
Abstract
Japanese encephalitis virus (JEV) belongs to arthropod-borne virus family, which are infectious agents transmitted by blood-sucking arthropods. They multiply in the tissues of the arthropod without evidence of disease or damage. The principal vector is Culex mosquito, most important being C. tritaenorhynchus, which is a rural mosquito, breeding extensively in rice fields and bites large domestic animals. In temperate zones, this vector is present in greatest density from June to November. The natural cycle of JEV consists of pig–mosquito–pig or bird–mosquito–bird cycle. Pigs serve as most important biological amplifiers and reservoirs. JEV is transmitted to humans through the bites of infected mosquitoes. Humans are accidental, dead-end hosts as they do not develop a level of viraemia sufficient to infect mosquitoes. The infection with JEV ranges from nonspecific febrile illness to a severe meningoencephalomyelitis illness. The risk for Japanese encephalitis varies by local ecology and season. In temperate areas of Asia, human disease usually peaks in summer and falls down after that and these seasonal epidemics can be explosive with thousands of cases occurring over a period of several months; whereas, in the subtropics and tropics, transmission can occur throughout the year, with disease at a peak during rainy season. A detailed study has been done on geographic distribution of JEV and incidence and burden of disease in India. Vaccination proves to be the best measure to protect the individual against any disease. So, large scale immunization of susceptible human population is highly important to prevent this deadly infection. In India, vaccinations against Japanese encephalitis are administered in areas where the disease is hyperendemic.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Japanese encephalitis (JE), one of the most common cause of acute encephalitis in tropics [1, 2], has generated considerable public anxiety in India. Caused by a neurovirulent RNA flavivirus, JEV and transmitted by mosquitoes, the occurrence of this disease highlights the inter relationship between man and animals, birds and the environment. Among an estimated 35,000–50,000 cases reported annually, approximately 20–30% of patients die and 30–50% of survivors suffer from neurological sequelae [3, 4]. The infection with JEV ranges from nonspecific febrile illness to a severe meningoencephalomyelitis illness [5]. The symptoms are serious and no definite treatment is available. JE is mainly a disease of children, but it can occur among persons of any age which is mostly travel related and is generally very rare [6–8]. Travellers living for prolonged periods in rural areas where JE is endemic or epidemic are at greater risk than short term and urban travellers.
Vaccination proves to be the best measure to protect the individual against any disease. Hence, large scale immunization of susceptible human population is highly important to prevent this deadly infection. In India, vaccinations against Japanese encephalitis are administered in areas where the disease is hyperendemic, like Gorakhpur region of Uttar Pradesh [9]. In the case of JE, it is essential to immunize the pigs (amplifying host) also to interrupt the transmission of disease [10]. Thus, control of vectors and intense immunization in endemic regions are the only effective preventive measure. The vaccines available for JE these days are of three types—(i) A Mouse-brain derived inactivated vaccine (only vaccine which is WHO approved), (ii) cell-culture derived inactivated JE vaccine (which was developed in China), and (iii) cell-culture derived live attenuated JE vaccine (which is the most cost-effective vaccine [11]). Apart from them, recombinant protein based vaccine and DNA vaccines are still in development process.
Historical Background
Japanese encephalitis was first recognised as a clinical entity in Japan in 1871; but the causative agent (JEV) was later isolated from a fatal human case in 1934 in Japan and was serologically and virologically established as a prototype (Nakayama) strain [12]. The Nakayama strain was later used in the development of mouse brain inactivated virus vaccine. It took almost 25 years after its first isolation, to elucidate the mode of transmission by mosquito vector. In last three decades, the focus of viral epidemics has changed from temperate zone of Asia to South and Southeast Asia [13]. In India, acute viral encephalitis was first detected in 1955 and since then, it has taken away thousands of lives. Several encephalitis outbreaks reported in the later years remained undiagnosed.
Ecology and JEV Transmission
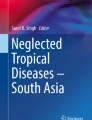
JEV belongs to arthropod-borne virus family (arboviruses), which are a group of infectious agents that are transmitted by blood-sucking arthropods. They multiply in the tissues of the arthropod without evidence of disease or damage. The principal vector of this zoonotic disease is Culex mosquito, most important being C. tritaenorhynchus, others are C. vishnui and C. pseudo-vishnui [14, 15], which are primarily rural mosquitoes breeding extensively in rice fields and preferentially bite large domestic animals like pigs and wading birds [16]. In temperate zones, this vector is present in greatest density from June to November. The natural cycle of JEV consists of pig–mosquito–pig or bird–mosquito–bird cycle (Fig. 1). Other minor hosts are cattle, buffaloes, goats, sheep, horses, rodents, monkeys, dogs and bats [17].

Transmission cycle of Japanese encephalitis virus (JEV). JEV is transmitted in an enzootic cycle between Culex mosquitoes and amplifying vertebrate hosts, primarily pigs and wading birds like water fowls and egrets. Human beings serve as a dead-end host in the JEV transmission cycle with low levels of viremia. Humans play no role in the maintenance or amplification of JEV, and the virus is not transmitted directly from person to person
Pigs are the most important biological amplifiers and reservoirs [18]. Countries, like Pakistan, that do not rear pigs experience rare JE cases [19]. In the study done on rural children in Thanjavur district (Tamil Nadu), an area with extensive paddy cultivation, JE occurrence was found to be very low and without epidemics. The reason could possibly be high cattle to pig ratio (400:1) [20]. JEV is transmitted to humans through the bites of infected mosquitoes. Humans usually do not develop a level of viraemia sufficient to infect mosquitoes [21]. Therefore, humans are accidental, dead-end hosts, and human JE cases imported into non-endemic areas represent a minimal risk for subsequent transmission of the virus [22]. Direct person-to-person spread of JEV does not generally occur until and rarely it is through intrauterine transmission [23, 24]. Blood transfusion and organ transplantation may also serve as potential mode of JEV transmission [25]. The risk for JE varies by local ecology and season. In temperate areas of Asia, human disease usually peaks in summer and falls down after that [26–28] and these seasonal epidemics can be explosive with thousands of cases occurring over a period of several months; whereas, in the subtropics and tropics, transmission can occur throughout the year, with disease at a peak during rainy season. A recent study in China has correlated the different weather variables like temperature, relative humidity as possible predictors of Japanese encephalitis incidence for regions with similar geographic, weather and socio-economic conditions [29]. However in endemic areas (e.g., southern India) sporadic cases may occur throughout the year due to congenial climatic conditions [30].
Geographic Distribution of JE
Japanese encephalitis occurs throughout Asia and parts of the Western Pacific areas (Fig. 2). The disease was recognized in the first half of 20th century in the temperate areas of Asia, mainly Japan, Korea, Taiwan and mainland China [31–33]; but over the past few decades, the disease appears to have spread to Southeast Asia, India, Bangladesh, Sri Lanka and Nepal [34–37]. By 1990s, JEV had spread to non-Asian regions, Saipan and Australia, where it was reported first from Torres Strait islands and then from northern mainland [38, 39]. The reasons for this wide distribution can be population shifts or changes in climate, ecology, agricultural practices, animal husbandry or migrating bird patterns [40]. Though exact cause is uncertain, these factors could very well contribute to further spread, potentially beyond Asia and Western Pacific.

