.
-
Sedation (mOAA/S). Before starting nursing care, following study drug administration, the mOAA/S scores remained stable. Most (88.1%) patients returned to their initial mOAA/S value during the 120-min follow-up period.
3.4.3 Safety Outcomes
None of the patients experienced bradycardia. One patient presented with an episode of hypoxemia that required oxygen administration when receiving SC opioids.
4 Discussion
Pain in older patients often remains under-diagnosed, poorly recognized, and inadequately treated. Pain management strategies other than opioids by the oral or parenteral route are needed [33]. Relaxation techniques and medications such as nonsteroidal anti-inflammatory drugs, acetaminophen, and topical medications can reduce pain but often do not provide adequate pain relief. We acknowledge the limitations due to the insufficient sample size of our study, but considering that managing pain without opioids is demanding, and that data from randomized trials in this specific population are scarce, we believe it is relevant to share our results.
4.1 Findings and Context
The major finding of this study is that IN administration of study drugs was easy and convenient in all participants, even in those in whom a confusional state was detected. Furthermore, our results, while limited, suggest that IN DEX could be an alternative to SC opioids in older patients. Indeed, there were no severe adverse events reported, and the IN DEX sedative effect was mild, enabling the patient collaboration during nursing care and minimal monitoring.
Emerging literature highlights the potential role of DEX in palliative care. A case series [34], case reports [35, 36], a small prospective (26 adults of mean age > 65 years) [37], and a nine-patient pediatric cohort study [38] all suggest the potential interest of IN, IV, or SC infusions of DEX for the treatment of intractable pain, opioid-induced hyperalgesia, terminal intractable delirium, and dystonia [34,35,36,37,38]. The adequate dose of IN DEX to be administered was a challenging choice. One case report suggested that both 1 and 1.5 µg/kg of IN DEX were safe and effective to induce light sedation in the management of complex wound dressings for cutaneous thoracic metastatic bilateral breast cancer in a 45-year-old woman [39]. The recommended doses of IN DEX varied from 0.5 to 1.5 µg/kg for adults, while the doses commonly reported in children varied from 0.5 to 4 µg/kg [13, 15, 20, 23,24,25, 40, 41]. Intranasal DEX bioavailability was estimated to be 40.6% (95% CI 34.7–54.4) for atomization [42]. It must be underlined that age-adjusted dosing is not recommended, although caution is warranted as sedative effects, hypotension, and bradycardia might be more pronounced in elderly patients. Based on the literature review, previous local experience and observations, the dose chosen for DEX treatment in the present study was 1.25 μg/kg of actual body weight. Interestingly, in studies published recently (2019–22), and therefore after the present trial had been initiated, IN DEX 100, 50 µg, or 1 µg/kg was administered before anesthesia, or after spinal/or general anesthesia in elderly healthy subjects, with a relatively good tolerance profile [43,44,45].
4.2 Generalizability, Strengths, and Limitations
Our study population reflects the geriatric population encountered in daily practice, palliative units, hospices, or retirement homes, despite the stringent non-inclusion criteria applied. The strength of our study is that it addresses an important topic concerning a population rarely studied in randomized controlled trials. It has been well designed and conducted partly in a difficult period. A cross-over design was chosen for two main reasons. First, because pain experience differs from one individual to another and because the differences can be even larger between patients of the targeted population. Second, expecting a relatively scarce number of patients recruited, the cross-over design was an interesting option. A maximum period of 24–48 h between the two nursing care sessions was decided as rapid changes in a patient’s status may occur near end-of-life. Although, because of the patient’s health conditions, some dropouts occurred between the two sessions, we believe that the cross-over design was a good choice. Because of the specific type and health conditions of the studied population, we expected diverse adverse events, unrelated to the investigational product, to occur and therefore focused only on bradycardia and hypotension. Eventually, bradycardia was not observed with IN DEX during the study. Although this alone does not allow a conclusion on the safety of the IN DEX administration, we did not face serious adverse events.
