
Abstract
Introduction
Serum neurofilament light chain (sNfL) is an emerging biomarker of neuronal damage in several neurological disorders. Its association with cognitive function in the general US population aged 60 years and above is unknown. The aim of this study was to investigate the correlation between sNfL and cognitive function in the general US population aged 60 and above.
Methods
The data were obtained from the 2013–2014 National Health and Nutrition Examination Survey (NHANES), which include 506 individuals aged 60 or older who met our search criteria. In our study, sNfL levels were divided into two groups based on dichotomization (19.0 pg/mL). After adjusting for multiple covariates, it was found that the high sNfL group (≥ 19.0 pg/mL) had lower cognitive performance than the low sNfL group (< 19.0 pg/mL). This relationship was also stable in subgroup analysis.
Conclusion
In this sample of an American elderly population, higher sNfL levels are correlated with lower cognitive performance. Our findings suggest that sNfL may become a potential screening tool for early prediction and confirmation of cognitive damage.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
Cognitive disorders are increasing annually, placing a significant burden on society and families. The presence of a prolonged latency period prior to the manifestation of cognitive impairment highlights the need for reliable screening indicators to facilitate early diagnosis. |
Serum neurofilament light chain (sNfL) has emerged as a potential biomarker for neuronal damage in various neurological conditions, such as multiple sclerosis (MS), Parkinson's disease, and Alzheimer's disease. |
What was learned from the study? |
The implication of this study is that elevated levels of sNfL are associated with low cognitive performance in the general US population aged 60 and above. In the future, for the identification of specific neurological conditions, sNfL can serve as a potential screening biomarker for early diagnosis and intervention. |
Drawing from previous research conducted on populations with neurodegenerative disease, our hypothesis posits a correlation between sNfL levels and cognitive function in the general US population aged 60 and above. |
Introduction
Aging is a normal physiological process that involves degenerative changes in the function and structure of organs throughout the body as individuals grow older. Of these changes, cognitive decline or development of dementia are particularly noticeable. Any cognitive decline may eventually progress to dementia, which is best described as a syndrome rather than a specific disease, severe enough to interfere with independent daily activities. The causes of dementia are varied and include primary neurological, neuropsychiatric, and medical conditions. Neurodegenerative dementias, such as Alzheimer's disease (AD) and dementia with Lewy bodies, are most common in the elderly, while traumatic brain injury and brain tumors are common causes in younger adults [1]. AD is the most common neurodegenerative disease, accounting for an estimated 60–70% of all dementia cases worldwide [2]. Due to an aging population and an increase in chronic comorbidities, global estimates suggest that dementia will continue to rise [3,4,5], placing a significant burden on both society and families [6, 7]. By 2050, it is projected that the number of people with dementia will triple to 152 million [8].
Biomarkers associated with pathological processes are believed to indicate disease progression prior to the appearance of clinical signs of cognitive decline [9, 10]. Some core markers, such as Aβ42, total tau (t-tau), and phosphorylated tau (p-tau) in cerebrospinal fluid (CSF) [10], as well as newer markers like amyloid positron emission tomography (PET) [11, 12], the soluble form of trigger receptor expressed on myeloid cells 2 (sTREM2) [13], CSF neurogranin (Ng) [10], and neurofilament light chain (NfL) [14, 15], have been identified. NfL is considered to be a novel marker of neurodegeneration. It is one of the three subunits of neurofilaments, which are specific cytoskeletal proteins of neurons and are particularly abundant in extensively myelinated axons. Axonal damage releases NfL into the cerebrospinal fluid (CSF) and eventually into the blood. Higher levels of NfL are thought to indicate more severe cerebral axonal degeneration [16] and have been found to be elevated in CSF and blood in several neurodegenerative diseases [17]. Neurodegenerative disease is defined as a progressive decline in the function of the nervous system due to degenerative changes in nerve cells, which may cause changes in cognitive function. Many previous studies have explored the relationship between NfL levels and cognitive function in neurodegenerative disease. The majority of studies have found a negative correlation between NfL level and cognitive performance [18]. However, this relationship is not universal due to the nature of neurological disorders, individual differences between participants, or inconsistencies in testing methods [18].