Approximate geographic range (epidemiology) of Japanese encephalitis highlighting the areas which are engulfed by Japanese encephalitis virus
Incidence and Burden of Disease in India
In India, the disease has been recognized since 1945 and though virus causes epidemics, it is endemic in several parts of the country [41–44]. The earliest evidence of the prevalence of JE virus was cited through serological studies carried out at the Virus Research Centre, Pune in 1952 and then in 1956, the isolation of JE virus was made from the wild caught mosquitoes, establishing its presence in India. However, the virus could not be recovered from human until 1958, when three isolations were made from the brain tissue of encephalitis cases in Tamil Nadu [45]. The geographic area affected by JEV has expanded in the last 60 years with higher epidemic activity in North India and Central India (Fig. 3). Since the confirmation of first clinical case of JE from Vellore in 1955 [46], there had been many major JE outbreaks reported from Bihar, Uttar Pradesh, Assam, Manipur, Andhra Pradesh, Karnataka, Madhya Pradesh, Maharashtra, Tamil Nadu, Haryana, Kerala, West Bengal, Orissa and Union Territories of Goa and Pondicherry [47, 48].

Approximate display of JE occurrence areas in India. Different colours in the map highlight the intensity by which JEV occurs in different areas
Carey et al. [49] had reported almost 65 JE cases from South India from 1955 to 1966 by demonstrating specific neutralizing antibodies to JE. In its first major outbreak in West Bengal, JE had taken about 300 lives from the two districts, Burdwan and Bankura in 1973 [50]. During 1978, several outbreaks of JE occurred in different parts of India viz. Kolar district of Karnataka, Tirunelvelli, Benpura, Burdwan and adjoining areas of West Bengal, Dhanbad district of Bihar, Dibrugarh district in Assam, Goa on the west coast [42] and eastern districts of Uttar Pradesh [41], which was one of the worst JEV outbreaks. From this outbreak, a successful isolation and identification of JE virus as the causative agent was made from the brain tissue of a fatal case of encephalitis from Gorakhpur district for the first time by Asha Mathur and her team at the King Georges’ Medical College, Lucknow [41]. Outbreak of JE was again reported in 1981 from South Arcot district [46] and from Gorakhpur in 1988 with as much as around 875 cases reported [51]. Eastern paddy growing districts of Haryana suffered an epidemic of encephalitis in 1990 [43] and Muzaffarpur district of Bihar in 1995. JE had emerged as a major public health problem in naive non-endemic area like Kerala [52], where a large outbreak of JE occurred in Kuttanad area of Allepey district [53]. In a severe epidemic of JE during October–November 1999 in Andhra Pradesh, out of 23 districts, fifteen districts were affected with 873 cases and about 20% mortality [54]. Another outbreak occurred in July 2003 in Warangal and Karim Nagar district of Andhra Pradesh [55]. From north-east regions, JE outbreaks which were reported from Assam during July–August 1989, had affected a population of ~36,000 with 50% case fatality rate [56]. After that, several other outbreaks have been reported from Assam between 2000 and 2002 [57].
Thus, encephalitis by JEV that was known to cause epidemics in several parts of the country now has become endemic in many parts of India, especially in South India [58] (including Tamil Nadu [47]) and terrain belt of Uttar Pradesh [59], which is a matter of serious public health problem. In Uttar Pradesh, the most severely JE affected region is Gorakhpur and the longest epidemic in three decades, had been reported from this district from July to November, 2005, in which 5,737 people were affected and approximately 1,344 died [60]. More recent studies on phylogeny of virus revealed that the epidemic was caused by JEV GP78 [61]. Gorakhpur and surrounding region in Uttar Pradesh still gets consistent outbreaks of fatal acute encephalitis syndrome (AES), of which ~10–15% is caused by JEV [62].
Among children in endemic zone, the incidence of laboratory confirmed JE varies widely areawise, the range being 5–50 cases per 100,000 children/year [28, 63]. The number of affected persons is magnified also because of many non-JE cases with unidentified etiologies. So, now the cases are classified as JE and non-JE and enterovirus 89 and 76 were isolated from the CSF of non-JE encephalitis cases from Gorakhpur in 2006 [11].
Japanese Encephalitis Virus
Four Flaviviral infections, of which three are encephalitis, are transmitted by mosquitoes from birds [64]. Clinically the most serious of these infections is “Japanese encephalitis”, caused by Japanese encephalitis virus (JEV). The North Indian strain of Japanese encephalitis virus (JEV) is GP78, which is phylogenetically closer to the Chinese SA14 isolate. The other, Vellore P20778 isolate, was obtained from southern India in 1958 [65]. JEV is an enveloped virus and has a linear, single stranded, positive-sense ~11 kb long RNA as a genome and measures 40–50 nm in diameter with a nucleocapsid which is surrounded by a lipid envelope (Fig. 4). The genomic RNA contains a single open reading frame (ORF) and codes for a polyprotein of ~3,400 amino acids. This polyprotein is cleaved by viral and host proteases into ten proteins: three structural proteins (capsid, M and E proteins) and seven non-structural proteins [66] (NS1, 2A, 2B, 3, 4A, 4B & 5). Envelope or E defines the type specificity. The viral RNA has non-coding regions of 95 and 585 bases at 5′ and 3′ ends which interact with viral or host proteins which are important for virus replication [67]. Looking at the regular epidemics of JE, studies are being conducted to look for any mutation with the viral genome and as demonstrated by Pujhari et al. [68] a novel mutation was detected in domain II of the envelop gene of JEV circulating in North India. More studies are required to ascertain its role in JE pathogenesis.

Morphology of the Japanese encephalitis virus and the detailed display of the organisation of viral genome highlighting the structural and non-structural genes and also the structure of protein extracted
Genotypes of Japanese Encephalitis Virus
Epidemics of encephalitis were described in Japan from 1870s onwards and have subsequently been found across most of Asia [3]. For most of the major human pathogens, we have little idea about where they have originated. Because JEV has so rapidly spread to new areas, tracing its geographical origin has been somewhat possible [69] and phylogenetic comparison with other flaviviruses suggest that it evolved from an ancestral virus a few centuries ago. Five genotypes of JEV have been identified based on nucleotide sequences of C/PrM and E genes: Genotype 1 to 5 [70]. Among the five, GIV and GV appeared rarely. Genotype 1 (GI) is found to be circulating in northern Thailand, Cambodia and Korea. It has been less associated with human disease than genotype 3 in China; but a recent study reported isolation of genotype 1 (GI) from a vaccinated boy who developed JE [71]. Genotype 2 (GII) includes isolates from southern Thailand, Malaysia, Indonesia and Northern Australia. Isolates from temperate regions of Asia i.e. Japan, China, Taiwan, Philippines, Vietnam, Sri Lanka, Nepal and India has been put in Genotype 3 (GIII), whereas GIV includes isolates from Indonesia only [72]. GV included only a single strain isolated from a patient from Mummer, Malaysia in 1952 [73]. Since all five genotypes have been found in the Indonesia Malaysia region, it is likely that these current five genotypes evolved around the same region (Fig. 5). GI and GIII occur in epidemic regions, whereas GII and GIV are associated with endemic disease [3].

