
Abstract
Introduction
Pandemic caused by novel coronavirus has created an unprecedented situation of lockdown in India. This retrospective study was undertaken to evaluate the impact of COVID-19 restrictions on cases of maxillofacial trauma and its etiologic variation by comparing it with the previous year archived data.
Materials and Methods
Patients with maxillofacial fracture visiting during the lockdown period (Phase) were compared to the patient’s record during the same time period in the year 2019 (Control). They were subcategorised based on the etiology of trauma, i.e., road traffic accident (RTA), self-fall, physical assault and animal attacks. Age and gender variations were also assessed. Degree of significance was calculated using t test and p value obtained.
Result
Mean age of trauma patients during lockdown and control period was 32.66 and 27.93 years, respectively. Number of cases of overall trauma had significantly decreased. Cases of RTA and self-fall were 22 and 4 in lockdown compared to 135 and 16 during control phase. Cases of physical assault increased by 50%, i.e., from 9 to 6 on comparison of both the phases. Animal attack maxillofacial injuries were 2 in each group.
Conclusion
RTA and subsequent drop in numbers of maxillofacial trauma can be shown as the benefit of lockdown nonetheless on the other side increase in number of physical assaults also shows how isolation and restrictions have psychological negative impact on society.
Similar content being viewed by others


Introduction
Disease caused by novel coronavirus strain in 2019, also called COVID-19, is the latest infectious disease that has rapidly spread worldwide. The disease started in Wuhan (China), and soon reached in the whole world. The first case of COVID-19 was reported in Kerala, India on January 30, 2020, but it was not until the mid of March 2020 that an alarming situation was anticipated [1]. Following the growing trend of virus spread a bold decision was taken by the Indian government to impose a total lockdown, which included closure of all the commercial activities and restricting the modes of transportation. Jharkhand following the guidelines of the union government enforced a firm lockdown in the state on 24th March, which continued for the next 75 days in the form of lockdown 1.0(21 days), lockdown 2.0(19 days), lockdown 3.0(14 days) and lockdown 4.0(21 days). It was gradually relaxed by means of unlock 1.0(23 days) and so on [2].
One of the norms was the restricted movement of public; even walking without a valid reason was punishable. Roads were visibly deserted and vehicular movement was scant. The infectious nature of the disease and deathly virulence of COVID-19 created fear in the mind of people and even decrease in the general non COVID-19 patients at hospital were noted. This unprecedented situation provided the opportunity to study the effect of this situation on maxillofacial trauma at our government institute which usually has a high number of cases. With the above background, the present study was undertaken to analyse the variations in the incidence, age and gender distribution of maxillomandibular trauma along with its etiological pattern during lockdown. The objectives of the study were to compare the aforementioned parameters with the recorded data of the previous year of the respective month and evaluate the possible implications in future injury prevention.
Materials and Methods
A comparative, retrospective study was performed from the archived data of maxillofacial trauma cases during the lockdown period 2020 and of the same respective months in the previous year 2019. The study was initiated after approval from the institutional research committee. All the patients who reported with maxillofacial trauma at the outpatient department of oral and maxillofacial surgery or referred from various departments of the same medical institution between March 24, 2019–30 June, 2019 and March 24, 2020–30 June, 2020 were included in the study.
The lockdown period was divided into five phases:
-
(1)
Phase A or Lockdown 1.0 (March 24, 2020–April 14, 2020)—21 days,
-
(2)
Phase B or Lockdown 2.0 (April 15, 2020–May 3, 2020)—19 days,
-
(3)
Phase C or Lockdown 3.0 (May 4, 2020–May 17, 2020)—14 days,
-
(4)
Phase D or Lockdown 4.0 (May 18, 2020–June 7, 2020)—21 days and
-
(5)
Phase E or Unlock 1.0 (June 8, 2020–June 30, 2020)—23 days.