Age is thought to be somewhat related to NfL level. The normal maximum reference value for NfL levels in CSF increases by 2.5-fold between the ages of 20 and 50 years, and subsequently doubles by the age of 70 years [19]. Research on cognitive aging has consistently demonstrated a pervasive decline in cognitive abilities as individuals grow older [20]. A strong correlation between age and NfL blood levels has also been observed, indicating a significant increase in NfL levels in the blood of healthy controls by 2.2% per year between the ages of 18 and 70. The utilization of the ultrasensitive single-molecule array (Simoa) technique facilitated this finding [21, 22].
The general population aged 60 years and older in the United States was the target population for this study. Drawing from previous research conducted on neurodegenerative diseases, we conducted this cross-sectional study, aimed to explore the relationship between sNfL and cognitive performance in the general US population aged 60 and above.
Methods
Data Sources
The cross-sectional data utilized in this study were obtained from the National Health and Nutrition Examination Survey (NHANES) 2013–2014. The NHANES was authorized by the National Center for Health Statistics (NCHS) Ethics Review Committee, and all participants completed written informed consent forms before participation. The NCHS Research Ethics Review Board (protocol #2011-17) approved these studies. The secondary analysis did not require additional Institutional Review Board approval and the Yancheng Third People's Hospital opted to waive ethical review. All data in this study were accessible on the following website: https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/default.aspx?BeginYear=2013.
This study adhered to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement.
Participants and Study Design
The NHANES is a program of studies conducted by the NCHS, which is a part of the Centers for Disease Control and Prevention (CDC). The CDC is responsible for providing crucial health statistics for the United States. This study utilized cross-sectional data from NHANES 2013–2014, conducted by the CDC and the NCHS. The study population consisted of 10,175 individuals who underwent interviews and physical examinations. To ensure data quality, certain exclusion criteria were applied. Individuals younger than 60 years of age and those with missing data for sNfL or cognitive score were excluded. Ultimately, a total of 506 subjects were included in the study. The flowchart of subject enrollment is presented in Fig. 1.

Flowchart of the present study. NHANES National Health and Nutrition Examination Survey. sNfL serum neurofilament light chain
Data Collection and Measurements
Demographic, health status, and lifestyle data were collected through household interviews and mobile examination center (MEC) questionnaires administered by trained interviewers. The demographic information gathered includes age, gender, race, and body mass index (BMI). Race categories include Mexican American, other Hispanic, non-Hispanic White, non-Hispanic Black, and other races. BMI is calculated by dividing weight (in kilograms) by height (in meters squared) and is derived from anthropometric measurements taken during NHANES. Marital status is categorized as either married or living with a partner, or living alone. Educational attainment is classified as less than 9 years of education, 9–12 years of education, or more than 12 years of education. Household income is classified into three categories based on the poverty income ratio (PIR) as defined by a US government report: low (PIR ≤ 1.3), medium (PIR > 1.3 to 3.5), and high (PIR ≥ 3.5). Health status data include self-reported history of hypertension, diabetes mellitus (DM), coronary heart disease, and stroke. Participants were asked if their doctor or other healthcare professional had diagnosed them with any of these conditions. Lifestyle data include smoking status and alcohol consumption. Smoking status is defined as having smoked at least 100 cigarettes in one's lifetime. Alcohol consumption is assessed by asking participants if they have consumed alcoholic beverages at least 12 times per year. Laboratory tests were conducted to measure glycohemoglobin, creatinine, estimated glomerular filtration rate (eGFR), and albumin levels.
sNfL Examination
Serum samples collected between 2013 and 2014 were subjected to NfL testing using a highly sensitive immunoassay developed by Siemens Healthineers. All steps are seamlessly executed on the fully automated Attelica immunoassay system. For further information and more detailed protocols, please refer to the following link: https://wwwn.cdc.gov/Nchs/Nhanes/2013-2014/SSSNFL_H.htm.