Sequence phlylogeny of JEV isolates. Sequence phylogeny of Japanese encephalitis virus isolates from Gorakhpur (India) 2005 epidemic, with reference to other Southeast Asian isolates and flaviviruses based on partial E gene sequence. The tree was generated by neighbor-joining method. Bootstrap values are indicated at the branch points. DEN, WNV, KUN, SLEV and MVE denotes Dengue virus, West Nile virus, Kunjin virus, Saint Louis encephalitis virus and Murray Valley encephalitis virus respectively [61]
JEV is naturally transmitted between vertebrate hosts by Culex and other mosquitoes. The reasons for its spread are uncertain but many include changing agricultural practices, such as increasing irrigation and animal husbandry [74]. JEV continues to spread with recent outbreaks in India, Nepal and Australia. GIII is most widely distributed and was the only genotype found in India till 2007 [62]. However, in a recent study done by Fulmali and his co-workers demonstrated simultaneous detection and isolation of GI and GIII JEV strains from 66 acute encephalitis syndrome (AES) patients. Clinical syndrome for the two strains was indistinguishable. Thus GI and GIII detection indicates their co-circulation and association with human infections in Gorakhpur region [9]. GI isolate from India has been found to share close relationship with GI strain from Japan and Korea. GIII was the major genotype circulating in Japan, Korea and Vietnam until the early 1990s. However, by mid 1990, G III disappeared in Japan and Vietnam and GI supplanted it. This phenomenon is called “Genetic Shift” [75]. In Japan, JEV has been shown to overwinter and settle [76]. In India, the exact mode of introduction of GI JEV is not clear. It is possible that it may have been introduced into India through migratory birds like other Asian countries [77]. More studies are required to establish the role of migratory birds in JE transmission.
Pathology and Pathogenesis
A considerable degree of variation exists in neurovirulence and peripheral pathogenicity among JE virus strains and the mechanism of JEV pathogenesis is still unclear [78]. It has also been noted that typical pathological changes associated with each epidemic varied dramatically [79]. After the virus gets inoculated into the skin by the bite of an infected mosquito, it is quickly disseminated in the body and proliferates in the reticuloendothelial system. There is a transient period of viremia after which invasion of the central nervous system occurs. JEV is thought to invade brain via vascular endothelial cells by endocytosis [80], which involve clathrin and membrane cholesterol, referred to as lipid rafts acting as portals for virus entry [81]. In brain, the distribution of virus is in the thalamus, hippocampus, substantia nigra and medulla oblongata [82]. In the neurons, JEV replicates and matures in the neuronal secretary system. Neurocysticercosis (NCC) in 33% of patients dying with JE has been seen, but in only 1% of patients dying due to other causes, suggesting that NCC may somehow predispose to JE [79, 83]. A high level of tumour necrosis factor is correlated with adverse outcome in JE [84].
Clinical Spectrum
The majority of human infections with JEV are asymptomatic with proportion of apparent to inapparent JEV infection found to be 1:300 to 1:1000 during epidemics [85]. In a study of JE infection in Assam, the ratio of apparent to inapparent infection was shown to be 9.1:100 [86]. Milder forms of disease (e.g. aseptic meningitis or undifferentiated febrile illness) can also occur, but have been reported more commonly among adults [87]. JE affects all age groups, with higher incidence in children aged <15 years of age [37, 88]. However, in countries (China and Japan) with childhood JE immunization programmes, the overall incidence of JE has decreased and similar numbers of cases are observed among children and adults [89, 90]. Because unvaccinated travellers from non endemic countries usually are immunologically naive, travel associated JE can occur in persons of any age [22].
Among patients, who develop clinical symptoms, the incubation period is 5–15 days. Table 1 shows the course of disease which is divided into three stages—prodromal stage, acute encephalitic stage and late convalescent stage. Fatality in JE patients is usually seen within 24–48 h of admission [91] and among the survivors; at least one in 200 affected individuals develop severe psychoneurological sequelae [92] in the form of parkinsonism [93], convulsive disorders, motor abnormalities, impaired intellect, hearing deficit, scholastic backwardness, speech disturbances [94] and other subtle neurological signs. Movement disorders have also been observed [95]. The disease can be much more difficult to detect in infants.
Immune Mechanism Against JE Infection
After the entry, JE virus is partially destroyed at the site of its entry and the remaining virus is disseminated by local and systemic extra neural replication leading to viraemia. After primary infection with JEV, presence of IgM antibodies and T-lymphocytes are seen until about 2 weeks [96, 97]. But antibodies alone are neither capable of terminating the viraemia nor preventing the subsequent infection [98]. Pregnancy is known to cause immunosuppression and persistent maternal infection or pregnancy induced reactivation of the virus may cause foetal infection. Isolation of JEV from human placenta and foetuses has been reported by Chaturvedi et al. [23], whereas Mathur et al. [24] have described an animal model of congenital infection with JEV, showing an active replication of virus in placenta. They have also shown transplacental transmission of virus during consecutive pregnancies of mice. JEV can establish latency within different organs despite the presence of antiviral antibodies [99]. Immunological and virological evidence for persistence of JEV have been described in human nervous system also [100]. Latent and recurrent infection as a consequence of activation of latent JEV has been reported in humans [101].
A significant decrease in serum iron levels, a frequent feature of microbial invasion is observed during JE infection [102, 103]. An early influx of macrophages followed by neutrophils at the site of injury in different organs in humans [104] and mice [105] has been reported, which is correlated with the production of a neutrophil chemotactic macrophage derived factor, MDF [106], with development of hypoglycaemia [107, 108]. This chemotactic protein (MDF) has been shown to play a protective role in the host defence against JEV, through production of reactive oxygen intermediates [109] in neutrophils and reactive nitrogen oxide species [110] degrading the virus protein and RNA. In other studies, mechanism of proinflammatory cytokine [111] and cytokine secretion at molecular level has been studied and the involvement of monocyte and macrophage receptor, CLEC5A, in severe inflammatory response in JEV infection of brain is reported [112]. Misra et al. [113] have found increased levels of proinflammatory and anti-inflammatory cytokines and monocyte chemoattractant protein-1 in the serum of rats after JEV infection. The mechanism of JEV pathogenesis is still unclear [78]. For the development of appropriate and effective therapy there is an immediate requirement to understand the role of host factors in JEV-induced neuropathogenesis [114].
Laboratory Diagnosis
Clinical findings with JE are nonspecific and might include moderately elevated white blood cell count, mild anaemia and hyponatremia [22, 115]. The clinical suspicion of encephalitis can be supported with CSF analysis [30, 115]. Usefulness of various conventional magnetic resonance imaging (MRI) of the brain is better than computed tomography for detecting JEV associated changes [116]. Recently the utility and usefulness of various conventional MRI sequences in the diagnosis of acute viral encephalitis has been evaluated. Viral encephalitis patients were assessed by clinical evaluation and confirmation was done by analyzing serum or CSF for dengue, JE, herpes, measles, echo, coxsackie and polio viruses using ELISA or PCR. It was found that the MRI changes are correlated with type of encephalitis and duration of illness [117].
In India, the actual JE burden could be estimated only by strengthening diagnostic facilities for JE confirmation in hospitals [10]. The laboratory diagnosis of a confirmed case of Japanese encephalitis is based on either isolation of virus from specimen or by antibody detection. Because humans have low or undetectable levels of viremia by the time distinctive clinical symptoms are recognized, virus isolation and nucleic acid amplification tests (NAAT) are insensitive and should not be used for ruling out a diagnosis of JE [22]. For rapid diagnosis of JE, detection of antigen in CSF using immunofluorescence [118] and reverse passive haemagglutination [119] using poly or monoclonal antibodies has been successful. The reverse transcriptase polymerase chain reaction amplification of viral RNA may help in rapid detection of JEV in samples [13].
