
Abstract
Purpose
There is currently no single modality for accurate characterization of enlarged mediastinal lymph nodes into benign or malignant. Recently 18F-fluorothymidine (FLT) has been used as a proliferation marker. In this prospective study, we examined the role of 18F-fluorodeoxyglucose (18F-FDG) positron emission tomography/computed tomography (PET/CT) and 18F-FLT PET/CT in categorizing mediastinal lymph nodes as benign or malignant.
Materials and methods
A total of 70 consecutive patients with mediastinal lymphadenopathy detected on computed tomography (CT) or chest radiograph underwent whole body 18F-FLT PET/CT and 18F-FDG PET/CT (within 1 week of each other). Lymph nodal tracer uptake was determined by calculation of standardized uptake value (SUV) with both the tracers. Results of PET/CT were compared with histopathology of the lymph nodes.
Results
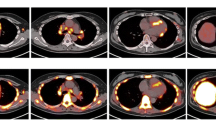
Histopathology results showed thirty-seven patients with sarcoidosis, seven patients with tuberculosis, nine patients with non-small cell lung cancer, five patients with Hodgkin’s lymphoma and twelve patients with non-Hodgkin’s lymphoma. The mean FDG SUVmax of sarcoidosis, tuberculosis, Hodgkin’s and non-Hodgkin’s lymphoma was 12.7, 13.4, 8.2, and 8.8, respectively, and the mean FLT SUVmax was 6.0, 5.4, 4.4, and 3.8, respectively. It was not possible to characterize mediastinal lymphadenopathy as benign or malignant solely based on FDG SUVmax values (p > 0.05) or FLT SUVmax values (p > 0.05). There was no significant difference in FDG uptake (p > 0.9) or FLT uptake (p > 0.9) between sarcoidosis and tuberculosis. In lung cancer patients, the FDG SUVmax and FLT SUVmax of those lymph nodes with tumor infiltration on biopsy was 6.7 and 3.9, respectively, and those without nodal infiltration was 6.4 and 3.7, respectively, and both the tracers were not able to characterize the nodal status as malignant or benign (p > 0.05).
Conclusion
Though 18F-FLT PET/CT and 18F-FDG PET/CT reflect different aspects of biology, i.e., proliferation and metabolism, respectively, neither tracer could provide satisfactory categorization of benign and malignant lymph nodes. The results of this study clearly suggest that differentiation of mediastinal nodes into benign and malignant solely based on SUVmax values cannot be relied upon, especially in settings where tuberculosis and sarcoidosis are common.






Similar content being viewed by others


Explore related subjects
Discover the latest articles and news from researchers in related subjects, suggested using machine learning.References
Goodwin RA, Shapiro JL, Thurman GH, Thurman SS, Des Prez RM. Disseminated histoplasmosis: clinical and pathologic correlations. Medicine (Baltimore). 1980;59(1):1–33.
Sagel SS. Common fungal diseases of the lungs. I. Coccidioidomycosis. Radiol Clin North Am. 1973;11(1):153–61.
Manns BJ, Baylis BW, Urbanski SJ, Gibb AP, Rabin HR. Paracoccidioidomycosis: case report and review. Clin Infect Dis. 1996;23(5):1026–32.
Petrillo R, Balzarini L, Bidoli P, Ceglia E, D’Ippolito G, Tess JD, et al. Esophageal squamous cell carcinoma: MRI evaluation of mediastinum. Gastrointest Radiol. 1990;15(4):275–8.
Zerhouni EA, Rutter C, Hamilton SR, Balfe DM, Megibow AJ, Francis IR, et al. CT and MR imaging in the staging of colorectal carcinoma: report of the Radiology Diagnostic Oncology Group II. Radiology. 1996;200(2):443–51.
Sohn KM, Lee JM, Lee SY, Ahn BY, Park SM, Kim KM. Comparing MR imaging and CT in the staging of gastric carcinoma. AJR Am J Roentgenol. 2000;174(6):1551–7.
