
Abstract
Purpose
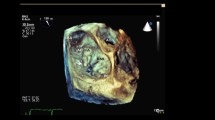
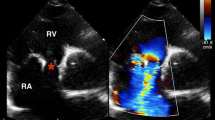
Transesophageal echocardiography is crucial for the diagnosis of infective endocarditis (IE). Use of three-dimensional transesophageal echocardiography (3D-TEE) could improve the reliability of echocardiographic findings. This study sought to determine the value of 3D-TEE in the diagnosis of IE in comparison to two-dimensional (2D)-TEE and 2D transthoracic echocardiography (2D-TTE).
Methods
In this prospective cohort study in a tertiary care university hospital 144 consecutive patients with clinically suspected IE were included. The patients were subjected to clinical, microbiological and echocardiographic evaluation (2D-TTE, 2D-TEE and 3D-TEE) and their clinical history evaluated retrospectively to establish a reference diagnosis of IE in accordance to current guideline recommendations.
Results
In 48 (33 %) patients the diagnosis of IE was established. 2D-TEE and 3D-TEE showed a sensitivity, specificity, positive and negative predictive value for diagnosis of IE of 94 % and 63, 90 and 95 %, 82 and 86 % and 97 and 83 %, respectively, with similar results in patients with native and prosthetic valves. Vegetations and abscess were detected in 43 and 5 patients with final diagnosis of IE by any of the assessed echocardiographic modalities, with only one case of vegetation detected by 3D-TEE only and not by 2D-TEE.
Conclusions
In this cohort of patients with suspected IE, 3D-TEE showed substantial lower sensitivity and negative predictive value for diagnosis of IE when compared to 2D-TEE. 3D-TEE might provide additive diagnostic information with impact on clinical decisions only in individual cases.


Similar content being viewed by others
References
Prendergast BD. The changing face of infective endocarditis. Heart. 2006;92:879–85. doi:10.1136/hrt.2005.067256.
Heiro M, Helenius H, Hurme S, et al. Long-term outcome of infective endocarditis: a study on patients surviving over one year after the initial episode treated in a Finnish teaching hospital during 25 years. BMC Infect Dis. 2008;8:49. doi:10.1186/1471-2334-8-49.
Moreillon P, Que Y-A. Infective endocarditis. Lancet. 2004;363:139–49. doi:10.1016/S0140-6736(03)15266-X.
Khanna N, Roy A, Bahl VK. Janeway lesions: an old sign revisited. Circulation. 2013;127:861. doi:10.1161/CIRCULATIONAHA.112.127787.
Li JS, Sexton DJ, Mick N, et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis. 2000;30:633–8. doi:10.1086/313753.
Habib G, Hoen B, Tornos P, et al. Guidelines on the prevention, diagnosis, and treatment of infective endocarditis (new version 2009): the task force on the prevention, diagnosis, and treatment of infective endocarditis of the European society of cardiology (ESC). Endorsed by the European. Eur Heart J. 2009;30:2369–413. doi:10.1093/eurheartj/ehp285.
Habib G, Badano L, Tribouilloy C, et al. Recommendations for the practice of echocardiography in infective endocarditis. Eur J Echocardiogr. 2010;11:202–19. doi:10.1093/ejechocard/jeq004.
Liu Y, Tsai W, Lin C. Usefulness of real-time three-dimensional echocardiography for diagnosis of infective endocarditis. Scand Cardiovasc J. 2009;43:318–23. doi:10.1080/14017430902737940.
Hansalia S, Biswas M, Dutta R, et al. The value of live/real time three-dimensional transesophageal echocardiography in the assessment of valvular vegetations. Echocardiography. 2009;26:1264–73. doi:10.1111/j.1540-8175.2009.01042.x.
Berdejo J, Shibayama K, Harada K, et al. Evaluation of vegetation size and its relationship with embolism in infective endocarditis: a real-time 3-dimensional transesophageal echocardiography study. Circ Cardiovasc Imaging. 2014;7:149–54. doi:10.1161/CIRCIMAGING.113.000938.
Kort S. Real-time 3-dimensional echocardiography for prosthetic valve endocarditis: initial experience. J Am Soc Echocardiogr. 2006;19:130–9. doi:10.1016/j.echo.2005.08.023.
Tanis W, Teske AJ, van Herwerden LA, et al. The additional value of three-dimensional transesophageal echocardiography in complex aortic prosthetic heart valve endocarditis. Echocardiography. 2014;. doi:10.1111/echo.12602.
Kenzaka T, Nishimura Y. Three-dimensional transoesophageal echocardiography for the diagnosis of prosthetic valve endocarditis. BMJ Case Rep. 2014;2014:1–2. doi:10.1136/bcr-2014-203592.
Caselli S, Mazzesi G, Tritapepe L, et al. 3D echocardiographic delineation of mitral-aortic intervalular fibrosa pseudoaneurysm caused by bicuspid aortic valve endocarditis. Echocardiography. 2011;28:E1–4. doi:10.1111/j.1540-8175.2010.01229.x.