Acute phase specimens are tested for JEV-specific IgM antibodies using a capture enzyme-linked immunosorbent assay (MAC-ELISA) [22]. Many modifications of MAC-ELISA such as nitrocellulose membrane based IgM capture dot enzyme immunoassay (Mac DOT), Avidin biotin system (ABC Mac ELISA), biotin labelled immunosorbent assay to sandwich ELISA and antibody capture radioimmunoassay (ACRIA) have been successfully tested for antibody detection [13]. Therefore, a positive IgM test has good diagnostic predictive value, but cross-reaction with arboviruses from same family can occur. The performance of three commercial JEV IgM antibody capture ELISA (MAC ELISA) kits has been evaluated with acute encephalitis specimens from India and Bangladesh and were found to be having high specificity (95–99.5%), but low sensitivities (15–57%) [120]. The two commercially available kits in India: Japanese encephalitis—Dengue IgM combo ELISA (Panbio Diagnostics) and JEV-Chex IgM capture ELISA (Cyton Diagnostics Limited) for the diagnosis of Japanese encephalitis in field samples have also been compared recently, in which the sensitivity and specificity were found to be 63.6 and 98.4% respectively for XCyton ELISA and 75 and 97.7% for Panbio ELISA [121].
Treatment and Management
There is no specific treatment or specific antiviral agent or other medication to mitigate the effects of JEV infection [122]. Thus it becomes highly important that the infection be managed carefully. Only one in every six deaths is directly due to JE virus and five out of six are preventable with prompt and early management, thus bringing down the case fatality rate of JE from 35–50% to less than 6% [30]. In different studies, monoclonal antibodies [13], corticosteroids, interferon alpha-2a or ribavirin have not been shown to improve clinical outcome [22]. Swarup et al. [123] have shown the effect of rosamarinic acid (RA) as an efficient antiviral agent that reduced JE viral load along with proinflammatory cytokines in experimental animals. Therapeutic role of diethyldithiocarbamate (Anti JEd) have been demonstrated during JEV infection [124]. Nazmi et al. [125] have demonstrated an effective way to counter the virus through inhibiting viral replication by using anti-sense molecules (Vivo-Morpholino) directed against the viral genome. Mycophenolic acid has been found to inhibit the replication of JEV in vitro and protected mice in vivo [126].
Outcome and Sequelae
JE has a case-fatality ratio of approximately 20–30% [22, 37, 123] and although some motor deficits improve after acute illness, 30–50% survivors have neurologic or psychiatric sequelae for years [123, 127]. Drug therapy and physiotherapy are necessary for survivors with sequelae like seizures, paralysis, movement disorders, Parkinsonism and psychiatric problems [30]. Also recurrence of symptoms after recovery with fresh neurologic deficits can occur as the virus remains latent in peripheral lymphocytes, and can later cause recurrence [99].
Prevention and Control
Preventive measures are very important for minimizing JE infection. Vector control should include measures such as eliminating potential mosquito breeding areas, shifting pigsties and environmental sanitation. Reduction of breeding source for larvae can be done by water management system with intermittent irrigation system, which is nothing but a strategy of alternate drying and wetting water management system in the rice fields. Equine and swine in affected areas should be vaccinated [10]. For humans in endemic areas, vaccination should be implemented, as well as personal protective measures. Vector control alone cannot be relied upon to prevent JE. Rapid identification and diagnosis is important for protecting the public and our livestock from this disease. For the disinfection, Biosafety level three precautions and practices are recommended for investigators working with this virus [128].
Vaccination
In the last five decades, JE has been effectively controlled and virtually eliminated in Japan, Taiwan, China and Korea after implementation of childhood immunization programs using inactivated mouse brain derived vaccine [129]. In Cambodia, JE surveillance commenced in 2006, and an immunization program has been planned [130]. Therefore, vaccination of the population at risk against JE, appears to be the most important control measure now, and in the future. At present, three types of vaccines are in use worldwide (Table 2 ).
-
(i)
Formalin-inactivated mouse brain derived vaccine is the only WHO approved vaccine. Asian field trials have shown that two doses (1–2 weeks apart) provide an efficacy of 91% [131]. However, three doses (0, 1 and 6 months) are being followed to immunize children in endemic zone. The vaccine is contraindicated for women who are pregnant and those who are immunocompromised. It is also being produced from Beijing-1 strain due to its high cross-reactivity among the JEV strain. The vaccine is being manufactured by Research Institute, Kasauli in India [132]. Vaccine has some common allergic reactions like fever, headache, malaise, dizziness, erythema, swelling and tenderness [133]. The mucocutaneous and neurologic allergic reactions reported after JE vaccination, may vary in frequency, and therefore these should be evaluated very carefully yearly [133]. Though safe and effective, the vaccine has limitations in terms of cost, availability and lack of long term immunity.
-
(ii)
Inactivated primary hamster kidney cell derived vaccine has been developed in China. The efficacy was found to be 76–90% in a field trial in China [134] and there were fewer side effects. A vero-cell culture derived inactivated vaccine from attenuated SA 14-14-2 strain has been developed, which induced high titers of neutralizing antibodies in experimental animals [135]. Another vero cell-culture derived inactivated JE vaccine using Indian isolate (P 20778) has been developed. It generated high titers of anti-JEV antibodies in mice [136].
-
(iii)
A cell-culture derived live, attenuated SA 14-14-2 vaccine from China has recently become internationally available and is increasingly replacing the inactivated, mouse brain-derived vaccine in Asia. A single dose of the vaccine demonstrated 96% efficacy after 5 years [137]. The vaccine is very cost-effective and appears to be safe and neuroattenuation is stable [13]. The government of India introduced the SA 14-14-2 vaccine in 2006, and nearly 50 million children 1–15 years of age have been reached through vaccination campaigns and routine immunization [138].
JE vaccine candidates in late-stage of development include a live, attenuated chimeric virus vaccine (IMOJEV®) and an inactivated Vero cell-derived vaccine; each based on the SA 14-14-2 strain. IMOJEV® (previously known as ChimeriVax™—JE), is a novel recombinant chimeric vaccine, developed using the yellow fever virus (YFV) vaccine vector as its backbone. It is found to be safe, highly immunogenic and capable of inducing long-lasting immunity in both preclinical and clinical trials [139]. Additionally, 2 inactivated, Vero cell-derived vaccines based on the Beijing-1 strain are being developed in Japan [140]. Second generation recombinant vaccines are also being developed, where signal sequences of PrM with genes encoding PrM and E proteins are packaged into vectors, e.g. E. coli and vaccinia [141]. Studies on plasmid DNA-based JEV vaccine are also giving promising results on experimental animals [142] and in one of the study; the JEV candidate DNA vaccine was capable of generating protective levels of neutralizing antibodies in rhesus monkeys [143]. DNAzymes (Dzs) that cleave the RNA sequence of the 3′-NCR of JEV genome in vitro, on intra-cerebral administration in JEV-infected mice led to more than 99.99% inhibition of virus replication in brain, resulting in a dose-dependent extended life-span or complete recovery of the infected animals [144]. New vaccine development, along with progress in surveillance and immunization, offers promise for sustainable control of clinical JE. To achieve this, global partners are working together to develop a strategic plan for JE control by 2015 [145].