All these phases had different levels of travel restrictions. Phase E was an easing exercise and the least restrictive one. Control Phase for comparison was taken from the archived data of March 24, 2019–June 30, 2019 and divided into five phases corresponding to phases of lockdown, namely Control A, Control B, Control C, Control D and Control E. Phase A–D was the period of strict lockdown and combinedly named a separate Phase L. Phase A to E was compiled and named phase T. Similarly control phase was named Control L and Control T, respectively.
Patients with soft tissue injuries only and those who did not require any surgical intervention were excluded from the study. Complete history of the incidence was recorded. Clinical and radiological findings with orthopantomogram and computed tomographic scan of the face were noted. All the data were tabulated in a proforma specially designed for the study. Comparative analysis was done for parameters such as number of trauma cases, gender and age. Maxillofacial trauma cases were further subcategorized as road traffic accidents, physical assault, self-fall and animal attack. Statistical analysis was done with the help of Statistical Product and Service Solutions (SPSS) version 16.01 software using Student’s t test and p value calculated. p value was considered significant at p < 0.05.
Results
A total of 59 patients of maxillofacial fractures were recorded during the study period (phase T) out of which 36 patients visited during strict lockdown 2020 (phase L) comparing to 215 patients (control T) and 158 patients (control L), respectively, during the same period of the year 2019. (Table 1).
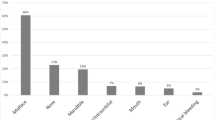
During lockdown, average age of patients was 34.42 years in Phase L and 32.66 years in phase T. Data of previous year showed mean age of 27.61 and 27.93 years, respectively. Figure 1 illustrates the variation in the mean age during all the phases A, B, C, D, E in the study and control group.

Graph showing the variation in the mean age during all the phases A, B, C, D, E in the study and control group
Analysing the etiology of the injury, road traffic accident accounted for 41 out of 59(69.49%) and 22 out of 36(61.11%) patients in lockdown phase T and strict lockdown phase L comparing to 181 out of 215(84.18%) and 135 out of 158 (85.44%) patients in the control phases (T and L), respectively. It was found to be statistically significant with p value < 0.0001. (Table 2).
Maxillofacial trauma due to physical assault was reported as 11(18.64%) and 9(25%) during phase T and phase L compared to 9(4.1%) and 6(3.79%) at control T and control L period, respectively. Although the result was not significant with p value > 0.05, 22 and 50% of patients increased compared to the data of control phase. (Table 3).
Self-fall, another cause of maxillofacial trauma was reported as 5(8.47%) and 4(11.11%) during Phase T and Phase L comparing to data of Control T and Control L which was 23(10.69%) and 16(10.12%), respectively. It was found to be statistically significant at p value < 0.05. (Table 4) The remaining two cases each in both Phase T and Control T were recorded as animal attacks corresponding to 3.38 and 0.93%, respectively.
Discussion
A pandemic of such a high magnitude is unforeseen and a dynamic phenomenon in recent history. Due to the lack of availability of universally accepted treatment or vaccination, precautionary measures like social distancing and personal hygiene are the most potent tool against this virus. Governments all over the world has struggled to deal with the situation, most of the countries had imposed lockdown for atleast few days to decelerate the spread of infection. In contrary, few countries like Sweden had followed the concept of herd immunity and focussed on social distancing and use of virus prevention tool rather than imposing travel and economic activities restriction [3]. One way or the other, COVID-19 pandemic has influenced everyday life of individual in particular and societal development in general.
In a country like India with an enormous population and deficient medical facilities, it was necessary to slow down the rate of infection spread and flatten the curve. Even before the community transfer phase of the pandemic, restriction of unprecedented magnitude was imposed in the country. Ceiling of economic activities and limiting travel without a pass or emergency resulted in decrease sale in petrochemicals and thus environmental pollution. Even the Himalayan mounting tops were visible from the distance of over 100 miles (around 160 km) with a naked eye [4, 5].
