
Abstract
Introduction
Central nervous system toxicity is a well-known side effect of isotretinoin treatment. The aim of this study was to establish the effects of isotretinoin on retinal nerve fiber layer (RNFL) thickness.
Materials and Methods
Study subjects received oral isotretinoin treatment for nodulocystic acne. All patients underwent a detailed ophthalmologic examination including best-corrected visual acuity, slit-lamp examination, tonometry, color vision assessment, fundoscopy, and RNFL measurement. RNFL measurements by optical coherence tomography were done at onset, and were repeated at the 1st and 6th months of therapy.
Results
A total of 22 eyes of 11 patients (seven males and four females) were included in this study. The mean age of the patients was 20.18 ± 5.13 (14–26) years. Mean RNFL thickness was 90.72 ± 9.19 (78.2–112.0) μm before treatment, 90.40 ± 9.24 (79.5–112.4) μm after 1 month of treatment, and 90.52 ± 8.92 (78.4–114.8) μm after 6 months. No statistically significant change was detected between RNFL thickness values before and after treatment.
Conclusion
No adverse effects of systemic isotretinoin treatment on RNFL thickness were observed.
Similar content being viewed by others

Introduction
Isotretinoin, or 13-cis retinoic acid, is the treatment of choice for severe recalcitrant nodular acne, and has been used to treat various other skin disorders, such as severe recalcitrant psoriasis, for almost two decades [1]. This drug has numerous ocular side effects, including abnormal meibomian gland secretions, blepharoconjunctivitis, corneal opacities, decreased dark adaptation, decreased tolerance to contact lens use, decreased vision, increased tear osmolarity, keratitis, meibomian gland atrophy, myopia, ocular discomfort, dry eyes, photophobia, and teratogenic ocular abnormalities [2–4].
Previous reports have suggested a causal association between oral isotretinoin and acquired central nervous system (CNS) neurotoxicity and neuropathy [5–7]. The most frequent CNS adverse effect associated with oral isotretinoin is headache, either as an independent adverse effect or as part of benign intracranial hypertension, which is additionally characterized by nausea and visual changes [5–7]. A single case of optic swelling associated with isotretinoin has also been reported [8]. Retinal ganglion cells contain melanopsin, which is very similar to other opsin photopigments, and it is known that melanopsin uses the same retinaldehyde chromophore. Therefore, isotretinoin may exert an inhibitory effect on chromophore regeneration in retinal ganglion cells similar to what is seen in rod and cone cells [9]. However, to the best of the authors’ knowledge, this is the first study that objectively determines retinal nerve fiber layer (RNFL) thickness changes after 6 months of oral isotretinoin treatment.
Materials and methods
Patients prescribed typical oral isotretinoin (0.5 mg/kg) to treat nodulocystic acne were referred by dermatologists for a detailed ophthalmologic examination. Informed consent and ethical approval was given by patients. This initial examination included visual acuity, slit-lamp examination, tonometry, color vision assessment with Ishihara plates, dilated fundoscopy with a 78D lens, and RNFL measurement by Optical Coherence Tomography (Cirrus HD Spectral OCT, Carl Zeiss Meditec Inc., Dublin, CA, USA). Patients >40 years of age, with systemic and/or ocular disorders, those who had previous ocular surgery, and those receiving systemic corticosteroid treatment were excluded. Best-corrected visual acuity (BCVA) of all patients was measured by Snellen chart at 6 m prior to isotretinoin treatment. The same experienced observer performed RNFL thickness measurements by Optical Coherence Tomography at the onset of isotretinoin treatment, as well as after the 1st and 6th months of therapy. Three consecutive measurements were acquired at each visit, and the mean of these three readings was used for statistical analysis. All statistical analyses were performed using SPSS version 17.0 (SPSS Inc., Chicago, IL, USA) and a P value <0.05 was considered statistically significant.
Results
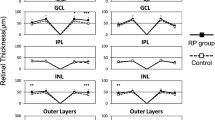
A total of 22 eyes of 11 patients (seven males and four females) were included in this study. The mean age of the patients was 20.18 ± 5.13 (14–26) years. BCVA of all patients was 20/20 by Snellen chart at 6 m prior to isotretinoin treatment. BCVA and refraction values showed no significant change after 1 or 6 months of treatment. Mean intraocular pressure was 13.2 ± 1.4 mmHg at onset, 13.7 ± 1.5 mmHg at 1-month follow-up, and 13.4 ± 1.2 mmHg at 6 months. No change was detected in color vision or fundoscopy before and after treatment. Mean RNFL thickness was 90.72 ± 9.19 (78.2–112.0) μm before treatment, 90.40 ± 9.24 (79.5–112.4) μm at 1 month, and 90.52 ± 8.92 (78.4–114.8) μm at 6 months. No statistically significant change was detected in RNFL thickness values before and after treatment (P = 0.08). There were no consistent trends of change in the regional areas of thickness, which is shown in a double-hump pattern in printouts.