Future Challenges
Currently in India, since the risk of JE is limited to focal areas, its immunization is not included in the National Immunization Program. It is recommended for active immunization only in JE prone areas [30]. There is a need for a proper pilot trial on JE vaccination involving hyperendemic districts for making a policy on mass JE vaccination in the community. JE vaccination should be considered in travelers, who are likely to spend >30 days in a JE-endemic country or travelers on brief trips if they have extensive outdoor or night time exposure in rural areas during periods of active transmission [22, 146]. It is also been reported that routine availability of vaccine and information, education and communication strategies play important roles in improving knowledge and achieving high vaccination rates [147]. For the development of effective therapy, there is an immediate requirement to understand the host factors in JEV-induced neuropathogenesis [109]. Because the live attenuated JE vaccine used in India is derived from GIII strain SA14-14-2, vaccine’s efficacy to protect against GI must be evaluated. Also the expansion of GI JEV into other parts of India should be continuously tracked [9]. It is also necessary to elucidate the ecology of migrating reservoir animals. Genotyping of both the mosquitoes and JEV should be done concurrently at many locations in temperate and tropical regions simultaneously. Any distinct biological markers, like susceptibility of replaced strains in mosquitoes, birds etc. should be elucidated.
References
Halstead SB, Jacobson J (2008) Japanese encephalitis vaccines. In: Plotkin SA, Orenstein WA, Offit P (eds) Vaccines, 45th edn. Saunders Elsevier, Philadelphia 311–352
Erlanger TE, Weiss S, Keiser J et al (2009) Past, present, and future of Japanese encephalitis. Emerg Infect Dis 15:1–7
Solomon T, Dung NM, Kneen R et al (2000) Japanese encephalitis. J Neurol Neurosurg Psychiatry 68:405–415
World Health Organization (2006) Sixteenth meeting of the technical advisory group on immunization and vaccine preventable diseases in the Western Pacific Region; Manila, Philippines. Available from http://www.wpro.who.int/NR/rdonlyres/1B75A8B9-2F00-4559-9A1F-C55C24A69304/0/MTGRPT_TAG16.pdf
Solomon T, Dung NM, Kneen R et al (2002) Seizures and raised intracranial pressure in Vietnamese patients with Japanese encephalitis. Brain 125:1084–1093
Centers for Disease Control and Prevention (CDC) (2009) Japanese encephalitis among three U.S. Travelers returning from Asia, 2003–2008. MMWR Morb Mortal Wkly Rep 58:737–740
Hills SL, Griggs AC, Fischer M (2010) Japanese encephalitis in travelers from non-endemic countries, 1973–2008. Am J Trop Med Hyg 82:930–936
Marfin AA, Eidex RS, Kozarsky PE et al (2005) Yellow fever and Japanese encephalitis vaccines: indications and complications. Infect Dis Clin North Am 19:151–168
Fulmali PV, Sapkal GN, Athawale S et al (2011) Introduction of Japanese encephalitis virus genotype I, India. Emerg Infect Dis 17:319–321
Kabilan L, Rajendran R, Arunachalam N et al (2004) Japanese encephalitis in India: an overview. Indian J Pediatr 71:609–615
Saxena V, Dhole TN (2008) Preventive strategies for frequent outbreaks of Japanese encephalitis in Northern India. J Biosci 33:505–514
Miyake M (1964) The pathology of Japanese encephalitis: a review. Bull World Health Organ 30:153–160
Tiroumourougane SV, Raghava P, Srinivasan S (2002) Japanese viral encephalitis. Postgrad Med J 78:205–215
Sucharit S, Surathin K, Shrestha SR (1989) Vectors of Japanese encephalitis virus (JEV): species complexes of the vectors. Southeast Asian J Trop Med Public Health 20:611–621
Arunachalam N, Samuel PP, Hiriyan J et al (2004) Japanese encephalitis in Kerala, South India: can Mansonia (Diptera: Culicidae) play a supplemental role in transmission? J Med Entomol 41:456–461
Rosen L (1986) The natural history of Japanese encephalitis virus. Annu Rev Microbiol 40:395–414
Mall MP, Kumar A, Malik SV (1995) Sero-positivity of domestic animals against Japanese encephalitis in Bareilly area, U.P. J Commun Dis 27:242–246
Gubler DJ, Rochrig JT (1998) Arboviruses (Togaviridae and Flavivirdae). In: Collier L, Balows A, Sussman M (eds) Topley & Wilson’s microbiology and microbial infection, 9th edn. Arnold, London, pp 579–600
Igarashi A, Tanaka M, Morita K (1994) Detection of West Nile and Japanese encephalitis viral genome sequences in cerebrospinal fluid from acute encephalitis cases in Karachi, Pakistan. In: Takasu T, Ahmed A (eds) Subacute sclerosing panencephalitis: a neuro- viro- patho- epidemio- entomological survey, 1st edn. Karachi Encephalitis Survey Team Secretariat, Tokyo, pp 135–142
Vijayarani H, Gajanana A (2000) Low rate of Japanese encephalitis infection in rural children in Thanjavur district (Tamil Nadu), an area with extensive paddy cultivation. Indian J Med Res 111:212–214
Misra UK, Kalita J (2001) Seizures in Japanese encephalitis. J Neurol Sci 190:57–60
Centers for Disease Control and Prevention (CDC) (2010) Japanese encephalitis vaccines: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep 59(RR-1):1–27
Chaturvedi UC, Mathur A, Chandra A, Das SK et al (1980) Transplacental infection with Japanese encephalitis virus. J Infect Dis 141:712–715
Mathur A, Arora KL, Chaturvedi UC (1981) Congenital infection of mice with Japanese encephalitis virus. Infect Immun 34:26–29
Pealer LN, Marfin AA, Petersen LR et al (2003) Transmission of West Nile virus through blood transfusion in the United States in 2002. N Engl J Med 49:1236–1245
Yongxin Y (1995) Japanese encephalitis in China. Southeast Asian J Trop Med Public Health 26(suppl 3):17–21
Tam N, Yen N (1995) Japanese encephalitis in Vietnam 1985–93. Southeast Asian J Trop Med Public Health 26(suppl 3):47–50
Wu YC, Huang YS, Chien LJ et al (1999) The epidemiology of Japanese encephalitis on Taiwan during 1966–1997. Am J Trop Med Hyg 61:78–84
Lin H, Yang L, Liu Q et al (2011) Time series analysis of Japanese encephalitis and weather in Linyi City, China. Int J Public Health 10:1–8
Rao PN (2001) Japanese encephalitis. Indian Pediatr 38:1252–1264
Sohn YM (2000) Japanese encephalitis immunization in South Korea: past, present, and future. Emerg Infect Dis 6:17–24
Yamanaka A, Mulyatno KC, Susilowati H et al (2010) Prevalence of antibodies to Japanese encephalitis virus among pigs in Bali and East Java, Indonesia, 2008. Jpn J Infect Dis 63:58–60