Curtin HD, Ishwaran H, Mancuso AA, Dalley RW, Caudry DJ, McNeil BJ. Comparison of CT and MR imaging in staging of neck metastases. Radiology. 1998;207(1):123–30.
Puri SK, Fan CY, Hanna E. Significance of extracapsular lymph node metastases in patients with head and neck squamous cell carcinoma. Curr Opin Otolaryngol Head Neck Surg. 2003;11(2):119–23.
Savage C, Zwischenberger JB. Image-guided fine needle aspirate strategies for staging of lung cancer. Clin Lung Cancer. 2000;2(2):101–10 (discussion 11–12).
Milman N, Faurschou P, Munch EP, Grode G. Transbronchial lung biopsy through the fibre optic bronchoscope. Results and complications in 452 examinations. Respir Med. 1994;88(10):749–53.
Pereira W Jr, Kovnat DM, Snider GL. A prospective cooperative study of complications following flexible fiberoptic bronchoscopy. Chest. 1978;73(6):813–6.
Varela-Lema L, Fernandez-Villar A, Ruano-Ravina A. Effectiveness and safety of endobronchial ultrasound-transbronchial needle aspiration: a systematic review. Eur Respir J. 2009;33(5):1156–64.
Strauss LG. Fluorine-18 deoxyglucose and false-positive results: a major problem in the diagnostics of oncological patients. Eur J Nucl Med. 1996;23(10):1409–15.
Buck AC, Schirrmeister HH, Guhlmann CA, Diederichs CG, Shen C, Buchmann I, et al. Ki-67 immunostaining in pancreatic cancer and chronic active pancreatitis: does in vivo FDG uptake correlate with proliferative activity? J Nucl Med. 2001;42(5):721–5.
Tehrani OS, Shields AF. PET imaging of proliferation with pyrimidines. J Nucl Med. 2013;54(6):903–12.
Yamamoto Y, Nishiyama Y, Kimura N, Ishikawa S, Okuda M, Bandoh S, et al. Comparison of (18)F-FLT PET and (18)F-FDG PET for preoperative staging in non-small cell lung cancer. Eur J Nucl Med Mol Imaging. 2008;35(2):236–45.
Yang W, Zhang Y, Fu Z, Yu J, Sun X, Mu D, et al. Imaging of proliferation with 18F-FLT PET/CT versus 18F-FDG PET/CT in non-small-cell lung cancer. Eur J Nucl Med Mol Imaging. 2010;37(7):1291–9.
Tian J, Yang X, Yu L, Chen P, Xin J, Ma L, et al. A multicenter clinical trial on the diagnostic value of dual-tracer PET/CT in pulmonary lesions using 3′-deoxy-3′-18F-fluorothymidine and 18F-FDG. J Nucl Med. 2008;49(2):186–94.
Hoshikawa H, Kishino T, Mori T, Nishiyama Y, Yamamoto Y, Inamoto R, et al. Comparison of (18) F-FLT PET and (18) F-FDG PET for detection of cervical lymph node metastases in head and neck cancers. Acta Otolaryngol. 2012;132(12):1347–54.
Schaefferkoetter JD, Carlson ER, Heidel RE. Can 3′-deoxy-3′-((18)F) fluorothymidine out perform 2-deoxy-2-((18)F) fluoro-d-glucose positron emission tomography/computed tomography in the diagnosis of cervical lymphadenopathy in patients with oral/head and neck cancer? J Oral Maxillofac Surg. 2015;73(7):1420–8.
Nakajo M, Kajiya Y, Jinguji M, Nishimata N, Shimaoka S, Nihara T, et al. Diagnostic performance of (1)(8)F-fluorothymidine PET/CT for primary colorectal cancer and its lymph node metastasis: comparison with (1)(8)F-fluorodeoxyglucose PET/CT. Eur J Nucl Med Mol Imaging. 2013;40(8):1223–32.