Diagnosis of Cognitive Impairment
The digit symbol substitution test (DSST) has been widely used to evaluate cognitive function in individuals aged 60 years and older [23, 24]. It is considered to be highly sensitive in detecting cognitive impairment in individuals with a good baseline level of cognition [4]. The DSST may be a more sensitive measure of dementia than the Mini-Mental State Examination [25], as it assesses processing speed, sustained attention, and working memory. Given the existence of previous studies that have singled out DSST for detection of cognitive performance, the same method was applied to our study [26]. During this exercise, participants were provided with a paper table containing nine numbers and symbols. They were given 2 min to match the symbols to the 133 boxes of adjacent numbers. The score is determined by the total number of correct pairs. Prior to the main test, participants were given a sample practice test. In the NHANES study, participants who were unable to correctly match symbols and numbers on their own during the practice test were not allowed to proceed.
The data file for this study can be obtained from the National Health and Nutrition Examination Survey, 2013–2014 Data Documentation, Codebook, and Frequencies, Cognitive Functioning (CFQ_H), Data File: CFQ_H.xpt available at https://wwwn.cdc.gov/Nchs/Nhanes/2013-2014/CFQ_H.htm.
There is no gold standard threshold for identifying low cognitive ability, so the lowest unweighted quartile (DSST 34) in the study population was used to define cognitive impairment or low cognitive function, in line with the previously used method [4, 26,27,28,29].
Statistical Analysis
All normally distributed and skewed continuous variables were expressed as mean (SD) or median (interquartile range [IQR]). Categorical variables were presented as frequencies (%). Missing information on family income and marital status was imputed using the median. Baseline characteristics were presented based on an sNfL level of 19.0 pg/mL. Multiple logistic regression models were utilized to examine the relationship between sNfL and cognitive function, employing both unadjusted and multivariate adjusted models. Subgroup analyses were conducted using stratified logistic regression models. Modifications and interactions of subgroups were assessed using likelihood ratio tests. Potential confounders were selected based on previous scientific literature or if they resulted in a change in effect estimates of more than 10%. All analyses were performed using the statistical software packages R (http://www.R-project.org, The R Foundation) and Free Statistics software version 1.7.1.
Results
Study Population
There were a total of 10,725 participants in the entire 2013–2014 cycle, out of which 1841 were over the age of 60. We excluded individuals with missing data for sNfL (n = 1299) and cognitive score (n = 36). Ultimately, this cross-sectional study included 506 participants from NHANES during 2013–2014. The detailed inclusion and exclusion process is presented in Fig. 1.
Baseline Characteristics
The participant characteristics are presented in Table 1, which illustrates the baseline characteristics of all subjects based on the dichotomies of sNfL. Among the 506 participants, 116 (22.9%) exhibited low cognitive performance. The average age of the participants was 66.5 years (SD 4.4), with women accounting for 269 (53.2%) of the total. It was observed that individuals with higher sNfL levels tended to be older and had a higher prevalence of low cognitive performance. In the high sNfL group, the mean glycohemoglobin level was 6.1 (SD 1.1), while the mean albumin level was 41.7 g/L (SD 3.1). Table 1 provides a stratification of the baseline characteristics of participants based on sNfL (19.0 pg/mL).
Relationship Between sNfL Levels and Cognitive Impairment
Table 2 presents the results of the univariate analysis. Several risk factors were found to be associated with low cognitive performance, including sNfL, age, race, education level, family income, marital status, alcohol consumption, DM, glycohemoglobin, and albumin levels.