Shimojima M, Nagao Y, Shimoda H et al (2011) Full genome sequence and virulence analyses of the recent equine isolate of Japanese encephalitis virus. J Vet Med Sci 73:813–816
Umenai T, Krzysko R, Bektimirov TA et al (1985) Japanese encephalitis: current worldwide status. Bull World Health Organ 63:625–631
Joshi D (1986) Japanese encephalitis in Nepal. JE HFRS Bull 1:5–15
Chunsuttiwat S, Warachit P (1995) Japanese encephalitis in Thailand. Southeast Asian J Trop Med Public Health 26(suppl 3):43–46
Bista MB, Shrestha JM (2005) Epidemiological situation of Japanese encephalitis in Nepal. J Nepal Med Assoc 44:51–56
van den Hurk AF, Ritchie SA, Mackenzie JS (2009) Ecology and geographical expansion of Japanese encephalitis virus. Annu Rev Entomol 54:17–35
Hanna JN, Ritchie SA, Phillips DA et al (1999) Japanese encephalitis in north Queensland, Australia, 1998. Med J Aust 170:533–536
Keiser J, Maltese MF, Erlanger TE et al (2005) Effect of irrigated rice agriculture on Japanese encephalitis, including challenges and opportunities for integrated vector management. Acta Trop 95:40–57
Mathur A, Chaturvedi UC, Tandon HO et al (1982) Japanese encephalitis epidemic in Uttar Pradesh, India during 1978. Indian J Med Res 75:161–169
Mohan Rao CV, Prasad SR, Rodrigues JJ, Sharma NG et al (1983) The first laboratory proven outbreak of Japanese encephalitis in Goa. Indian J Med Res 78:745–750
Prasad SR, Kumar V, Marwaha RK et al (1993) An epidemic of encephalitis in Haryana: serological evidence of Japanese encephalitis in a few patients. Indian Pediatr 30:905–910
Saxena SK, Singh M, Pathak AK, Mathur A (2006) Reply to ‘Encephalitis outbreak finds Indian officials unprepared’. Nat Med 12:269–270
Webb JKG, Pavri K, George S et al (1964) Asian Paediatrics, the scientific Proceedings of the first all Asian Congress of Paediatrics. Asia Publishing House, Bombay
Namachivayam V, Umayal K (1982) Profile of the 1981 epidemic of encephalitis in South Arcot district. In: Proceedings of the national conference on Japanese encephalitis. ICMR, pp 30–33
Kabilan L, Vrati S, Ramesh S, Srinivasan S et al (2004) Japanese encephalitis virus (JEV) is an important cause of encephalitis among children in Cuddalore district, Tamil Nadu, India. J Clin Virol 31:153–159
Potula R, Badrinath S, Srinivasan S (2003) Japanese encephalitis in and around Pondicherry, South India: a clinical appraisal and prognostic indicators for the outcome. J Trop Pediatr 49:48–53
Carey DE, Reuben R, Myers RM (1968) Japanese encephalitis studies in Vellore, South India. I. Virus isolation from mosquitoes. Indian J Med Res 56:1309–1318
Chakravarty SK, Sarkar JK, Chakravarty MS et al (1975) The first epidemic of Japanese encephalitis studied in India—virological studies. Indian J Med Res 63:77–82
Rathi AK, Kushwaha KP, Singh YD et al (1993) JE virus encephalitis: 1988 epidemic at Gorakhpur. Indian Pediatr 30:325–333
Reuben R, Gajanana A (1997) Japanese encephalitis in India. Indian J Pediatr 64:243–251
Dhanda V, Thenmozhi V, Kumar NP et al (1997) Virus isolation from wild-caught mosquitoes during a Japanese encephalitis outbreak in Kerala in 1996. Indian J Med Res 106:4–6
Rao JS, Misra SP, Patanayak SK et al (2000) Japanese Encephalitis epidemic in Anantapur district, Andhra Pradesh (October–November, 1999). J Commun Dis 32:306–312
Das BP, Lal S, Saxena VK (2004) Outdoor resting preference of Culex tritaeniorhynchus, the vector of Japanese encephalitis in Warangal and Karim Nagar districts, Andhra Pradesh. J Vector Borne Dis 41:32–36
Vajpayee A, Dey PN, Chakraborty AK et al (1992) Study of the outbreak of Japanese encephalitis in Lakhimpur district of Assam in 1989. J Indian Med Assoc 90:114–115
Phukan AC, Borah PK, Mahanta J (2004) Japanese encephalitis in Assam, northeast India. Southeast Asian J Trop Med Public Health 35:618–622
Gajanana A, Rajendran R, Samuel PP et al (1997) Japanese encephalitis in south Arcot district, Tamil Nadu, India: a three-year longitudinal study of vector abundance and infection frequency. J Med Entomol 34:651–659
Kar NJ, Bora D, Sharma RC et al (1992) Epidemiological profile of Japanese encephalitis in Gorakhpur district, Uttar Pradesh, 1982–1988. J Commun Dis 24:145–149
Parida M, Dash PK, Tripathi NK et al (2006) Japanese encephalitis outbreak, India, 2005. Emerg Infect Dis 12:1427–1430
Saxena SK, Mishra N, Saxena R, Singh M, Mathur A (2009) Trend of Japanese encephalitis in North India: evidence from thirty-eight acute encephalitis cases and appraisal of niceties. J Infect Dev Ctries 3:517–530
Sapkal GN, Bondre VP, Fulmali PV et al (2009) Enteroviruses in patients with acute encephalitis, Uttar Pradesh, India. Emerg Infect Dis 15:295–298
Vaughn DW, Hoke CH Jr (1992) The epidemiology of Japanese encephalitis: prospects for prevention. Epidemiol Rev 14:197–221
Ludwig GV, Iacono-Connors LC (1993) Insect-transmitted vertebrate viruses: flaviviridae. In Vitro Cell Dev Biol Anim 29A:296–309
Vrati S (2000) Comparison of the genome sequences and the phylogenetic analyses of the GP78 and the Vellore P20778 isolates of Japanese encephalitis virus from India. J Biosci 25:257–262
Chambers TJ, Hahn CS, Galler R et al (1990) Flavivirus genome organization, expression, and replication. Annu Rev Microbiol 44:649–688
Vashist S, Bhullar D, Vrati S (2011) La protein can simultaneously bind to both 3′- and 5′-noncoding regions of Japanese encephalitis virus genome. DNA Cell Biol 30:339–346
Pujhari SK, Prabhakar S, Ratho RK et al (2011) A novel mutation (S227T) in domain II of the envelope gene of Japanese encephalitis virus circulating in North India. Epidemiol Infect 139:849–856
Solomon T, Ni H, Beasley DW et al (2003) Origin and evolution of Japanese encephalitis virus in Southeast Asia. J Virol 77:3091–3098
Mackenzie JS, Barrett AD, Deubel V (2002) The Japanese encephalitis serological group of flaviviruses: a brief introduction to the group. Curr Top Microbiol Immunol 267:1–10
Zhang JS, Zhao QM, Guo XF et al (2011) Isolation, genetic characteristics of human genotype 1 Japanese encephalitis virus, China, 2009. PLoS ONE 6:e16418
Chen WR, Rico-Hesse R, Tesh RB (1992) A new genotype of Japanese encephalitis virus from Indonesia. Am J Trop Med Hyg 47:61–69