The main limitation of this study is that we encountered difficulties in recruitment, leading to prolonged duration of the trial and lack of resources, and were therefore unable to enroll the number of patients needed to draw firm conclusions. The problem of difficult recruitment in clinical trials including older patients is well recognized [46]. Our restrictive eligibility criteria certainly led to a reduced recruitment. In fact, of the 523 patients assessed for eligibility, 460 (88%) were not eligible. Although these criteria were settled with the aim to minimize the likelihood of harm to vulnerable patients (e.g., ileus, recent stroke, heart, or respiratory failure), and of frequently reported side effects (nausea/vomiting, respiratory depression), some of these criteria should be revised if a similar study was planned. For example, we restricted inclusion to patients with a weight > 80 kg, as an 80-kg patient would need to receive an IN volume of 1 mL, which is the commonly maximum volume recommended for nasal administration. If we were to plan a future study, we may choose to include these patients and adapt the administration scheme with a maximum dose. Additionally, excluding patient using opioids other than morphine and hydromorphone on a regular basis may not be necessary. We chose SC morphine or hydromorphone as active comparators as these were the opioids most frequently used in our institution, reaching their peak effect after 45 min, with a maximum efficiency lasting up to 90 min. However, 42 patients were not approached because they were using other opioids. Less stringent eligibility criteria could improve participation. In the present trial, about half of the patients approached refused to participate. The fact that, from March 2020 on, their relatives were hardly available for discussion, in the context of visit restrictions during the COVID-19 pandemic, did not help. It is possible that in another context, the acceptance rate would have been greater. However, this a fair consent rate for a drug clinical trial according to our experience in Geneva. A recently published survey highlights that more time is needed to enroll older patients and suggests that it can be dealt with by increasing the number of recruiting sites, planning a longer time for recruitment, widening eligibility criteria, and adapting the information on the study to this population [47]. Finally, a future study should try to involve the next-of-kin in a patient and public involvement approach [48]. Collaboration with the next-of-kin of seriously ill patients would certainly help to better understand what can be implemented in the design and conduct of the trial to make it more attractive and valuable for patients and their families. For example, the selection of an appropriate tool for pain assessment is challenging. Although many exist, there is limited evidence regarding their reliability, feasibility, and clinical utility for older adults [49]. We chose what we considered as a meaningful score of 5 on the ECPA, together with a self-reported measure of pain as the ECPA is user friendly and its internal consistency has an acceptable rating of 0.7, compared with other scales [49]. As an appropriate choice of outcomes and tools for measuring outcomes is essential, we strongly encourage researchers to discuss with patients and their next-of-kin in order to select the most appropriate assessment tools for future studies by conducting a feasibility or pilot study. Finally, as this was a clinical trial, we did not attempt to describe the pharmacokinetics of the study drugs in this specific population.
4.3 Interpretation/Adaptation and Future Directions
The present study is too small to draw any conclusion regarding the efficacy and safety of the IN administration of DEX. However, we have collected data on 21 patients from a population rarely included in randomized trials. We believe that recognizing and discussing our difficulties, as well as describing our results is relevant as it will enable the scientific and medical community to design and achieve future multi-centric studies and hamper failure in recruitment. Although SC and oral routes could also be possible suitable routes for DEX administration, in palliative care situations, especially in the community or hospice setting [50, 51], future multi-centric trials should consider IN DEX as an option for procedural pain management.
5 Conclusions
The new insights this study has yielded are that IN DEX administration was feasible and could potentially provide safe short-term analgesia, anxiolysis, and light-to-mild sedation during daily nursing care in older patients receiving opioids regularly. Future trials should consider strategies to ensure sufficient enrollment. If statistically supported by a larger study, the novel findings reported in this study could benefit a large segment of society.
References
Magnani C, Giannarelli D, Casale G. Procedural pain in palliative care: is it breakthrough pain? A multicenter national prospective study to assess prevalence, intensity, and treatment of procedure-related pain in patients with advanced disease. Clin J Pain. 2017;33(8):707–14. https://doi.org/10.1097/AJP.0000000000000450.
Czarnecki ML, Turner HN, Manda Collins P, et al. Procedural pain management: a position statement with clinical practice recommendations. Pain Manag Nurs. 2011;12(2):95–111. https://doi.org/10.1016/j.pmn.2011.02.003.
Birnie KA, Chambers CT, Fernandez CV, et al. Hospitalized children continue to report undertreated and preventable pain. Pain Res Manag. 2014;19(4):198–204. https://doi.org/10.1155/2014/614784.
Maillard F. Statut de performance et douleur des soins: résultats préliminaires de l’étude SPdol. Available from: http://www.cnrd.fr/Resultats-preliminaires-de-l-etude-8526. Accessed 12 Aug 2022.
Weerink MAS, Struys MMRF, Hannivoort LN, et al. Clinical pharmacokinetics and pharmacodynamics of dexmedetomidine. Clin Pharmacokinet. 2017;56(8):893–913. https://doi.org/10.1007/s40262-017-0507-7.
Virtanen R, Savola JM, Saano V, et al. Characterization of the selectivity, specificity and potency of medetomidine as an alpha 2-adrenoceptor agonist. Eur J Pharmacol. 1988;150:9–14.