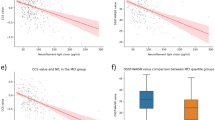
Table 3 presents the prevalence of cognitive impairment and the correlation between sNfL levels and low cognitive performance. The prevalence of low cognitive performance was 22.9% (116 subjects). The unadjusted odds ratio (OR) for the high group compared to the low group was 1.98 (95% CI 1.29–3.03; p = 0.002). After adjusting for various factors in the multivariable analysis (Table 3), sNfL levels were found to be significantly associated with the prevalence of low cognitive performance. The incidence of low cognitive performance was higher in the high sNfL group (> 19.0 pg/mL) compared to the low sNfL group (< 19.0 pg/mL). Moreover, adjusting for age, gender, BMI, race, education level, marital status, family income, hypertension, DM, smoking status, alcohol consumption, coronary heart disease, stroke, glycohemoglobin, creatinine, albumin, and eGFR did not significantly alter the results. The adjusted ORs (95% CI) for the prevalence of low cognitive performance were 1.75 (1.13–2.72), 3.17 (1.54–6.45), 2.78 (1.29–6.02) in models II–IV.
Stratified Analysis Based on Additional Variables
In order to determine the stability of the association between sNfL and cognitive impairment in various subgroups, stratified analysis was performed in this study (Fig. 2). None of the variables, including age (65–70 years and ≥ 70 years), BMI (< 25 and ≥ 25 kg/m2), education (< 12 and ≥ 12 years), and DM (yes/no), had a significant impact on the association between sNfL and cognitive decline (all p for interaction > 0.05).

Subgroup analyses of the association between sNfL levels and cognitive function in the database from NHANES 2013–2014. Adjusted for age, gender, BMI, race, education level, marital status, family income, hypertension, DM, smoking status, drink, CHD, stroke, glycohemoglobin, creatinine, albumin, eGFR. sNfL serum neurofilament light chain, NHANES National Health and Nutrition Examination Survey, OR odds ratio, CI confidence interval, BMI body mass index, eGFR estimated glomerular filtration rate
Discussion
The results of this study revealed a significant association between high sNfL levels and the development of cognitive decline in the elderly population sample in the United States. This association remained consistent even after adjusting for various models, indicating its robustness. Stratified analyses based on demographic and clinical factors further supported the stability of this association.
In our experiments, the high sNfL group of people with diabetes showed a more pronounced cognitive decline than people without diabetes. The relationship between diabetes and cognitive function has been widely studied [30, 31]. More than 50% of individuals with diabetes develop neuropathy, the main form of which is diabetic peripheral neuropathy (DPN) [31]. This affects individuals with diabetes or impaired glucose tolerance and/or impaired fasting glucose and is characterized by demyelination and axonal loss of peripheral sensory and motor nerves [32]. Axonal damage releases NfL into the cerebrospinal fluid (CSF) and eventually into the blood.
This is consistent with previous studies which have shown that patients with peripheral neuropathy have elevated sNfL [33, 34]. Other studies have shown that diabetes increases the risk of mild cognitive impairment (MCI) and dementia [30, 35]. In conclusion, sNfL may play an important role in mediating the relationship between diabetes and cognitive functioning, and we are able to assess neuronal damage and cognitive function in patients with diabetes by monitoring changes in sNfL levels.
Recent research has shown that patients with MCI and Alzheimer's disease (AD) have higher levels of NfL in their plasma compared to patients with subjective cognitive decline (SCD) [36]. While some studies have found no significant correlation between sNfL and cognitive function in adults without cognitive impairment, higher sNfL levels were associated with lower overall cognitive scores in the MCI population [21, 37]. These consistent findings suggest that the difference in sNfL levels and cognitive function is more pronounced in the MCI population than in normal CSF and plasma neurofilament light-control groups [16, 21, 38]. This makes it easier to detect a correlation between plasma NfL and cognitive function in MCI patients. In a recent cross-sectional analysis, higher sNfL levels were associated with poorer performance on all three cognitive functioning tests [39]. However, there is a lack of further detailed studies exploring the relationship between sNfL and cognitive function in the general US population aged 60 and above. Furthermore, a previous cohort study examined the relationship between sNfL levels and cognitive function in a population of elderly individuals with varying degrees of cognitive impairment [21]. The study included participants with normal cognitive function, MCI, and AD. The findings revealed that NfL levels were significantly higher in the AD group than in the MCI and normal cognitive function groups. Additionally, within the MCI group, higher sNfL levels were associated with a greater decline in cognitive function over a period.