Uchil PD, Satchidanandam V (2001) Phylogenetic analysis of Japanese encephalitis virus: envelope gene based analysis reveals a fifth genotype, geographic clustering, and multiple introductions of the virus into the Indian subcontinent. Am J Trop Med Hyg 65:242–251
Tsai TF (1997) Factors in the changing epidemiology of Japanese encephalitis and West Nile fever. In: Saluzzo JF, Dodet B (ed) Factors in the emergence of arbovirus diseases. Elsevier, Paris, pp 179–189
Nabeshima T, Loan HT, Inoue S et al (2009) Evidence of frequent introductions of Japanese encephalitis virus from south-east Asia and continental east Asia to Japan. J Gen Virol 90:827–832
Nabeshima T, Morita K (2010) Phylogenetic analysis of the migration of Japanese encephalitis virus in Asia. Future Virol 5(3):343–354
Huang JH, Lin TH, Teng HJ, Su CL et al (2010) Molecular epidemiology of Japanese encephalitis virus, Taiwan. Emerg Infect Dis 16:876–878
Yang Y, Ye J, Yang X et al (2011) Japanese encephalitis virus infection induces changes of mRNA profile of mouse spleen and brain. Virol J 8:80
Shankar SK, Rao TV, Mruthyunjayanna BP et al (1983) Autopsy study of brains during an epidemic of Japanese encephalitis in Karnataka. Indian J Med Res 78:431–440
Liou ML, Hsu CY (1998) Japanese encephalitis virus is transported across the cerebral blood vessels by endocytosis in mouse brain. Cell Tissue Res 293:389–394
Das S, Chakraborty S, Basu A (2010) Critical role of lipid rafts in virus entry and activation of phosphoinositide 3′ kinase/Akt signaling during early stages of Japanese encephalitis virus infection in neural stem/progenitor cells. J Neurochem 115:537–549
Desai A, Ravi V, Chandramuki A et al (1995) Proliferative response of human peripheral blood mononuclear cells to Japanese encephalitis virus. Microbiol Immunol 39:269–273
Desai A, Shankar SK, Jayakumar PN et al (1997) Co-existence of cerebral cysticercosis with Japanese encephalitis: a prognostic modulator. Epidemiol Infect 118:165–171
Ravi V, Parida S, Desai A, Chandramuki A et al (1997) Correlation of tumor necrosis factor levels in the serum and cerebrospinal fluid with clinical outcome in Japanese encephalitis patients. J Med Virol 51:132–136
Gajanana A, Rajendran R, Thenmozhi V et al (1995) Comparative evaluation of bioassay and ELISA for detection of Japanese encephalitis virus in field collected mosquitos. Southeast Asian J Trop Med Public Health 26:91–97
Mahanta J, Boruah U, Sarmabordoloi JN et al (1996) Japanese encephalitis virus antibody among normal individuals of Dibrugarh area, upper Assam. J Commun Dis 28:181–184
Kuwayama M, Ito M, Takao S et al (2005) Japanese encephalitis virus in meningitis patients, Japan. Emerg Infect Dis 11:471–473
Chatterjee AK, Banerjee K (1975) Epidemiological studies on the encephalitis epidemic in Bankura. Indian J Med Res 63:1164–1179
Ayukawa R, Fujimoto H, Ayabe M et al (2004) An unexpected outbreak of Japanese encephalitis in the Chugoku district of Japan, 2002. Jpn J Infect Dis 57:63–66
Wang LH, Fu SH, Wang HY et al (2007) Japanese encephalitis outbreak, Yuncheng, China, 2006. Emerg Infect Dis 13:1123–1125
Burke DS, Lorsomrudee W, Leake CJ et al (1985) Fatal outcome in Japanese encephalitis. Am J Trop Med Hyg 34:1203–1210
Kumar R, Mathur A, Singh KB et al (1993) Clinical sequelae of Japanese encephalitis in children. Indian J Med Res 97:9–13
Pradhan S, Pandey N, Sashank S et al (1999) Parkinsonism due to predominant involvement of substantia nigra in Japanese encephalitis. Neurology 53:1781–1786
Gourie Devi M (1984) Clinical aspects and experience in the management of Japanese encephalitis patients. In: Proceedings of the national conference of Japanese encephalitis, ICMR, New Delhi, pp 25–29
Misra UK, Kalita J (1997) Movement disorders in Japanese encephalitis. J Neurol 244:299–303
Mathur A, Arora KL, Chaturvedi UC (1982) Transplacental Japanese encephalitis virus (JEV) infection in mice during consecutive pregnancies. J Gen Virol 59:213–217
Burke DS, Nisalak A, Ussery MA et al (1985) Kinetics of IgM and IgG responses to Japanese encephalitis virus in human serum and cerebrospinal fluid. J Infect Dis 151:1093–1099
Mathur A, Arora KL, Chaturvedi UC (1983) Host defence mechanisms against Japanese encephalitis virus infection in mice. J Gen Virol 64:805–811
Mathur A, Arora KL, Rawat S et al (1986) Persistence, latency and reactivation of Japanese encephalitis virus infection in mice. J Gen Virol 67:381–385
Ravi V, Desai AS, Shenoy PK et al (1993) Persistence of Japanese encephalitis virus in the human nervous system. J Med Virol 40:326–329
Sharma S, Mathur A, Prakash V et al (1991) Japanese encephalitis virus latency in peripheral blood lymphocytes and recurrence of infection in children. Clin Exp Immunol 85:85–89
Bharadwaj M, Khanna N, Mathur A et al (1991) Effect of macrophage-derived factor on hypoferraemia induced by Japanese encephalitis virus in mice. Clin Exp Immunol 83:215–218
Mathur A, Bharadwaj M, Chaturvedi UC (1990) Alterations in iron levels in Japanese encephalitis virus infection. Int J Exp Pathol 71:307–312
Johnson RT, Burke DS, Elwell M et al (1985) Japanese encephalitis: immunocytochemical studies of viral antigen and inflammatory cells in fatal cases. Ann Neurol 18:567–573
Khanna N, Mathur A, Chaturvedi UC (1994) Regulation of vascular permeability by macrophage-derived chemotactic factor produced in Japanese encephalitis. Immunol Cell Biol 72:200–204
Khanna N, Agnihotri M, Mathur A et al (1991) Neutrophil chemotactic factor produced by Japanese encephalitis virus stimulated macrophages. Clin Exp Immunol 86:299–303
Khanna N, Mathur A, Bharadwaj M et al (1997) Induction of hypoglycemia in Japanese encephalitis virus infection: the role of T lymphocytes. Clin Exp Immunol 107:282–287
Tandon A, Singh A, Mathur A et al (2002) Hypoglycemia during Japanese encephalitis virus infection in man. Int J Exp Pathol 83:39–43
Srivastava S, Khanna N, Saxena SK et al (1999) Degradation of Japanese encephalitis virus by neutrophils. Int J Exp Pathol 79:17–24
Saxena SK, Mathur A, Srivastava RC (2001) Induction of nitric oxide synthase during Japanese encephalitis virus infection: evidence of protective role. Arch Biochem Biophys 391:1–7
Singh A, Kulshreshtha R, Mathur A (2000) Secretion of the chemokine interleukin-8 during Japanese encephalitis virus infection. J Med Microbiol 49:607–612
Gupta N, Lomash V, Rao PV (2010) Expression profile of Japanese encephalitis virus induced neuroinflammation and its implication in disease severity. J Clin Virol 49:4–10