Reduction in motor vehicles and roadsters in the street resulted in a decrease in the road traffic accident and was reflected in our study. Maxillofacial fractures are consequences of any form of accident either isolated or associated with fractures of other parts of the body. In our study, we found a drastic drop in the total number of patients with maxillomandibular fracture during lockdown. Seventy three percent reduction in overall cases of trauma was observed compared to the trauma record of the previous year (Out-patients and In-patients departmental record). Although there was no significant change in male to female ratio in the study periods, the mean average age of the patients increased by 4.78 years. Explanation of this observation is due to change in etiological cause of the trauma during both the study period. Other studies suggested that in India, maxillofacial fractures due to road traffic accidents (RTA) is prominent in the age group of 20–30 years and non-RTA induced injuries are evident in people in 30 s [6].
Widen and smooth highways along with the development of superior fast bikes and cars have made accidents a blunt reality in our society. RTA is the main causative factor for the maxillo-mandibular fracture, accounting for 68–73% in India which is confirmed by various studies [7, 8]. Moreover in our study, RTA was 85.44% in the control period which significantly decreased to 61.11% of total etiology during strict lockdown(Phase L). Similar statistics were noted throughout the world. In South Africa, Morissa D (2020) [9] found the number of trauma cases reduced to 39% from 55% in 2018 and 51% in 2019 at the emergency department of an institute during the lockdown at South Africa. Nunez (2020) observed a significant reduction in the number of emergency trauma visits on comparison with the four periods for emergency trauma visits during COVID-19 pandemic, which had approximately one-fourth as many trauma admissions as any other period. Emergency trauma visits was accounted for just 7.8% of all the admissions [10]. Despite of all the problems caused by Covid-19, a decrease in the incidence of the RTA is like a silver lining in the dark sky.
Self-fall including fall from a height, slipping or injuries was the second most cause of maxillofacial trauma. Significant reduction of these patients was also noted during phase T and phase L. Restriction in outdoor activities and work-related accidents attributes to low number of self-fall injuries during the lockdown.
Apart from these restrictions, prohibition on the alcohol retail during this period was another cause for reduction of these numbers. Hingston (1993) on a review on alcohol and non-traffic untended injuries found that alcohol was present on 20–77% of the fall fatalities [11]. In another recent study by Chen CM et al. [12] (2017), it was found that increased-risk drinkers and highest-risk drinkers are more susceptible to nonfatal fall injuries than lifetime abstainers [12].
Another key finding of the present study was increased maxillofacial trauma due to physical assault, including domestic violence. The low number of patients of these categories was reported in all the phases and the comparative result between the groups was statistically insignificant. However, 50% of increase of cases with assault was reported compared to the archived data of the control period. A higher perceived risk to Covid-19 could increase anticipatory fear and anxiety. This fear, depression, loneliness and anxiety during the time of crisis not only could affect mental health but also make them aggressive and irritable. [13] It was found that 40–50% increase in domestic violence in Brazil, 25% increase in help call related to domestic violence in the UK was reported. [14] Boseruo (2020) reported 10 to 27% increase in domestic violence at different police stations in America. [15] Boredom, people staying in quarantine and isolation have proved to be ailing for their mental health. This must be resolved by proper counselling, creating social bubble between individuals and starting some sort of outdoor activities.
During unlock, phase of restriction denoted as phase E in our study, rise in the number of patients with RTA was noted. In this phase except for public transport, all the means of road transportation were started. This was even reflected in our study as 19 patients in 23 days reported in contrast to 22 patients in 75 days of lockdown periods. Nevertheless, the data suggest that it was significantly less than 46 patients in the control E period of 2019.
Economic activities, traffic and thus RTA are on the rise again but it will take some time to resume to the magnitude of the post-COVID-19 era. Tackling COVID-19 is a multidisciplinary approach. Imposing lockdown is a potent tool in the armoury of every government to slow the virus spread but policy makers must take a balance approaching tackling the situation.
Conclusion
Significant drop in maxillofacial injuries was directly related to drop in vehicular movement amid lockdown. Increase incidence of inter-personnel violence induced injuries illustrated how isolation and stagnation in life have influenced negatively towards the mental health of few individuals. Lockdown is like a pause button for the disease spread and a short-term weapon against COVID-19 but in long-term a more balanced approach in prevention and restriction should be the way forward.
