
Abstract
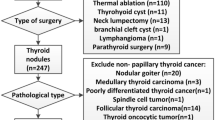
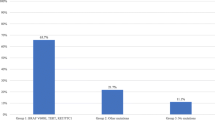
To assess the utility of mutational markers in determining the most appropriate initial surgery for patients with thyroglossal duct cyst carcinoma (TGDCCa) and a normal thyroid gland. Our sample comprised 15 patients with a diagnosis of TGDCCa and a thyroid gland histologically negative for any malignant involvement, who underwent surgery between the years 1994 and 2017. Clinical records were reviewed and tissue specimens were genetically tested for the presence of the most commonly encountered mutational markers in differentiated thyroid cancer: BRAF, N-RAS, and H-RAS. The primary outcome of interest was the correlation between mutational marker positivity and the T-stage of the primary tumor and its potential implication on therapeutic decision making. All 15 cases were papillary carcinomas with a mean tumor size of 17 mm (2–40 mm). According to the 7th edition of the American Joint Committee on Cancer TNM staging system, these represented: T1 (n = 3), T2 (n = 1), and T3 (n = 11). Cancerous invasion of the pericystic soft tissue and/or hyoid bone was considered T3. BRAFV600E was the only mutational marker identified (7 in 15 cases). All BRAFV600E-positive lesions were T3, necessitating radioactive iodine ablation (RIA) therapy, therefore, total thyroidectomy. The correlation between BRAFV600E positivity and extracystic cancerous extension was statistically significant [1.0 (7/7) vs. 0.5 (4/8); p value = 0.0035]. BRAFV600E positivity seems to be predictive of locally advanced disease mandating RIA therapy. Therefore, it could serve as a preoperative tool that predicts the need for total thyroidectomy, in addition to Sistrunk’s procedure.
Similar content being viewed by others

References
Ellis PD, Van Nostrand AW (1977) The applied anatomy of thyroglossal tract remnants. Laryngoscope 87:765–770
Choi YM, Kim TY, Song DE et al (2013) Papillary thyroid carcinoma arising from a thyroglossal duct cyst: a single institution experience. Endocr J 60:665–670
Carter Y, Yeutter N, Mazeh H (2014) Thyroglossal duct remnant carcinoma: beyond the Sistrunk procedure. Surg Oncol 23:161–166
De Napoli L, Bakkar S, Ambrosini CE et al (2016) Indeterminate single thyroid nodule: synergistic impact of mutational markers and sonographic features in triaging patients to appropriate surgery. Thyroid. 26:390–394
World Health Organization Classification of Tumors (2004) Pathology and genetics of tumors of endocrine organs. IARC Press, Lyon
Nikiforov YE, Steward DL, Robinson-Smith TM, Haugen BR, Klopper JP, Zhu Z, Fagin JA, Falciglia M, Weber K, Nikiforova MN (2009) Molecular testing for mutations in improving the fine-needle aspiration diagnosis of thyroid nodules. J Clin Endocrinol Metab 94:2092–2098
Campbell I (2007) Chi squared and Fisher-Irwin tests of two-by-two tables with small sample recommendations. Stat Med 26:3661–3675
Richardson JT (2011) The analysis of 2 × 2 contingency tables–yet again. Stat Med 30:890. https://doi.org/10.1002/sim.4116(author reply 891-2)
Altman DG, Machin D, Bryant TN, Gardner MJ (eds) (2000) Statistics with confidence, 2nd edn. BMJ Book, London
Edge S, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A (eds) (2010) AJCC cancer staging manual, 7th edn. Springer, New York
Patel SG, Escrig M, Shaha AR, Singh B, Shah JP (2002) Management of well-differentiated thyroid carcinoma within a thyroglossal duct cyst. J Surg Oncol 79:134–139
Plaza CP, Lopez ME, Carrasco CE, Meseguer LM, Perucho Ade L (2006) Management of well-differentiated thyroglossal remnant thyroid carcinoma: time to close the debate? Report of five new cases and proposal of a definitive algorithm for treatment. Ann Surg Oncol 13:745–752
Luna-Ortiz K, Hurtado-Lopez LM, Valderrama-Landaeta JL, Ruiz- Vega A (2004) Thyroglossal duct cyst with papillary carcinoma: what must be done? Thyroid 14:363–366
Miccoli P, Bakkar S (2017) Surgical management of papillary thyroid carcinoma: an overview. Updates Surg. 69:145–150. https://doi.org/10.1007/s13304-017-04495
Miccoli P, Minuto MN, Galleri D, Puccini M, Berti P (2004) Extent of surgery in thyroglossal duct carcinoma: reflections on a series of eighteen cases. Thyroid 14:121–123
Hartl DM, Al Ghuzlan A, Chami L, Leboulleux S, Schlumberger M, Travagli JP (2009) High rate of multifocality and occult lymph node metastases in papillary thyroid carcinoma arising in thyroglossal duct cysts. Ann Surg Oncol 16:2595–2601
Dzodic R, Markovic I, Stanojevic B et al (2012) Surgical management of primary thyroid carcinoma arising in thyroglossal duct cyst: an experience of a single institution in Serbia. Endocr J 59:517–522
Pellegriti G, Lumera G, Malandrino P, Latina A, Masucci R, Scollo C, Spadaro A, Sapuppo G, Regalbuto C, Pezzino V, Vigneri R (2013) Thyroid cancer in thyroglossal duct cysts requires a specific approach due to its unpredictable extension. J Clin Endocrinol Metab 98:458–465. https://doi.org/10.1210/jc.2012-1952
Bakkar S, Biricotti M, Stefanini G, Ambrosini CE, Materazzi G, Miccoli P (2016) The extent of surgery in thyroglossal cyst carcinoma. Langenbecks Arch Surg 402:799–804. https://doi.org/10.1007/s00423-016-1460-x
Capelli L, Marfisi C, Puccetti M et al (2015) Role of BRAF molecular analysis in the management of papillary thyroid carcinoma: analysis of cytological and histological samples. Cytopathology 26:297–301
Ohori NP, Wolfe J, Hodak SP et al (2013) “Colloid-rich” follicular neoplasm/suspicious for follicular neoplasm thyroid fine needle aspiration specimens: cytologic, histologic, and molecular basis for considering an alternate view. Cancer Cytopathol. 121:718–728
Yip L (2015) Molecular markers for thyroid cancer diagnosis, prognosis, and targeted therapy. J Surg Oncol 111:43–50
Macerola E, Torregrossa L et al (2017) BRAF(K601E) mutation in a follicular thyroid adenoma: a case report. Int J Surg Pathol 25:348–351. https://doi.org/10.1177/1066896916688083
Tuttle RM, Haugen B, Perrier ND (2017) Updated American Joint Committee on Cancer/Tumor-Node-Metastasis Staging System for Differentiated and Anaplastic Thyroid Cancer (Eighth Edition): what changed and why? Thyroid 27:751–756. https://doi.org/10.1089/thy.2017.0102
Rossi ED, Martini M, Straccia P et al (2014) Thyroglossal duct cancer most likely arises from a thyroid gland remnant. Virchows Arch 465:67–72
Funding
This study was not funded by any grant.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Research involving human participants and/or animals
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
For this type of study, formal consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Bakkar, S., Macerola, E., Aljarrah, Q. et al. BRAFV600E mutation: a potential predictor of more than a Sistrunk’s procedure in patients with thyroglossal duct cyst carcinoma and a normal thyroid gland. Updates Surg 71, 701–704 (2019). https://doi.org/10.1007/s13304-019-00684-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13304-019-00684-7