Misra UK, Srivastava R, Kalita J et al (2010) Sequential changes in serum cytokines and chemokines in a rat model of Japanese encephalitis. Neuroimmunomodulation 17:411–416
Gupta N, Bhaskar AS, Lakshmana Rao PV (2011) Transcriptional regulation and activation of the mitogen-activated protein kinase pathway after Japanese encephalitis virus infection in neuroblastoma cells. FEMS Immunol Med Microbiol 62:110–121
Kumar R, Tripathi P, Singh S, Bannerji G (2006) Clinical features in children hospitalized during the 2005 epidemic of Japanese encephalitis in Uttar Pradesh, India. Clin Infect Dis 43:123–131
Kalita J, Misra UK (1998) EEG in Japanese encephalitis: a clinico-radiological correlation. Electroencephalogr Clin Neurophysiol 106:238–243
Misra UK, Kalita J, Phadke RV, Wadwekar V et al (2010) Usefulness of various MRI sequences in the diagnosis of viral encephalitis. Acta Trop 116:206–211
Mathur A, Kumar R, Sharma S et al (1990) Rapid diagnosis of Japanese encephalitis by immunofluorescent examination of cerebrospinal fluid. Indian J Med Res 91:1–4
Ravi V, Premkumar S, Chandramuki A et al (1989) A reverse passive haemagglutination test for detection of Japanese encephalitis virus antigens in cerebrospinal fluid. J Virol Methods 23:291–298
Robinson JS, Featherstone D, Vasanthapuram R et al (2010) Evaluation of three commercially available Japanese encephalitis virus IgM enzyme-linked immunosorbent assays. Am J Trop Med Hyg 83:1146–1155
Lewthwaite P, Shankar MV, Tio PH et al (2010) Evaluation of two commercially available ELISAs for the diagnosis of Japanese encephalitis applied to field samples. Trop Med Int Health 15:811–818
Gould EA, Solomon T, Mackenzie JS (2008) Does antiviral therapy have a role in the control of Japanese encephalitis? Antiviral Res 78:140–149
Swarup V, Ghosh J, Ghosh S, Saxena A et al (2007) Antiviral and anti-inflammatory effects of rosmarinic acid in an experimental murine model of Japanese encephalitis. Antimicrob Agents Chemother 51:3367–3370
Saxena SK, Mathur A, Srivastava RC (2003) Inhibition of Japanese encephalitis virus infection by diethyldithiocarbamate is independent of its antioxidant potential. Antivir Chem Chemother 14:91–98
Nazmi A, Dutta K, Basu A (2010) Antiviral and neuroprotective role of octaguanidinium dendrimer-conjugated morpholino oligomers in Japanese encephalitis. PLoS Negl Trop Dis 4:e892
Sebastian L, Madhusudana SN, Ravi V et al (2011) Mycophenolic acid inhibits replication of Japanese encephalitis virus. Chemotherapy 57:56–61
Dung NM, Turtle L, Chong WK et al (2009) An evaluation of the usefulness of neuroimaging for the diagnosis of Japanese encephalitis. J Neurol 256:2052–2060
Japanese Encephalitis Fact Sheet. Centre for Disease Control and Prevention. National Centre for Emerging and Zoonotic Infectious Diseases (NCEZID). Division of Vector-Borne Diseases (DVBD). www.cdc.gov/ncidod/dvbid/jencephalitis/facts.htm
Chambers TJ, Tsai TF, Pervikov Y et al (1997) Vaccine development against dengue and Japanese encephalitis: report of a World Health Organization meeting. Vaccine 15:1494–1502
World Health Organization Third Biregional Meeting on Control of Japanese encephalitis; 2007 Apr 26–27; Ho Chi Minh City, Vietnam. Available from http://www.wpro.who.int/NR/rdonlyres/50129D1D-E9B3-4707-A62E-0A541DBC3032/0/MTGRPT_JEBireg3.pdf
Hoke CH, Nisalak A, Sangawhipa N et al (1988) Protection against Japanese encephalitis by inactivated vaccines. N Engl J Med 319:608–614
Bharati K, Vrati S (2006) Japanese encephalitis: development of new candidate vaccines. Expert Rev Anti Infect Ther 4:313–324
Plesner AM (2003) Allergic reactions to Japanese encephalitis vaccine. Immunol Allergy Clin North Am 23:665–697
Tsai TF, Chang GJ, Yu XY (1999) Japanese encephalitis vaccine. In: Plotkins SA, Orenstein OK (eds) Vaccine, vol 18. Thailand, 13–15 October, 1998, pp 1–25
Srivastava AK, Putnak JR, Lee SH et al (2001) A purified inactivated Japanese encephalitis virus vaccine made in Vero cells. Vaccine 19:4557–4565
Appaiahgari MB, Vrati S (2004) Immunogenicity and protective efficacy in mice of a formaldehyde-inactivated Indian strain of Japanese encephalitis virus grown in Vero cells. Vaccine 22:3669–3675
Tandan JB, Ohrr H, Sohn YM, Yoksan S et al (2007) Single dose of SA 14-14-2 vaccine provides long-term protection against Japanese encephalitis: a case-control study in Nepalese children 5 years after immunization. Vaccine 25:5041–5045
WHO (2006) Japanese encephalitis vaccines. Wkly Epidemiol Rec 81:331–340
Appaiahgari MB, Vrati S (2010) IMOJEV(®): a Yellow fever virus-based novel Japanese encephalitis vaccine. Expert Rev Vaccines 9:1371–1384
Beasley DW, Lewthwaite P, Solomon T (2008) Current use and development of vaccines for Japanese encephalitis. Expert Opin Biol Ther 8:95–106
Seif SA, Morita K, Igarashi A (1996) A 27 amino acid coding region of JE virus E protein expressed in E. coli as fusion protein with glutathione-S-transferase elicit neutralizing antibody in mice. Virus Res 43:91–96
Appaiahgari MB, Saini M, Rauthan M et al (2006) Immunization with recombinant adenovirus synthesizing the secretory form of Japanese encephalitis virus envelope protein protects adenovirus-exposed mice against lethal encephalitis. Microbes Infect 8:92–104
Bharati K, Rani R, Vrati S (2009) Evaluation of Japanese encephalitis virus DNA vaccine candidates in rhesus monkeys [Macaca mulatta]. Vaccine 27:10–16
Appaiahgari MB, Vrati S (2007) DNAzyme-mediated inhibition of Japanese encephalitis virus replication in mouse brain. Mol Ther 15:1593–1599
Elias C, Okwo-Bele JM, Fischer M (2009) A strategic plan for Japanese encephalitis control by 2015. Lancet Infect Dis 9:7
Caramello P, Canta F, Balbiano R et al (2007) A case of imported JE acquired during short travel in Vietnam. Are current recommendations about vaccination broader? J Travel Med 14:346–348
Zhang S, Yin Z, Suraratdecha C et al (2011) Knowledge, attitudes and practices of caregivers regarding Japanese encephalitis in Shaanxi Province, China. Public Health 125:79–83
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Singh, A., Saxena, S.K., Srivastava, A.K. et al. Japanese Encephalitis: A Persistent Threat. Proc. Natl. Acad. Sci. Sect B. Biol. Sci. 82, 55–68 (2012). https://doi.org/10.1007/s40011-011-0005-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40011-011-0005-x