
Abstract
Background
Hyponatremia is common in neurocritical care and is associated with poor outcome, but the optimal treatment is not known. We wished to test the hypothesis that for neurocritical care patients with severe hyponatremia (Na < 130 mmol/l) or hyponatremia (Na < 135 mmol/l) with depressed Glasgow Coma Scale (GCS) that conivaptan use would lead to increased serum sodium compared to usual care.
Methods
We prospectively screened 249 neurocritical care patients with hyponatremia for a prospective, randomized pilot (goal N = 20) trial. Study interventions were usual care, or usual care plus conivaptan 20 mg IV as a bolus followed by 20 mg IV over 24 h, the lower FDA-approved dose. Patients were prospectively followed for changes in serum and urine electrolytes and clinical examinations with a blinded examiner. This study is registered at www.clinicaltrials.gov (NCT00727090).
Results
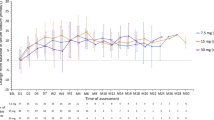
Despite the prevalence of hyponatremia, recruitment was difficult, and the study was terminated after six patients were enrolled, three in each group. Most hyponatremia in screened but non-randomized patients was transient or not associated with depressed GCS. Conivaptan led to higher serum sodium compared to usual care. The change in serum sodium from baseline, the pre-specified endpoint, was significantly different between groups at six (7.0 ± 1.7 vs. −0.6 ± 2.1 mmol/l, P = 0.008), 24 (9.7 ± 3.2 vs. 0 ± 1.0 mmol/l), and 36 h (8.0 ± 5.6 vs. −1.7 ± 2.1 mmol/l, P = 0.05). There were no apparent differences in clinical examination as a result of treatment. Adverse events were similar, and all randomized patients completed the protocol.
Conclusions
Despite an inclusive protocol, most patients were not candidates for conivaptan therapy for hyponatremia. The role of conivaptan in the Neuro-ICU remains to be defined.




Similar content being viewed by others


Explore related subjects
Discover the latest articles and news from researchers in related subjects, suggested using machine learning.References
Nathan BR. Cerebral correlates of hyponatremia. Neurocrit Care. 2007;6:72–8.
Bhardwaj A. Neurological impact of vasopressin dysregulation and hyponatremia. Ann Neurol. 2006;59:229–36.
Tisdall M, Crocker M, Watkiss J, Smith M. Disturbances of sodium in critically ill adult neurologic patients: a clinical review. J Neurosurg Anesthesiol. 2006;18:57–63.
Katayama Y, Haraoka J, Hirabayashi H, Kawamata T, Kawamoto K, Kitahara T, Kojima J, Kuroiwa T, Mori T, Moro N, Nagata I, Ogawa A, Ohno K, Seiki Y, Shiokawa Y, Teramoto A, Tominaga T, Yoshimine T. A randomized controlled trial of hydrocortisone against hyponatremia in patients with aneurysmal subarachnoid hemorrhage. Stroke. 2007;38:2373–5.
Schrier RW, Gross P, Gheorghiade M, Berl T, Verbalis JG, Czerwiec FS, Orlandi C. Tolvaptan, a selective oral vasopressin v2-receptor antagonist, for hyponatremia. N Engl J Med. 2006;355:2099–112.
Udelson JE, Smith WB, Hendrix GH, Painchaud CA, Ghazzi M, Thomas I, Ghali JK, Selaru P, Chanoine F, Pressler ML, Konstam MA. Acute hemodynamic effects of conivaptan, a dual v1a and v2 vasopressin receptor antagonist, in patients with advanced heart failure. Circulation. 2001;104:2417–23.
Wright WL, Asbury WH, Gilmore JL, Samuels OB. Conivaptan for hyponatremia in the neurocritical care unit. Neurocrit Care. 2009;11:6–13.
Murphy T, Dhar R, Diringer M. Conivaptan bolus dosing for the correction of hyponatremia in the neurointensive care unit. Neurocrit Care. 2009;11:14–9.
Laureno R, Karp BI. Myelinolysis after correction of hyponatremia. Ann Intern Med. 1997;126:57–62.
Koenig MA, Bryan M, Lewin JL III, Mirski MA, Geocadin RG, Stevens RD. Reversal of transtentorial herniation with hypertonic saline. Neurology. 2008;70:1023–9.
Acknowledgments
This study was funded by Astellas Pharma, US. The study sponsor had no role in the design of the protocol, recruitment of patients, analysis or decision to submit for publication. AMN is responsible for data integrity and the statistical analysis. AMN acknowledges past research support from NovoNordisk, the Neurocritical Care Society, and the Northwestern Memorial Foundation for an unrelated project. AMN acknowledges research support from Gaymar Inc unrelated to this study.
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article can be found at http://dx.doi.org/10.1007/s12028-011-9551-6
Rights and permissions
About this article
Cite this article
Naidech, A.M., Paparello, J., Leibling, S.M. et al. Use of Conivaptan (Vaprisol) for Hyponatremic Neuro-ICU Patients. Neurocrit Care 13, 57–61 (2010). https://doi.org/10.1007/s12028-010-9379-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-010-9379-5