Zhao Y, He J, Yu N, et al. Mechanisms of dexmedetomidine in neuropathic pain. Front Neurosci. 2020;14:330. https://doi.org/10.3389/fnins.2020.00330.
Hsu YW, Cortinez LI, Robertson KM, et al. Dexmedetomidine pharmacodynamics: part I: crossover comparison of the respiratory effects of dexmedetomidine and remifentanil in healthy volunteers. Anesthesiology. 2004;101(5):1066–76. https://doi.org/10.1097/00000542-200411000-00005.
Yoo H, Lirola T, Vilo S, et al. Mechanism-based population pharmacokinetic and pharmacodynamic modeling of intravenous and intranasal dexmedetomidine in healthy subjects. Eur J Clin Pharmacol. 2015;71(10):1197–207. https://doi.org/10.1007/s00228-015-1913-0.
Dexdor. Compendium suisse des médicaments. March 2017. Available from: https://compendium.ch/mpro/mnr/23800/html/fr?Platform=Desktop. Accessed 1 Sept 2022.
Chen K, Lu Z, Xin YC, et al. Alpha-2 agonists for long-term sedation during mechanical ventilation in critically ill patients. Cochrane Database Syst Rev. 2015;1:CD010269. https://doi.org/10.1002/14651858.CD010269.pub2.
Yuen VM, Hui TW, Irwin MG, et al. A randomised comparison of two intranasal dexmedetomidine doses for premedication in children. Anaesthesia. 2012;67(11):1210–26. https://doi.org/10.1111/j.1365-2044.2012.07309.x.
Plambeck MZ, Afshari A. Dexmedetomidine in the pediatric population: a review. Minerva Anesthesiol. 2015;81:320–32.
Li BL, Ni J, Huang JX, et al. Intranasal dexmedetomidine for sedation in children undergoing transthoracic echocardiography study: a prospective observational study. Paediatr Anaesth. 2015;25(9):891–6. https://doi.org/10.1111/pan.12687.
European Medicines Agency. Dexdor: EPAR: product information. Available from: http://www.ema.europa.eu/ema/index.jsp?curl=pages/includes/document/document_detail.jsp?webContentId=WC500115631&mid=WC0b01ac058009a3dc. Accessed 11 Oct 2022.
Yuen VM, Irwin MG, Hui TW, et al. A double-blind, crossover assessment of the sedative and analgesic effects of intranasal dexmedetomidine. Anesth Analg. 2007;105(2):374–80. https://doi.org/10.1213/01.ane.0000269488.06546.7c.
Patel VJ, Ahmed SS, Nitu ME, et al. Vasovagal syncope and severe bradycardia following intranasal dexmedetomidine for pediatric procedural sedation. Paediatr Anaesth. 2014;24(4):446–8. https://doi.org/10.1111/pan.12368.
Surendar MN, Pandey RK, Saksena AK, et al. A comparative evaluation of intranasal dexmedetomidine, midazolam and ketamine for their sedative and analgesic properties: a triple blind randomized study. J Clin Pediatr Dent. 2014;38(3):255–61. https://doi.org/10.17796/jcpd.38.3.l828585807482966.
Akin A, Bayram A, Esmaoglu A, et al. Dexmedetomidine vs midazolam for premedication of pediatric patients undergoing anesthesia. Paediatr Anaesth. 2012;22(9):871–6. https://doi.org/10.1111/j.1460-9592.2012.03802.x.
Talon MD, Woodson LC, Sherwood ER, et al. Intranasal dexmedetomidine premedication is comparable with midazolam in burn children undergoing reconstructive surgery. J Burn Care Res. 2009;30(4):599–605. https://doi.org/10.1097/BCR.0b013e3181abff90.
Nooh N, Sheta SA, Abdullah WA, et al. Intranasal atomized dexmedetomidine for sedation during third molar extraction. Int J Oral Maxillofac Surg. 2013;42(7):857–62. https://doi.org/10.1016/j.ijom.2013.02.003.
Reynolds J, Rogers A, Capehart S, et al. Retrospective comparison of intranasal dexmedetomidine and oral chloral hydrate for sedated auditory brainstem response exams. Hosp Pediatr. 2016;6(3):166–71. https://doi.org/10.1542/hpeds.2015-0152.
Sheta SA, Al-Sarheed MA, Abedlhalim AA. Intranasal dexmedetomidine vs midazolam for premedication in children undergoing complete dental rehabilitation: a double-blinded randomized controlled trial. Paediatr Anaesth. 2014;24(2):181–9. https://doi.org/10.1111/pan.12287.