Discussion
Retinoids are believed to play an essential role in the growth, differentiation, and function of nervous tissue in vivo and in vitro. Electrophysiological and clinical findings have suggested a causal association between an acquired CNS neurotoxicity or neuropathy and oral retinoids [10–12]. Decreased visual acuity, various visual field defects, pseudotumor cerebri, optic neuritis, and decreased color vision are the most common side effects involving the ocular nervous system that have been shown to be closely related to oral isotretinoin therapy [1, 3, 13, 14]. Visual field defects are more common in the central visual field due to pseudotumor cerebri and/or optic neuropathy [15]. In addition, oral retinoids have multiple mucocutaneous and systemic side effects. Different retinoids have different side effect profiles: isotretinoin tends to cause more mucosal drying, acitretin has higher incidences of alopecia and palmar/plantar desquamation, and reduced night vision is more common with fenretinide [16]. Teratogenicity is also a limiting factor with all oral retinoids.
Several studies have reported the importance of RNFL thickness determination in the early diagnosis and management of optic nerve conditions, such as glaucoma, and optic nerve diseases, including optic neuritis [17]. Optical coherence tomography can reveal changes in RNFL thickness before visual field defects appear [18]. In the present study, the authors did not find any RNFL changes due to isotretinoin treatment, despite the fact that oral isotretinoin treatment has been known to cause decreased dark adaptation, pseudotumor cerebri, optic nerve edema, and headaches. However, Dinc et al. [19] reported a case of bilateral optic nerve atrophy and decreased RNFL thickness associated with isotretinoin treatment for acne vulgaris, supporting the hypothesis that isotretinoin may cause RNFL changes.
In the present study, no neurotoxic side effects were detected. Similar to the present findings, Sari et al. [15] evaluated optic nerve function in patients treated with oral isotretinoin both clinically and with visual field tests, and reported no significant change after 5.5 months. In a pivotal study by Weleber et al. [4], three of 50 patients treated with isotretinoin (1 mg/kg/day) for cystic acne complained of poor night vision and/or excessive glare sensitivity. While still receiving the drug or shortly thereafter, two patients were found to have abnormal dark-adaptation curves, with elevations of either cone or rod thresholds, or both. Six months following cessation of therapy, the electroretinograph was still abnormal for one patient, but continued improvement was evident at 25 months; for the second patient, the electroretinograph was normal at 1 year.
Nyctalopia, or night blindness, has been reported with isotretinoin use [20]. This has been associated with objectively abnormal scotopic electroretinograms. It has been postulated that competitive inhibition of ocular retinol dehydrogenase by isotretinoin may be the cause of the nyctalopia [21, 22]. None of the patients in this study developed nyctalopia after 6 months of treatment.
In the present study, the authors did not find any color vision disturbances. Color vision is a sensitive indicator of optic nerve dysfunction. It is reduced in retinal and optic nerve disorders. Fraunfelder et al. [2] first suggested an association between isotretinoin and reversible decreased color vision.
There are limitations of this study that must be addressed. First, the authors did not perform any electrophysiological studies. In a recent study, an increased latency of P100 wave was detected after therapy in 18% of patients treated orally with isotretinoin [10]. Although this result was not statistically significant, subclinical effects of isotretinoin on optic nerve functions, which can be detected electrophysiologically before anatomical signs occur, may be possible. In addition, assessment of pupillary functions without using pupillography was another limitation of the present study.
Conclusion
In conclusion, the authors did not find any adverse effects of systemic isotretinoin treatment on RNFL thickness. Nevertheless, the authors think that the assessment of these functions in a larger patient group and with additional tests for early detection of visual field loss, such as Short Wavelength Automated Perimetry (SWAP) or Frequency Doubling Technology (FDT), would be more appropriate.
References
Fraunfelder FW, Fraunfelder FT, Corbett JJ. Isotretinoin-associated intracranial hypertension. Ophthalmology. 2004;111:1248–50.