The increase of NfL in cerebrospinal fluid (CSF) and blood is attributed to axonal damage that occurs in neurodegenerative diseases. This leads to an increased release of neuronal NfL into the interstitial fluid, which then diffuses into the CSF and blood [17]. Synaptic degeneration is widely recognized as a strong contributor to cognitive decline [40]. The loss of neurons and synapses throughout the brain occurs years before the clinical manifestation [41]. Axons play a critical role in transmitting impulses and facilitating cellular transport, making them the primary targets of neurodegeneration [42]. When axonal degeneration or neuronal loss occurs, the NfL is released into the cerebrospinal fluid (CSF) and plasma. Since axonal degeneration typically precedes and surpasses neuronal loss [42,43,44], early detection of CSF or plasma NfL levels may aid in the prevention of cognitive impairment at an early stage. In conclusion, there is an increasing correlation between axonal damage, loss of connectivity, and cognitive dysfunction [42]. Neurofilaments, as essential cytoskeletal components, regulate axonal caliber and growth, and facilitate the docking and transport of organelles. The hyperphosphorylation of the NfL is believed to lead to aggregation, impaired docking of motor proteins, and compromised transport [45]. The degree of phosphorylation has exhibited a negative correlation with the rate of axonal transport [46].
This study has several limitations that should be acknowledged. Firstly, the cross-sectional design of the study prevents us from establishing a causal relationship between sNfL and cognitive decline. Secondly, while this study focused on the association between sNfL and cognitive function, it is worth noting that other studies have suggested that cerebrospinal fluid NfL levels may provide a more accurate measure of neurodegeneration. However, a study found a correlation between sNfL and cerebrospinal fluid NfL levels [47], indicating that sNfL could potentially serve as a substitute for detecting changes in axonal disruption. Thirdly, the DSST can be used as part of an assessment of cognitive function, but it cannot be used alone to diagnose MCI, which prevented us from further exploring the relationship between sNfL and varying degrees of cognitive dysfunction in the general US population aged 60 and above.
Conclusion
In conclusion, this cross-sectional study provides evidence supporting the association between high sNfL levels and low cognitive function in the older US population sample. These findings have clinical implications for the early screening and management of cognitive decline. Further research is needed to elucidate the underlying mechanisms and explore potential therapeutic interventions.
Data Availability
The data were obtained from NHANES 2013–2014. All data were accessible on the following website: https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/default.aspx?BeginYear=2013.
References
Gale SA, Acar D, Daffner KR. Dementia. Am J Med. 2018;131(10):1161–9.
Leng F, Edison P. Neuroinflammation and microglial activation in Alzheimer disease: where do we go from here? Nat Rev Neurol. 2021;17(3):157–72.
Brookmeyer R, Johnson E, Ziegler-Graham K, Arrighi HM. Forecasting the global burden of Alzheimer’s disease. Alzheimers Dement. 2007;3(3):186–91.
Chen SP, Bhattacharya J, Pershing S. Association of vision loss with cognition in older adults. JAMA Ophthalmol. 2017;135(9):963–70.
Sperling RA, Aisen PS, Beckett LA, Bennett DA, Craft S, Fagan AM, et al. Toward defining the preclinical stages of Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):280–92.