Lia JE, Chen JY, Hu X, et al. A randomised study of intranasal dexmedetomidine and oral ketamine for premedication in children. Anaesthesia. 2013;68(9):944–9. https://doi.org/10.1111/anae.12312.
Gyanesh P, Haldar R, Srivastava D. Comparison between intranasal dexmedetomidine and intranasal ketamine as premedication for procedural sedation in children undergoing MRI: a double-blind, randomized, contrôle actif standard-controlled trial. J Anesth. 2014;28(1):12–8. https://doi.org/10.1007/s00540-013-1657-x.
Cimen ZS, Hansi A, Sivrikaya GU, et al. Comparison of buccal and nasal dexmedetomidine premedication for pediatric patients. Paediatr Anaesth. 2013;23(2):134–8.
Stephenson T. How children’s responses to drugs differ from adults. Br J Clin Pharmacol. 2005;59(6):670–3. https://doi.org/10.1111/j.1365-2125.2005.02445.x.
Schulz KF, Altman DG, Moher D, et al. CONSORT 2010 statement: updated guidelines for reporting parallel group randomized trials. BMC Med. 2010;24:11–32. https://doi.org/10.1186/1745-6215-11-32.
World Medical Association. Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–4. https://doi.org/10.1001/jama.
Morello R, Jean A, Alix M, et al. A scale to measure pain in non-verbally communicating older patients: the EPCA-2 Study of its psychometric properties. Pain. 2007;133(1–3):87–98. https://doi.org/10.1016/j.pain.2007.03.007.
McCormack HM, Horne DJ, Sheather S. Clinical applications of visual analogue scales: a critical review. Psychol Med. 1988;18(4):1007–19. https://doi.org/10.1017/s0033291700009934.
Chernik DA, Gillings D, Laine H, et al. Validity and reliability of the Observer’s Assessment of Alertness/Sedation Scale: study with intravenous midazolam. J Clin Psychopharmacol. 1990;10(4):244–51.
Pautex S, Vogt-Ferrier N, Zulian GB. Breakthrough pain in elderly patients with cancer: treatment options. Drugs Aging. 2014;31(6):405–11. https://doi.org/10.1007/s40266-014-0181-5.
Hofherr ML, Abrahm JL, Rickerson E. Dexmedetomidine: a novel strategy for patients with intractable pain, opioid-induced hyperalgesia, or delirium at the end of life. J Palliat Med. 2020;23(11):1515–7. https://doi.org/10.1089/jpm.2019.0427.
Hilliard N, Brown S, Mitchinson S. A case report of dexmedetomidine used to treat intractable pain and delirium in a tertiary palliative care unit. Palliat Med. 2015;29(3):278–81. https://doi.org/10.1177/0269216314556923.
De Zen L, Della Paolera S, Del Rizzo I, et al. Home intranasal dexmedetomidine for refractory dystonia in pediatric palliative care. J Pain Symptom Manag. 2020;59(6):e3–5. https://doi.org/10.1016/j.jpainsymman.2020.02.022.
Thomas B, Lo WA, Nangati Z, et al. Dexmedetomidine for hyperactive delirium at the end of life: an open-label single arm pilot study with dose escalation in adult patients admitted to an inpatient palliative care unit. Palliat Med. 2021;35(4):729–37. https://doi.org/10.1177/0269216321994440.
Burns J, Jackson K, Sheehy KA, et al. The use of dexmedetomidine in pediatric palliative care: a preliminary study. J Palliat Med. 2017;20(7):779–83. https://doi.org/10.1089/jpm.2016.0419.
Ferguson L, Wilson M. Intranasal dexmedetomidine: procedural sedation in palliative care: a case report. Palliat Med. 2021;35(8):1625–8. https://doi.org/10.1177/02692163211022184.
Cheung CW, Qiu Q, Chu KM, et al. Intranasal dexmedetomidine in combination with patient-controlled sedation during upper gastrointestinal endoscopy: a randomised trial. Acta Anaesthesiol Scand. 2015;59(2):215–23. https://doi.org/10.1111/aas.12445.
Mekitarian FE, Robinson F, de Carvalho WB, et al. Intranasal dexmedetomidine for sedation for pediatric computed tomography imaging. J Pediatr. 2015;166(5):1313-15.e1. https://doi.org/10.1016/j.jpeds.2015.01.036.
Li A, Yuen VM, Goulay-Dufaÿ S, et al. Pharmacokinetic and pharmacodynamic study of intranasal and intravenous dexmedetomidine. Br J Anaesth. 2018;120(5):960–8. https://doi.org/10.1016/j.bja.2017.11.100.
