
Abstract
Introduction
Difficulties initiating and uptitrating β-blockers due to tolerability can complicate management of heart failure. Among other actions, β-blockers reduce heart rate, which is an important cardiovascular risk factor in heart failure. A new therapeutic strategy is ivabradine, which reduces resting heart rate and is associated with improved outcomes.
Methods
A 5-month, prospective, open-label, nonrandomized single-center study was performed in 69 patients. All patients had chronic heart failure with left ventricular systolic dysfunction in sinus rhythm, each were initiated on 3.125 mg twice daily (bid) carvedilol alone (n = 36) or 3.125 mg bid carvedilol/5 mg bid ivabradine (n = 33), on top of background therapy including angiotensin-converting enzyme inhibitor (88%), diuretics (86%), antiplatelet agents (91%), and statins (90%). Dosages were uptitrated every 2 weeks to 25 mg bid carvedilol in both groups and 7.5 mg bid ivabradine maximum in the carvedilol/ivabradine group. Uptitration of carvedilol lasted 1.9 ± 0.4 months with carvedilol/ivabradine and 2.8 ± 0.6 months with carvedilol alone (P < 0.05).
Results
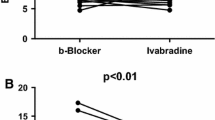
The patients receiving ivabradine had lower resting heart rate at 5 months (61.6 ± 3.1 versus 70.2 ± 4.4 bpm, P < 0.05). Adding ivabradine to carvedilol in patients with heart failure was associated with increases in the 6-min walk test and ejection fraction (all P < 0.05). Treatment tolerability was satisfactory. Patients receiving ivabradine and carvedilol had lower heart rates and better exercise capacity than those on carvedilol alone.
Conclusion
Adding ivabradine to carvedilol in patients with chronic heart failure improves the uptitration of β-blocker. The results merit further verification in a prospective double-blind study.




Similar content being viewed by others


References
Maggioni AP, Dahlstrom U, Filippatos G, et al. EURObservational Research Programme: the Heart Failure Pilot Survey (ESC-HF Pilot). Eur J Heart Fail. 2010;12(10):1076–84.
Jhund PS, Macintyre K, Simpson CR, et al. Long-term trends in first hospitalization for heart failure and subsequent survival between 1986 and 2003: a population study of 5.1 million people. Circulation. 2009;119(4):515–23.
Komajda M, Follath F, Swedberg K, et al. The EuroHeart Failure Survey programme—a survey on the quality of care among patients with heart failure in Europe. Part 2: treatment. Eur Heart J. 2003;24(5):464–74.
Komajda M, Hanon O, Hochadel M, et al. Contemporary management of octogenarians hospitalized for heart failure in Europe: Euro Heart Failure Survey II. Eur Heart J. 2009;30(4):478–86.
Dungen HD, Apostolovic S, Inkrot S, et al. Titration to target dose of bisoprolol vs. carvedilol in elderly patients with heart failure: the CIBIS-ELD trial. Eur J Heart Fail. 2011;13(6):670–80.
Franke J, Wolter JS, Meme L, et al. Optimization of pharmacotherapy in chronic heart failure: is heart rate adequately addressed? Clin Res Cardiol. 2013;102(1):23–31.
Russell SJ, Oliver M, Edmunds L, et al. Optimized beta-blocker therapy in heart failure: is there space for additional heart rate control? Br J Cardiol. 2012;19:21–3.
Bohm M, Swedberg K, Komajda M, et al. Heart rate as a risk factor in chronic heart failure (SHIFT): the association between heart rate and outcomes in a randomised placebo-controlled trial. Lancet. 2010;376(9744):886–94.
DiFrancesco D. Funny channels in the control of cardiac rhythm and mode of action of selective blockers. Pharmacol Res. 2006;53(5):399–406.
Swedberg K, Komajda M, Böhm M, et al. Ivabradine and outcomes in chronic heart failure (SHIFT): a randomised placebo-controlled trial. Lancet. 2010;376(9744):875–85.
Savelieva I, Camm AJ. I(f) inhibition with ivabradine : electrophysiological effects and safety. Drug Saf. 2008;31(2):95–107.
Joannides R, Moore N, Iacob M, et al. Comparative effects of ivabradine, a selective heart rate-lowering agent, and propranolol on systemic and cardiac haemodynamics at rest and during exercise. Br J Clin Pharmacol. 2006;61(2):127–37.