Knopman DS, Amieva H, Petersen RC, Chetelat G, Holtzman DM, Hyman BT, et al. Alzheimer disease. Nat Rev Dis Primers. 2021;7(1):33.
Scheltens P, De Strooper B, Kivipelto M, Holstege H, Chetelat G, Teunissen CE, et al. Alzheimer’s disease. Lancet. 2021;397(10284):1577–90.
Li RX, Ma YH, Tan L, Yu JT. Prospective biomarkers of Alzheimer’s disease: a systematic review and meta-analysis. Ageing Res Rev. 2022;81: 101699.
Khachaturian ZS, Petersen RC, Snyder PJ, Khachaturian AS, Aisen P, de Leon M, et al. Developing a global strategy to prevent Alzheimer’s disease: Leon Thal Symposium 2010. Alzheimers Dement. 2011;7(2):127–32.
Zetterberg H, Bendlin BB. Biomarkers for Alzheimer’s disease-preparing for a new era of disease-modifying therapies. Mol Psychiatry. 2021;26(1):296–308.
Hansson O, Seibyl J, Stomrud E, Zetterberg H, Trojanowski JQ, Bittner T, et al. CSF biomarkers of Alzheimer’s disease concord with amyloid-beta PET and predict clinical progression: a study of fully automated immunoassays in BioFINDER and ADNI cohorts. Alzheimers Dement. 2018;14(11):1470–81.
Scheltens P, Blennow K, Breteler MM, de Strooper B, Frisoni GB, Salloway S, et al. Alzheimer’s disease. Lancet. 2016;388(10043):505–17.
Gaetani L, Paolini Paoletti F, Bellomo G, Mancini A, Simoni S, Di Filippo M, et al. CSF and blood biomarkers in neuroinflammatory and neurodegenerative diseases: implications for treatment. Trends Pharmacol Sci. 2020;41(12):1023–37.
Mattsson N, Cullen NC, Andreasson U, Zetterberg H, Blennow K. Association between longitudinal plasma neurofilament light and neurodegeneration in patients with Alzheimer disease. JAMA Neurol. 2019;76(7):791–9.
Olsson B, Lautner R, Andreasson U, Ohrfelt A, Portelius E, Bjerke M, et al. CSF and blood biomarkers for the diagnosis of Alzheimer’s disease: a systematic review and meta-analysis. Lancet Neurol. 2016;15(7):673–84.
Lin YS, Lee WJ, Wang SJ, Fuh JL. Levels of plasma neurofilament light chain and cognitive function in patients with Alzheimer or Parkinson disease. Sci Rep. 2018;8(1):17368.
Chatterjee P, Cheong YJ, Bhatnagar A, Goozee K, Wu Y, McKay M, et al. Plasma metabolites associated with biomarker evidence of neurodegeneration in cognitively normal older adults. J Neurochem. 2020;159(2):389–402.
Ramani S, Berard JA, Walker LAS. The relationship between neurofilament light chain and cognition in neurological disorders: a scoping review. J Neurol Sci. 2021;420:117229.
Yilmaz A, Blennow K, Hagberg L, Nilsson S, Price RW, Schouten J, et al. Neurofilament light chain protein as a marker of neuronal injury: review of its use in HIV-1 infection and reference values for HIV-negative controls. Expert Rev Mol Diagn. 2017;17(8):761–70.
Dzierzewski JM, Dautovich N, Ravyts S. Sleep and cognition in older adults. Sleep Med Clin. 2018;13(1):93–106.
Mattsson N, Andreasson U, Zetterberg H, Blennow K, Alzheimer’s Disease Neuroimaging I. Association of plasma neurofilament light with neurodegeneration in patients with Alzheimer disease. JAMA Neurol. 2017;74(5):557–66.
Disanto G, Barro C, Benkert P, Naegelin Y, Schädelin S, Giardiello A, et al. Serum Neurofilament light: a biomarker of neuronal damage in multiple sclerosis. Ann Neurol. 2017;81(6):857–70.