Uusalo P, Jätinvuori H, Löyttyniemi E, et al. Intranasal low-dose dexmedetomidine reduces postoperative opioid requirement in patients undergoing hip arthroplasty under general anesthesia. J Arthroplasty. 2019;34(4):686-92.e2. https://doi.org/10.1016/j.arth.2018.12.036.
Seppänen SM, Kuuskoski R, Mäkelä KT, et al. Intranasal dexmedetomidine reduces postoperative opioid requirement in patients undergoing total knee arthroplasty under general anesthesia. J Arthroplasty. 2021;36(3):978-85.e1. https://doi.org/10.1016/j.arth.2020.09.032.
Xu X, Cao Y, Wu Y, Ding M. Intranasal dexmedetomidine in elderly patients (aged > 65 years) during maxillofacial surgery: sedative properties and safety analysis. J Oral Maxillofac Surg. 2022;80(3):443–55. https://doi.org/10.1016/j.joms.2021.10.013.
Lirola T, Vilo S, Manner T, et al. Bioavailability of dexmedetomidine after intranasal administration. Eur J Clin Pharmacol. 2011;67(8):825–31. https://doi.org/10.1007/s00228-011-1002-y.
Buttgereit T, Palmowski A, Forsat N, et al. Barriers and potential solutions in the recruitment and retention of older patients in clinical trials-lessons learned from six large multicentre randomized controlled trials. Age Ageing. 2021;50(6):1988–96. https://doi.org/10.1093/ageing/afab147.
Crocker JC, Ricci-Cabello I, Parker A, et al. Impact of patient and public involvement on enrolment and retention in clinical trials: systematic review and meta-analysis. BMJ. 2018;363: k4738. https://doi.org/10.1136/bmj.k4738.
Lichtner V, Dowding D, Esterhuizen P, et al. Pain assessment for people with dementia: a systematic review of systematic reviews of pain assessment tools. BMC Geriatr. 2014;17(14):138. https://doi.org/10.1186/1471-2318-14:138.
Chamadia S, Pedemonte JC, Hobbs LE, et al. A pharmacokinetic and pharmacodynamic study of oral dexmedetomidine. Anesthesiology. 2020;133(6):1223–33. https://doi.org/10.1097/ALN.0000000000003568.
Uusalo P, Al-Ramahi D, Tilli I, et al. Subcutaneously administered dexmedetomidine is efficiently absorbed and is associated with attenuated cardiovascular effects in healthy volunteers. Eur J Clin Pharmacol. 2018;74(8):1047–54. https://doi.org/10.1007/s00228-018-2461-1.
Acknowledgements
The authors thank C. Mathey and C. Matis, who have contributed to the study sessions and collecting the data.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
Open access funding provided by University of Geneva. This research was partially supported by grants of the Geneva University Hospitals’ Projects Research & Development’s (PRD 12-2017-I) and the Swiss Academy of Medical Sciences’ Program for Research in Palliative Care (PC 04/17).
Conflict of interest
Nathalie Dieudonné Rahm, Isabelle Zaccaria, Béatrice Gil Wey, Sophie Pautex, Walid Habre, and Nadia Elia have no conflicts of interest that are directly relevant to the content of this article.
Ethics approval
This study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments, has received formal approval from the regulatory authorities, Swissethics (No. 2017-01211) on 26 October, 2017, and Swissmedic (ID 2018DR3056) on 18 May, 2018, and was registered in ClinicalTrials.gov (NCT03151863).
Consent to participate
A signed informed written consent was obtained from all participants or from their legal representative.
Consent for publication
Not applicable.
Availability of data and material
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Code availability
Not applicable.
Author contributions
Conceptualization: NDR, BGW, NE, WH; design, methodology: NE (lead), NDR, WH, BGW; funding acquisition: NDR, WH, SP; investigation, acquisition of data: NDR; project administration: BGW, NDR; data curation and analysis: IZ; interpretation of results: NE (lead), IZ; drafting the manuscript, writing review and editing: NDR (lead), NE, WH; supervision: WH (sponsor of the trial), NE, SP; revising the manuscript and approval of the final version: all authors; agreement to be accountable for all aspects of the work: all authors.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Dieudonné Rahm, N., Zaccaria, I., Gil Wey, B. et al. Intranasal Dexmedetomidine for Pain Management in Older Patients: A Cross-Over, Randomized, Double-Blinded, Active-Controlled Trial. Drugs Aging 40, 527–538 (2023). https://doi.org/10.1007/s40266-023-01027-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40266-023-01027-3