
Abstract
Introduction
Nodular goiter is the most common disorder of the thyroid gland. Less than total thyroidectomy procedures are considered the gold standard in the surgical management of nodular thyroid disease despite its propensity for recurrence. The aim of the study was to assess long-term sequelae of the less than total thyroidectomy procedures.
Material and methods
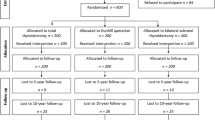
In this single-center retrospective study, records of 154 patients that underwent less than total thyroidectomy, for nodular disease and/or hyperthyroidism between 1998 and 2013, were reviewed. Patients with malignant findings in the histology report and a follow-up of less than 5 years were excluded.
Results
The mean age of the recorded patients was 65.1 ± 12.91 years of which 132 were females. Subtotal thyroidectomy was performed in 45.5% of the study population, 22.1% underwent partial thyroidectomy, while the remaining 32.5% underwent lobectomy. Long-term thyroxine supplementation was administered in 138 patients (89.6%). Recurrence of clinically important nodules (>1 cm) was observed in 68.2% of patients but only 11% of the population underwent completion thyroidectomy. In the univariate analysis, the duration of follow-up (p = 0.00005, C.I.: 0.903–0.965) as well as the type of operation (p = 0.035, C.I.: 1.031–2.348) appeared to have a significant correlation with nodular recurrence. The multivariate analysis identified the duration of follow-up (p = 0.0005, C.I.: 0.908–0.973) as the only significant predictive factor of nodular recurrence.
Conclusion
This is the first study with such a long duration of post-operative follow-up. The high rate of nodular recurrence in less than total thyroidectomy procedures along with the lifelong need for thyroxine supplementation suggest that a more conservative surgical approach is needed. When surgery is recommended, we suggest total thyroidectomy as the treatment of choice to avoid the recurrence of disease, the high cost associated with frequent follow-ups by means of sonography as well as thyroxine replacement therapy.
Similar content being viewed by others

References
J.P. Zevallos, C.M. Hartman, J.R. Kramer et al. Increased thyroid cancer incidence corresponds to increased use of thyroid ultrasound and fine-needle aspiration: a study of the Veterans Affairs health care system. Cancer 121, 741–746 (2015)
P. Perros, K. Boelaert, S. Colley et al. Guidelines for the management of thyroid cancer. Clin. Endocrinol. 81(Suppl 1), 1–122 (2014)
T. Karatzas, G. Charitoudis, D. Vasileiadis et al. Surgical treatment for dominant malignant nodules of the isthmus of the thyroid gland: a case control study. Int. J. Surg. 18, 64–68 (2015)
R. Cirocchi, S. Trastulli, J. Randolph et al. Total or near-total thyroidectomy versus subtotal thyroidectomy for multinodular non-toxic goitre in adults. Cochrane Database Syst. Rev. (2015). https://doi.org/10.1002/14651858.CD010370
M. Lytrivi, A. Kyrilli, A. Burniat et al. Thyroid lobectomy is an effective option for unilateral benign nodular disease. Clin. Endocrinol. 85(4), 602–608 (2016). https://doi.org/10.1111/cen.13088
G. Agarwal, V. Aggarwal, Is total thyroidectomy the surgical procedure of choice for benign multinodular goiter? An evidence-based review. World J. Surg. 32, 1313–1324 (2008)
H. Gharib, E. Papini, J.R. Garber et al. American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologi, Medical Guidelines for clinical practice for the diagnosis and management of thyroid nodules—2016 UPDATE. Endocr. Pract. 22, 622–639 (2016)
B.R. Haugen, E.K. Alexander, K.C. Bible et al. American Thyroid Association Management Guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines Task Force on thyroid nodules and differentiated thyroid cancer. Thyroid 26, 1–133 (2015)
