
Abstract
Background
Although anthracycline-related cardiomyopathy is a life-threatening complication during intensive treatment for hematological malignancies, clinical features and outcomes of this type of cardiomyopathy have been unclear because of limited reports in the literature.
Methods
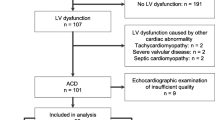
We analyzed three cases of anthracycline-related cardiomyopathy among 996 patients with either acute myelogenous leukemia (285), acute lymphoblastic leukemia (37), or malignant lymphoma (674) at our hospital during the period from 2006 to 2016.
Results
All patients showed accumulation of anthracycline within a proper range (< 500 mg/sqm). Two patients (Hodgkin lymphoma and acute lymphoblastic leukemia) showed acute heart failure (AHF) with ejection fraction (EF) of 30 and 40% after 4.5 and 5 years after diagnosis, respectively. For AHF, diuretics and carperitide were administered to control in–out balance. The remaining patient (follicular lymphoma) showed ventricular fibrillation (VF)/ventricular tachycardia (VT) with EF of 40% at 5 years after diagnosis. In this patient, immediate cardioversion made VF/VT to normal sinus rhythm, and then, amiodarone was given. Furthermore, implantable cardioverter defibrillator was set up for VF/VT. In all patients, β blocker and/or angiotensin-converting enzyme inhibitor (ACE-I) were administrated to prevent recurrence of anthracycline-related cardiomyopathy. Consequently, two of three patients showed mild improvement of cardiac function.
Conclusion
Our study indicates that late-onset (4 to 5 years) anthracycline-related cardiomyopathy can develop, though range of anthracycline accumulation is in proper range. Thus, a cautious follow-up by ECG and UCG is required. Furthermore, the early treatment after the onset of anthracycline-related cardiomyopathy should be also needed to improve the poor outcome.



Similar content being viewed by others


References
Armitage JO, Gascoyne RD, Lunning MA, et al. Non-Hodgkin lymphoma. Lancet. 2017;390:298–310.
Chatterjee K, Zhang J, Honbo N, et al. Doxorubicin cardiomyopathy. Cardiology. 2010;115:155–62.
Mazur M, Wang F, Hodge DO, et al. Burden of cardiac arrhythmias in patients with anthracycline-related cardiomyopathy. JACC Clin Electrophysiol. 2017;3:139–50.
Bernaba BN, Chan JB, Lai CK, et al. Pathology of late-onset anthracycline cardiomyopathy. Cardiovasc Pathol. 2010;19:308–11.
Slørdal L, Spigset O. Heart failure induced by non-cardiac drugs. Drug Saf. 2006;29:567–86.
Zamorano JL, Lancellotti P, Rodriguez Muñoz D, et al. ESC Scientific Document Group 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: & #x2002;The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur Heart J. 2016;37:2768–801.
Abdel-Qadir H, Amir E, Thavendiranathan P. Prevention, detection, and management of chemotherapy-related cardiac dysfunction. Can J Cardiol. 2016;32:891–9.
Piper SE, McDonagh TA. Chemotherapy-related cardiomyopathy. Eur Cardiol. 2015;10:19–24.
Plana JC, Galderisi M, Barac A, et al. Expert consensus for multimodality imaging evaluation of adult patients during and after cancer therapy: a report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2014;27:911–39.
Plana JC, Galderisi M, Barac A, et al. Expert consensus for multimodality imaging evaluation of adult patients during and after cancer therapy: a report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2014;15:1063–93.
Cardinale D, Colombo A, Bacchiani G, et al. Early detection of anthracycline cardiotoxicity and improvement with heart failure therapy. Circulation. 2015;131:1981–8.
Steinherz LJ, Steinherz PG, Tan CT, et al. Cardiac toxicity 4 to 20 years after completing anthracycline therapy. JAMA. 1991;266:1672–7.
Acknowledgements
We thank the medical and nursing staff who cared for the patients. We are grateful to Mr. Nakamae for the precious suggestions on the case.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Noriaki Kawano, Sayaka Kawano, Shuro Yoshida, Takuro Kuriyama, Taro Tochigi, Takashi Nakaike, Tomonori Shimokawa, Kiyoshi Yamashita, Hidenobu Ochiai, Kazuya Shimoda, Koichi Mashiba and Ikuo Kikuchi declare that they have no conflict of interest (COI).
Human rights statements and informed consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later revisions. Informed consent was obtained from all patients for this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kawano, N., Kawano, S., Yoshida, S. et al. Three cases of late-onset anthracycline-related cardiomyopathy due to chemotherapies for hematological malignancy. J Echocardiogr 19, 45–52 (2021). https://doi.org/10.1007/s12574-020-00484-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12574-020-00484-8