Mulder P, Barbier S, Chagraoui A, et al. Long-term heart rate reduction induced by the selective I(f) current inhibitor ivabradine improves left ventricular function and intrinsic myocardial structure in congestive heart failure. Circulation. 2004;109(13):1674–9.
De Ferrari GM, Mazzuero A, Agnesina L, et al. Favourable effects of heart rate reduction with intravenous administration of ivabradine in patients with advanced heart failure. Eur J Heart Fail. 2008;10:550–5.
Volterrani M, Cice G, Caminiti G, et al. Effect of Carvedilol, Ivabradine or their combination on exercise capacity in patients with Heart Failure (the CARVIVA HF trial). Int J Cardiol. 2011;151(2):218–24.
Reil JC, Tardif JC, Ford I, et al. Selective heart rate reduction with ivabradine unloads the left ventricle in heart failure patients. J Am Coll Cardiol. 2013;62(21):1977–85.
Ambrosy AP, Vaduganathan M, Mentz RJ, et al. Clinical profile and prognostic value of low systolic blood pressure in patients hospitalized for heart failure with reduced ejection fraction: insights from the Efficacy of Vasopressin Antagonism in Heart Failure: Outcome Study with Tolvaptan (EVEREST) trial. Am Heart J. 2013;165(2):216–25.
Banach M, Bhatia V, Feller MA, et al. Relation of baseline systolic blood pressure and long-term outcomes in ambulatory patients with chronic mild to moderate heart failure. Am J Cardiol. 2011;107(8):1208–14.
Meredith PA, Ostergren J, Anand I, et al. Clinical outcomes according to baseline blood pressure in patients with a low ejection fraction in the CHARM (Candesartan in Heart Failure: Assessment of Reduction in Mortality and Morbidity) Program. J Am Coll Cardiol. 2008;52(24):2000–7.
Raphael CE, Whinnett ZI, Davies JE, et al. Quantifying the paradoxical effect of higher systolic blood pressure on mortality in chronic heart failure. Heart. 2009;95(1):56–62.
Colin P, Ghaleh B, Monnet X, et al. Contributions of heart rate and contractility to myocardial oxygen balance during exercise. Am J Physiol Heart Circ Physiol. 2003;284(2):H676–82.
Colin P, Ghaleh B, Hittinger L, et al. Differential effects of heart rate reduction and beta-blockade on left ventricular relaxation during exercise. Am J Physiol Heart Circ Physiol. 2002;282(2):H672–9.
Steg P, Lopez-de-Sa E, Schiele F, et al. Safety of intravenous ivabradine in acute ST-segment elevation myocardial infarction patients treated with primary percutaneous coronary intervention: a randomized, placebo-controlled, double-blind, pilot study. Eur Heart J Acute Cardiovasc Care. 2013;2(3):270–9.
Amosova E, Andrejev E, Zaderey I, et al. Efficacy of ivabradine in combination with Beta-blocker versus uptitration of Beta-blocker in patients with stable angina. Cardiovasc Drugs Ther. 2011;25(6):531–7.
Zugck C, Martinka P, Stoeckl G, et al. Heart rate control in chronic systolic heart failure patients in Germany: results of a nationwide survey. Eur Heart J. 2013;34(suppl 1)P646.
Acknowledgments
Article processing charges for this paper were funded by Servier International, Suresnes, France. No funding was received for the study, which was independently conducted. All named authors meet the ICMJE criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval for the version to be published.
Conflict of interest
Andrey Bagriy has given lectures for Servier, Pfizer, Astra Zeneca, Takeda, and Sanofi. E. V. Schukina, O. V. Samoilova, O. A. Pricolota, S. I. Malovichko, A. V. Pricolota, E. A. Bagriy declare no conflicts of interest.
Compliance with ethics guidelines
All procedures followed were in accordance with the ethical standards of the responsible committee (institution and nation) and with the Helsinki Declaration of 1975, as revised in 2006 and 2008. Informed consent was obtained from all patients for being included in the study.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Bagriy, A.E., Schukina, E.V., Samoilova, O.V. et al. Addition of Ivabradine to β-Blocker Improves Exercise Capacity in Systolic Heart Failure Patients in a Prospective, Open-Label Study. Adv Ther 32, 108–119 (2015). https://doi.org/10.1007/s12325-015-0185-5
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-015-0185-5