References
Rawat M (2020) Coronavirus in India: Tracking country's first 50 COVID-19 cases; what numbers tell. In: Living Media India Limited. India. https://www.indiatoday.in/india/story/coronavirus-in-india-tracking-country-s-first-50-covid-19-cases-what-numbers-tell-1654468-2020-03-12. Accessed 20 Sep 2020
Singh SG (2020) Covid-19: Here's a timeline of events since lockdown was imposed in India. In: Business Standard Private Ltd. New Delhi. https://www.business-standard.com/article/current-affairs/here-s-a-timeline-of-events-since-lockdown-was-imposed-in-india-120070201413_1.html. Accessed 17 Jul 2020
Korhonen J, Granberg B (2020) Sweden backcasting, now? — strategic planning for covid-19 mitigation in a liberal democracy. Sustainability 12(10):4138
Agencies (2020) Lockdown impact: Fuel demand in India plunged to historic lows in April. In: Business Standard Private Ltd. New Delhi. https://www.business-standard.com/article/current-affairs/lockdown-impact-fuel-demand-in-india-plunged-to-historic-lows-in-april-120050900378_1. html. Accessed 17 Jul 2020
Picheta R (2020) People in India can see the Himalayas for the first time in 'decades,' as the lockdown eases air pollution. In: Cable News Network. https://edition.cnn.com/travel/article/himalayas-visible-lockdown-india-scli-intl/index.html. Accessed 17 Jul 2020
Ramdas S, Lingam PP, Sateesh S (2014) Review of maxillofacial fractures in a tertiary care centre in Puducherry, South East India. Ann Trop Med Public Health 7(2):100–104
Krishnaraj S, Chinnasamy R (2007) A 4-year retrospective study of mandibular fractures in a South Indian City. J Craniofac Surg 18(4):776–780
Barde D, Mudhol A, Madan R (2014) Prevalence and pattern of mandibular fracture in Central India. Natl J Maxillofac Surg 5(2):153–156
Morris D, Rogers M, Kissmer N, Du Preez A, Dufourq N (2020) Impact of lockdown measures implemented during the Covid-19 pandemic on the burden of trauma presentations to a regional emergency department in Kwa-Zulu Natal. Afr J Emerg Med, South Africa. https://doi.org/10.1016/j.afjem.2020.06.005
Nuñez JH, Sallent A, Lakhani K, Guerra-Farfan E, Vidal N, Ekhtiari S et al (2020) Impact of the COVID-19 pandemic on an emergency traumatology service: experience at a tertiary trauma centre in Spain. Injury 51(7):1414–1418
Hingson R, Howland J (1993) Alcohol and non-traffic unintended injuries. Addiction 88(7):877–883
Chen CM, Yoon YH (2017) Usual alcohol consumption and risks for nonfatal fall injuries in the United States: results from the 2004–2013 national health interview survey. Subst Use Misuse 52(9):1120–1132
Sharma AJ, Subramanyam MA (2020) Psychological impact of Covid-19 lockdown in India: Different strokes for different folks. In: MedRxiv. Cold Spring Harbor Laboratory. Available from; https://www.medrxiv.org/content/https://doi.org/10.1101/2020.05.25.20111716v1.full.pdf. Accessed 21 Jul 2020
Sharma A, Borah SB (2020) Covid-19 and domestic violence: an indirect path to social and economic crisis. J Fam Violence. 28:1–7. https://doi.org/10.1007/s10896-020-00188-8
Boserup B, McKenney M, Elkbuli A (2020) Alarming trends in US domestic violence during the COVID-19 pandemic. Am J Emerg Med 28:S0735-6757(20)30307–7. https://doi.org/10.1016/j.ajem.2020.04.077
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Vishal, Prakash, O., Rohit et al. Incidence of Maxillofacial Trauma Amid COVID-19: A Comparative Study. J. Maxillofac. Oral Surg. 21, 420–425 (2022). https://doi.org/10.1007/s12663-020-01484-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12663-020-01484-y