Baune BT, Brignone M, Larsen KG. A network meta-analysis comparing effects of various antidepressant classes on the Digit Symbol Substitution Test (DSST) as a measure of cognitive dysfunction in patients with major depressive disorder. Int J Neuropsychopharmacol. 2018;21(2):97–107.
Hoyer WJ, Stawski RS, Wasylyshyn C, Verhaeghen P. Adult age and digit symbol substitution performance: a meta-analysis. Psychol Aging. 2004;19(1):211–4.
Proust-Lima C, Amieva H, Dartigues JF, Jacqmin-Gadda H. Sensitivity of four psychometric tests to measure cognitive changes in brain aging-population-based studies. Am J Epidemiol. 2007;165(3):344–50.
Peeri NC, Egan KM, Chai W, Tao M-H. Association of magnesium intake and vitamin D status with cognitive function in older adults: an analysis of US National Health and Nutrition Examination Survey (NHANES) 2011 to 2014. Eur J Nutr. 2020;60(1):465–74.
Baker ML, Wang JJ, Rogers S, Klein R, Kuller LH, Larsen EK, Wong TY. Early age-related macular degeneration, cognitive function, and dementia: the Cardiovascular Health Study. Arch Ophthalmol. 2009;127(5):667–73.
Rosano C, Newman AB, Katz R, Hirsch CH, Kuller LH. Association between lower digit symbol substitution test score and slower gait and greater risk of mortality and of developing incident disability in well-functioning older adults. J Am Geriatr Soc. 2008;56(9):1618–25.
Swindell WR, Cummings SR, Sanders JL, Caserotti P, Rosano C, Satterfield S, et al. Data mining identifies digit symbol substitution test score and serum cystatin c as dominant predictors of mortality in older men and women. Rejuvenation Res. 2012;15(4):405–13.
Cheng G, Huang C, Deng H, Wang H. Diabetes as a risk factor for dementia and mild cognitive impairment: a meta-analysis of longitudinal studies. Intern Med J. 2012;42(5):484–91.
Morgenstern J, Groener JB, Jende JME, Kurz FT, Strom A, Göpfert J, et al. Neuron-specific biomarkers predict hypo- and hyperalgesia in individuals with diabetic peripheral neuropathy. Diabetologia. 2021;64(12):2843–55.
Ziegler D, Papanas N, Schnell O, Nguyen BDT, Nguyen KT, Kulkantrakorn K, et al. Current concepts in the management of diabetic polyneuropathy. J Diabetes Investig. 2020;12(4):464–75.
Kim S-H, Choi MK, Park NY, Hyun J-W, Lee MY, Kim HJ, et al. Serum neurofilament light chain levels as a biomarker of neuroaxonal injury and severity of oxaliplatin-induced peripheral neuropathy. Sci Rep. 2020;10(1).
van Lieverloo GGA, Wieske L, Verhamme C, Vrancken AFJ, van Doorn PA, Michalak Z, et al. Serum neurofilament light chain in chronic inflammatory demyelinating polyneuropathy. J Peripher Nerv Syst. 2019;24(2):187–94.
Xue M, Xu W, Ou Y-N, Cao X-P, Tan M-S, Tan L, et al. Diabetes mellitus and risks of cognitive impairment and dementia: a systematic review and meta-analysis of 144 prospective studies. Ageing Res Rev. 2019;55.
Giacomucci G, Mazzeo S, Bagnoli S, Ingannato A, Leccese D, Berti V, et al. Plasma neurofilament light chain as a biomarker of Alzheimer’s disease in subjective cognitive decline and mild cognitive impairment. J Neurol. 2022;269(8):4270–80.
He L, Morley JE, Aggarwal G, Nguyen AD, Vellas B, de Souto BP, et al. Plasma neurofilament light chain is associated with cognitive decline in non-dementia older adults. Sci Rep. 2021;11(1):13394.