Kumar A, Dutta R, Kannan U, Kumar R, Khilnani GC, Gupta SD. Evaluation of mediastinal lymph nodes using F-FDG PET-CT scan and its histopathologic correlation. Ann Thorac Med. 2011;6(1):11–6.
Al-Sarraf N, Aziz R, Doddakula K, Gately K, Wilson L, McGovern E, et al. Factors causing inaccurate staging of mediastinal nodal involvement in non-small cell lung cancer patients staged by positron emission tomography. Interact CardioVasc Thorac Surg. 2007;6(3):350–3.
Takamochi K, Yoshida J, Murakami K, Niho S, Ishii G, Nishimura M, et al. Pitfalls in lymph node staging with positron emission tomography in non-small cell lung cancer patients. Lung Cancer. 2005;47(2):235–42.
Carbone RG, Penna D, Baughman RP, Lower EE. Accuracy of serial PET-CT imaging in systemic sarcoidosis. J Clin Imaging Sci. 2014;4:21.
Sobic-Saranovic DP, Grozdic IT, Videnovic-Ivanov J, Vucinic-Mihailovic V, Artiko VM, Saranovic DZ, et al. Responsiveness of FDG PET/CT to treatment of patients with active chronic sarcoidosis. Clin Nucl Med. 2013;38(7):516–21.
Sobic-Saranovic D, Grozdic I, Videnovic-Ivanov J, Vucinic-Mihailovic V, Artiko V, Saranovic D, et al. The utility of 18F-FDG PET/CT for diagnosis and adjustment of therapy in patients with active chronic sarcoidosis. J Nucl Med. 2012;53(10):1543–9.
Maturu VN, Agarwal R, Aggarwal AN, Mittal BR, Bal A, Gupta N, et al. Dual-time point whole-body 18F-fluorodeoxyglucose PET/CT imaging in undiagnosed mediastinal lymphadenopathy: a prospective study of 117 patients with sarcoidosis and TB. Chest. 2014;146(6):e216–20.
Chilosi M, Menestrina F, Capelli P, Montagna L, Lestani M, Pizzolo G, et al. Immunohistochemical analysis of sarcoid granulomas. Evaluation of Ki67+ and interleukin-1+ cells. Am J Pathol. 1988;131(2):191–8.
Semenzato G, Pezzutto A, Pizzolo G, Chilosi M, Ossi E, Angi MR, et al. Immunohistological study in sarcoidosis: evaluation at different sites of disease activity. Clin Immunol Immunopathol. 1984;30(1):29–40.
Tan Y, Liang J, Liu D, Zhu F, Wang G, Ding X, et al. F-FLT PET/CT imaging in a Wister rabbit inflammation model. Exp Ther Med. 2014;8(1):69–72.
Zhao S, Kuge Y, Kohanawa M, Takahashi T, Zhao Y, Yi M, et al. Usefulness of 11C-methionine for differentiating tumors from granulomas in experimental rat models: a comparison with 18F-FDG and 18F-FLT. J Nucl Med. 2008;49(1):135–41.
Wang R, Zhu H, Chen Y, Li C, Li F, Shen Z, et al. Standardized uptake value based evaluation of lymphoma by FDG and FLT PET/CT. Hematol Oncol. 2014;32(3):126–32.
Buck AK, Bommer M, Stilgenbauer S, Juweid M, Glatting G, Schirrmeister H, et al. Molecular imaging of proliferation in malignant lymphoma. Cancer Res. 2006;66(22):11055–61.
Sharma SK, Mohan A. Sarcoidosis in India: not so rare! JIACM. 2004;5(1):12–21.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Rights and permissions
About this article

Cite this article
Rayamajhi, S.J., Mittal, B.R., Maturu, V.N. et al. 18F-FDG and 18F-FLT PET/CT imaging in the characterization of mediastinal lymph nodes. Ann Nucl Med 30, 207–216 (2016). https://doi.org/10.1007/s12149-015-1047-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-015-1047-6