
Abstract
Introduction
No proven treatments exist for intracerebral hemorrhage (ICH). Carefully selected patients may benefit from surgery, and an international multicenter trial is ongoing. We sought to determine how many patients in a population-based ICH cohort would have been eligible for surgery using the Surgical Trial in Intracerebral Hemorrhage II (STICH II) criteria.
Methods
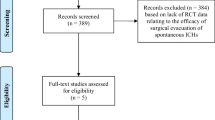
We identified all patients aged ≥18 years residing in the five-county Greater Cincinnati region who were hospitalized with first-ever nontraumatic ICH in 2005. STICH II trial criteria were used to determine eligibility for treatment and reasons for exclusion.
Results
During 2005, 286 ICH patients were identified (103 lobar, 126 deep cerebral, 23 brainstem, 28 cerebellar, and 6 IVH). Non-lobar hemorrhages are not eligible for STICH II. Among patients with lobar hemorrhage, 22 had no exclusions. The most common (not mutually exclusive) reasons for exclusion were volume <10 cc or >100 cc (n = 46) and presence of IVH (n = 27). No significant age, gender or racial differences existed between eligible and ineligible patients with lobar ICH. Only one (4.5%) of the 22 STICH II eligible patients in our population had surgery, compared with eight of 81 (9.9%) ineligible lobar ICH patients (P = 0.43). Mortality at 180 days in STICH II eligible patients was 36% vs. 49% for ineligible lobar ICH patients (P = 0.19).
Conclusions
In this population-based ICH cohort, 7.7% (22 of 286) of ICH patients would have qualified for STICH II enrollment. Other treatment options need to be explored for most ICH patients.

Similar content being viewed by others

References
Kissela B, Schneider A, Kleindorfer D, et al. Stroke in a biracial population: the excess burden of stroke among blacks. Stroke 2004;35:426–31.
Broderick J, Connolly S, Feldmann E, et al. Guidelines for the management of spontaneous intracerebral hemorrhage in adults: 2007 update: a guideline from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group. Stroke 2007;38:2001–23.
Xi G, Keep RF, Hoff JT. Mechanisms of brain injury after intracerebral haemorrhage. Lancet Neurol 2006;5:53–63.
Broderick J, Brott T, Tomsick T, Tew J, Duldner J, Huster G. Management of intracerebral hemorrhage in a large metropolitan population. Neurosurgery 1994;34:882–7.
Morgenstern LB, Frankowski RF, Shedden P, Pasteur W, Grotta JC. Surgical treatment for intracerebral hemorrhage (STICH): a single-center, randomized clinical trial. Neurology 1998;51:1359–63.
Zuccarello M, Brott T, Derex L, et al. Early surgical treatment for supratentorial intracerebral hemorrhage: a randomized feasibility study. Stroke 1999;30:1833–9.
Mendelow AD, Gregson BA, Fernandes HM. Early surgery versus initial conservative treatment in patients with spontaneous supratentorial intracerebral haematomas in the International Surgical Trial in Intracerebral Haemorrhage (STICH): a randomised trial. Lancet 2005;365:387–97.
Flaherty ML, Woo D, Haverbusch M, et al. Racial variations in location and risk of intracerebral hemorrhage. Stroke 2005;36:934–7.
Kothari RU, Brott TG, Broderick JP, et al. The abcs of measuring intracerebral hemorrhage volume. Stroke 1996;27:1304–5.
Rankin L. Cerebral vascular accidents in patients over the age of 60. II. Prognosis. Scott Med J 1957;2:200–15.
Mayer SA, Brun NC, Begtrup K, et al. Recombinant activated factor VII for acute intracerebral hemorrhage. N Engl J Med 2005;352:777–85.
Recombinant Factor VIIa in Acute Cerebral Hemorrhage (FAST) Trial results presented at the American Academy of Neurology Annual Meeting, Boston, MA 2007.
Goldstein JN, Fazen LE, Snider R, et al. Contrast extravasation on CT angiography predicts hematoma expansion in intracerebral hemorrhage. Neurology 2007;68:889–94.
Wada R, Aviv RI, Fox AJ, et al. CT angiography “spot sign” predicts hematoma expansion in acute intracerebral hemorrhage. Stroke 2007;38:1257–62.
Hattori N, Katayama Y, Maya Y, Gatherer A. Impact of stereotactic hematoma evacuation on activities of daily living during the chronic period following spontaneous putaminal hemorrhage: a randomized study. J Neurosurg 2004;101:417–20.
Marquardt G, Wolff R, Sager A, Janzen RW, Seifert V. Subacute stereotactic aspiration of haematomas within the basal ganglia reduces occurrence of complications in the course of haemorrhagic stroke in non-comatose patients. Cerebrovasc Dis 2003;15:252–7.
Flaherty ML, Kissela B, Woo D, et al. The increasing incidence of anticoagulant-associated intracerebral hemorrhage. Neurology 2007;68:116–21.
http://www.census.gov/population/censusdata. United States Bureau of the Census. Urban and Rural Population.
Acknowledgements
Supported in part by NINDS (R-01-NS 36695) and a University of Cincinnati College of Medicine Medical Student Summer Research Fellowship.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Adeoye, O., Woo, D., Haverbusch, M. et al. Eligibility for the Surgical Trial in Intracerebral Hemorrhage II Study in a Population-based Cohort. Neurocrit Care 9, 237–241 (2008). https://doi.org/10.1007/s12028-007-9045-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-007-9045-8