Osborn KE, Khan OA, Kresge HA, Bown CW, Liu D, Moore EE, et al. Cerebrospinal fluid and plasma neurofilament light relate to abnormal cognition. Alzheimers Dement (Amst). 2019;11:700–9.
Ciardullo S, Muraca E, Bianconi E, Ronchetti C, Cannistraci R, Rossi L, et al. Serum neurofilament light chain levels are associated with all-cause mortality in the general US population. J Neurol. 2023.
Kurucu H, Colom-Cadena M, Davies C, Wilkins L, King D, Rose J, et al. Inhibitory synapse loss and accumulation of amyloid beta in inhibitory presynaptic terminals in Alzheimer’s disease. Eur J Neurol. 2022;29(5):1311–23.
Serrano-Pozo A, Frosch MP, Masliah E, Hyman BT. Neuropathological alterations in Alzheimer disease. Cold Spring Harb Perspect Med. 2011;1(1): a006189.
Fathy YY, Jonkman LE, Bol JJ, Timmermans E, Jonker AJ, Rozemuller AJM, et al. Axonal degeneration in the anterior insular cortex is associated with Alzheimer’s co-pathology in Parkinson’s disease and dementia with Lewy bodies. Transl Neurodegener. 2022;11(1):52.
O’Keeffe GW, Sullivan AM. Evidence for dopaminergic axonal degeneration as an early pathological process in Parkinson’s disease. Parkinsonism Relat Disord. 2018;56:9–15.
Tagliaferro P, Burke RE. Retrograde axonal degeneration in Parkinson disease. J Parkinsons Dis. 2016;6(1):1–15.
Dhana A, DeCarli C, Dhana K, Desai P, Wilson RS, Evans DA, et al. White matter hyperintensity, neurofilament light chain, and cognitive decline. Ann Clin Transl Neurol. 2023;10(3):321–7.
Nixon RA, Paskevich PA, Sihag RK, Thayer CY. Phosphorylation on carboxyl terminus domains of neurofilament proteins in retinal ganglion cell neurons in vivo influences on regional neurofilament accumulation, interneurofilament spacing, and axon caliber. J Cell Biol. 1994;126(4):1031–46.
Preische O, Schultz SA, Apel A, Kuhle J, Kaeser SA, Barro C, et al. Serum neurofilament dynamics predicts neurodegeneration and clinical progression in presymptomatic Alzheimer’s disease. Nat Med. 2019;25(2):277–83.
Acknowledgements
We thank all NHANES participants and staff for their excellent contributions to guarantee the completion of the present and other study. We thank Free Statistics team for providing technical assistance and valuable tools for data analysis and visualization.
Funding
No funding or sponsorship was received for this study or publication of this article. The Rapid Service Fee was funded by the authors.
Author information
Authors and Affiliations
Contributions
Yuanyuan Gao and Dan Su contributed to the conception, design, writing the manuscript. Zhouya Xue collected and analyzed the original data. Shu Wang and Lin Ji revised the manuscript. All authors contributed to drafting the paper and were involved in the approval of the final version.
Corresponding author
Ethics declarations
Conflict of Interest
Yuanyuan Gao, Dan Su, Zhouya Xue, Lin Ji, and Shu Wang declare that they have no competing interests.
Ethical Approval
The NHANES was authorized by the National Center for Health Statistics (NCHS) Ethics Review Committee, and all participants completed written informed consent forms before participation. The secondary analysis did not require additional Institutional Review Board approval. The authors adhered to the Declaration of Helsinki 1964.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Gao, Y., Su, D., Xue, Z. et al. Association Between Serum Neurofilament Light Chain and Cognitive Performance Among Older Adults in the United States: A Cross-Sectional Study. Neurol Ther 12, 2147–2160 (2023). https://doi.org/10.1007/s40120-023-00555-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40120-023-00555-9