Fraunfelder FT, Fraunfelder FW, Edwards R. Ocular side effects possibly associated with isotretinoin usage. Am J Ophthalmol. 2001;132:299–305.
Fraunfelder FW, Fraunfelder FT. Adverse ocular drug reactions recently identified by the national registry of drug-induced ocular side effects. Ophthalmology. 2004;111:1275–9.
Weleber RG, Denman ST, Hanifin JM, Cunningham WJ. Abnormal retinal function associated with isotretinoin therapy for acne. Arch Ophthalmol. 1986;104:831–7.
Chroni E, Monastirli A, Tsambaos D. Neuromuscular adverse effects associated with systemic retinoid dermatotherapy: monitoring and treatment algorithm for clinicians. Drug Saf. 2010;33:25–34.
Danby FW. Oral isotretinoin, neuropathy and hypovitaminosis A. Clin Exp Dermatol. 2009;34:e260.
Danby FW. Oral isotretinoin, neuropathy and hypovitaminosis A. Clin Exp Dermatol. 2008;33:190.
Lerman S. Ocular side effects of accutane therapy. Lens Eye Toxic Res. 1992;9:429–38.
Szabo B. Antiandrogenic effect of isotretinoin: is the retina involved in mechanism of action? Med Hypotheses. 2007;69:1281–3.
Aydogan K, Turan OF, Onart S, Yazici B, Karadogan SK, Tokgoz N. Neurological and neurophysiological effects of oral isotretinoin: a prospective investigation using auditory and visual evoked potentials. Eur J Dermatol. 2008;18:642–6.
Chroni E, Sakkis T, Georgiou S, et al. Stiff-person syndrome associated with oral isotretinoin treatment. Neuromuscul Disord. 2002;12:886–8.
Nikiforidis G, Tsambaos D, Karamitsos D, Koutsojannis C, Georgiou S. Effects of oral isotretinoin on human auditory brainstem response. Dermatology. 1994;189:62–4.
Brelsford M, Beute TC. Preventing and managing the side effects of isotretinoin. Semin Cutan Med Surg. 2008;27:197–206.
Ellis CN, Krach KJ. Uses and complications of isotretinoin therapy. J Am Acad Dermatol. 2001;45:S150–7.
Sari A, Dinc E, Adiguzel U, Yildirim O, Kaya Tİ. Evaluation of optic nerve functions in patients treated with isotretinoin. TOD J. 2010;40:1–3. http://www.oftalmoloji.org/tr/makale/2/1/Tam-Metin. Accessed Dec 9 2012.
Ellis CN, Voorhees JJ. Etretinate therapy. J Am Acad Dermatol. 1987;16:267–91.
Pinilla I, Garcia-Martin E, Idoipe M, Sancho E, Fuertes I. Comparison of retinal nerve fiber layer thickness measurements in healthy subjects using Fourier and time domain optical coherence tomography. J Ophthalmol. 2012;2012:107053.
Bowd C, Zangwill LM, Berry CC, et al. Detecting early glaucoma by assessment of retinal nerve fiber layer thickness and visual function. Invest Ophthalmol Vis Sci. 2001;42:1993–2003.
Dinc UA, Yenerel NM, Gorgun E, Oral D, Oncel B, Oncel M. A case with bilateral optic nerve atrophy associated with isotretinoin treatment for acne vulgaris. TOD J. 2007;39:60–3. http://www.oftalmoloji.org/tr/makale/145/10/Tam-Metin. Accessed Dec 9 2012.
Rodahl K, Moore T. The vitamin a content and toxicity of bear and seal liver. Biochem J. 1943;37:166–8.
Watson NJ, Hutchinson CH. Rod and cone malfunction as a manifestation of isotretinoin therapy—a case report. J Dermatol Treat. 1992;3:205–7.
Weinberg DV, D’Amico DJ. Retinal toxicity of systemic drugs. In: Albert DM, Jakobiec FA, editors. Principles and practice of ophthalmology. New York: WB Saunders; 1994. p. 1042–50.
Acknowledgments
All the authors had full access to the data. Dr. Kaptı is the guarantor for this article, and takes responsibility for the integrity of the work as a whole.
Conflict of interest
None of the authors have any conflict of interest to declare.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License (https://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Kaptı, B.H., Aslan, G. & Yavruoğlu, M.A. Evaluation of Retinal Nerve Fiber Layer Changes with Oral Isotretinoin Treatment. Ophthalmol Ther 2, 19–23 (2013). https://doi.org/10.1007/s40123-012-0009-5
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40123-012-0009-5