Penugonda N, Duncan K, Afonso L. Complex endocarditis in an immunocompromised host: the role of three-dimensional echocardiography. J Am Soc Echocardiogr. 2007;20:1314.e9–11. doi:10.1016/j.echo.2007.02.033.
Walker N, Bhan A, Desai J, Monaghan MJ. Myocardial abscess: a rare complication of valvular endocarditis demonstrated by 3D contrast echocardiography. Eur J Echocardiogr. 2010;11:E37. doi:10.1093/ejechocard/jeq090.
Pothineni KR, Inamdar V, Miller AP, et al. Initial experience with live/real time three-dimensional transesophageal echocardiography. Echocardiography. 2007;24:1099–104. doi:10.1111/j.1540-8175.2007.00598.x.
Pepi M, Tamborini G, Maltagliati A, et al. Head-to-head comparison of two- and three-dimensional transthoracic and transesophageal echocardiography in the localization of mitral valve prolapse. J Am Coll Cardiol. 2006;48:2524–30. doi:10.1016/j.jacc.2006.02.079.
García-Orta R, Moreno E, Vidal M, et al. Three-dimensional versus two-dimensional transesophageal echocardiography in mitral valve repair. J Am Soc Echocardiogr. 2007;20:4–12. doi:10.1016/j.echo.2006.07.005.
Grewal J, Mankad S, Freeman WK, et al. Real-time three-dimensional transesophageal echocardiography in the intraoperative assessment of mitral valve disease. J Am Soc Echocardiogr. 2009;22:34–41. doi:10.1016/j.echo.2008.11.008.
Buck T, Breithardt OA, Fabe L, et al. Manual zur Indikation und Durchführung der Echokardiographie. Clin Res Cardiol Suppl. 2009;4:3–51. doi:10.1007/s11789-009-0051-6.
Murdoch DR, Corey GR, Hoen B, et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the international collaboration on endocarditis-prospective cohort study. Arch Intern Med. 2009;169:463–73. doi:10.1001/archinternmed.2008.603.
Habib G. Management of infective endocarditis. Heart. 2006;92:124–30. doi:10.1136/hrt.2005.063719.
Lang RM, Tsang W, Weinert L, et al. Valvular heart disease: the value of 3-dimensional echocardiography. J Am Coll Cardiol. 2011;58:1933–44. doi:10.1016/j.jacc.2011.07.035.
Anwar AM, Nosir YFM, Alasnag M, Chamsi-Pasha H. Real time three-dimensional transesophageal echocardiography: a novel approach for the assessment of prosthetic heart valves. Echocardiography. 2014;31:188–96. doi:10.1111/echo.12327.
Singh P, Manda J, Hsiung MC, et al. Live/real time three-dimensional transesophageal echocardiographic evaluation of mitral and aortic valve prosthetic paravalvular regurgitation. Echocardiography. 2009;26:980–7. doi:10.1111/j.1540-8175.2009.01022.x.
Lang RM, Badano LP, Tsang W, et al. EAE/ASE recommendations for image acquisition and display using three-dimensional echocardiography. Eur Heart J Cardiovasc Imaging. 2012;13:1–46. doi:10.1093/ehjci/jer316.
Flachskampf FA, Wouters PF, Edvardsen T, et al. Recommendations for transoesophageal echocardiography: EACVI update 2014. Eur Heart J Cardiovasc Imaging. 2014;15:353–65. doi:10.1093/ehjci/jeu015.
Sungur A, Hsiung MC, Meggo Quiroz LD, et al. The advantages of live/real time three-dimensional transesophageal echocardiography in the assessment of tricuspid valve infective endocarditis. Echocardiography. 2014;31:1293–309. doi:10.1111/echo.12785.
Ducas R, Tsang W, Chong AA, et al. Echocardiography and vascular ultrasound: new developments and future directions. Can J Cardiol. 2013;29:304–16. doi:10.1016/j.cjca.2012.11.001.
Feuchtner GM, Stolzmann P, Dichtl W, et al. Multislice computed tomography in infective endocarditis: comparison with transesophageal echocardiography and intraoperative findings. J Am Coll Cardiol. 2009;53:436–44. doi:10.1016/j.jacc.2008.01.077.
Pérez-Vázquez A, Fariñas MC, García-Palomo JD, et al. Evaluation of the Duke criteria in 93 episodes of prosthetic valve endocarditis: could sensitivity be improved? Arch Intern Med. 2000;160:1185–91.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
None.
Conflict of interest
The authors have no relevant conflicts of interest to disclose.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Roman Pfister and Yann Betton contributed equally.
Rights and permissions
About this article

Cite this article
Pfister, R., Betton, Y., Freyhaus, H.t. et al. Three-dimensional compared to two-dimensional transesophageal echocardiography for diagnosis of infective endocarditis. Infection 44, 725–731 (2016). https://doi.org/10.1007/s15010-016-0908-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-016-0908-9