R.M. Tuttle, J.A. Fagin, G. Minkowitz et al. Natural history and tumor volume kinetics of papillary thyroid cancers during active surveillance, JAMA Otolaryngol. Head Neck Surg. (2017). https://doi.org/10.1001/jamaoto.2017.1442
J. Moalem, I. Suh, Q.Y. Duh, Treatment and prevention of recurrence of multinodular goiter: an evidence-based review of the literature. World J. Surg. 32, 1301–1312 (2008)
C. Meltzer, M. Klau, D. Gurushanthaiah, J. Tsai et al. Surgeon volume in thyroid surgery: surgical efficiency, outcomes, and utilization. Laryngoscope 126(11), 2630–2639 (2016). https://doi.org/10.1002/lary.26119
G.C. Gourin, P.R. Tufano et al. Volume-based trends in thyroid surgery. Arch. Otolaryngol. Head Neck Surg. 136(12), 1191–1198 (2010). https://doi.org/10.1001/archoto.2010.212
J.C. Hardman, J.A. Smith, P. Nankivell, N. Sharma, J.C. Watkinson, Re-operative thyroid surgery: a 20-year prospective cohort study at a tertiary referral centre. Eur. Arch. Otorhinolaryngol. 272(6), 15h03–18h03 (2015). https://doi.org/10.1007/s00405-014-3068-5
S.J. Stoll, S.C. Pitt, J. Liu et al. Thyroid hormone replacement after thyroid lobectomy. Surgery 146(4), 554–558 (2009). https://doi.org/10.1016/j.surg.2009.06.026
D.Y. Lee, J. Seok, W.J. Jeong, S.H. Ahn, Prediction of thyroid hormone supplementation after thyroid lobectomy. J. Surg. Res 193(1), 273–278 (2014). https://doi.org/10.1016/j.jss.2014.07.003
L. Sandonato, G. Graceffa, C. Cipolla et al. Benign diseases of the thyroid: indications for surgical treatment and the current role of total thyroidectomy. Chir. Ital. 55, 179–187 (2003)
M. Barczynski, A. Konturek, F. Gołkowski et al. Five-year follow-up of a randomized clinical trial of unilateral thyroid lobectomy with or without postoperative levothyroxine treatment. World J. Surg. 34, 1232–1238 (2010)
P.S. Bauer, S. Murray, N. Clark et al. Unilateral thyroidectomy for the treatment of benign multinodular goiter. J. Surg. Res. 184, 514–518 (2013)
R. Bellantone, C.P. Lombardi, M. Boscherini et al. Predictive factors for recurrence after thyroid lobectomy for unilateral non-toxic goiter in an endemic area: results of a multivariate analysis. Surgery 136, 1247–1251 (2004)
Z. Ergul, M. Akinci, H. Kulacoglu, Hemithyroidectomy for unilateral thyroid disease. Chirurgia 109, 613–619 (2014)
M. Marchesi, M. Biffoni, C. Faloci et al. High rate of recurrence after lobectomy for solitary thyroid nodule. Eur. J. Surg. 168, 397–400 (2002)
H. Niepomniszcze, A. Garcia, E. Faure et al. Long-term follow-up of contralateral lobe in patients hemithyroidectomized for solitary follicular adenoma. Clin. Endocrinol. 55, 509–513 (2001)
S.E. Olson, J. Starling, H. Chen, Symptomatic benign multinodular goiter: unilateral or bilateral thyroidectomy? Surgery 142, 458–461 (2007)
R. Phitayakorn, D. Narendra, S. Bell et al. What constitutes adequate surgical therapy for benign nodular goiter? J. Surg. Res. 154, 51–55 (2009)
C. Wadstrom, J. Zedenius, A. Guinea et al. Multinodular goitre presenting as a clinical single nodule: how effective is hemithyroidectomy? Aust. N. Z. J. Surg. 69, 34–36 (1999)
G. Yetkin, M. Uludag, O. Onceken et al. Does unilateral lobectomy suffice to manage unilateral nontoxic goiter? Endocr. Pract. 16, 36–41 (2010)
J.R. Sorensen, T. Watt et al. Quality of life after thyroidectomy inpatients with nontoxic nodular goiter: a prospective cohort study. Head Neck 39, 2232–2240 (2017)
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Boutzios, G., Tsourouflis, G., Garoufalia, Z. et al. Long-term sequelae of the less than total thyroidectomy procedures for benign thyroid nodular disease. Endocrine 63, 247–251 (2019). https://doi.org/10.1007/s12020-018-1778-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12020-018-1778-y