
Abstract
Objective
The study investigated the use of great curvature plication with duodenal–jejunal bypass (GCP-DJB) in a type 2 diabetic with obesity rat model.
Methods
Twenty-two Sprague-Dawley rats were given a high fat and sugar diet with subsequent intraperitoneal injection of a small dosage of streptozotocin (30 mg/kg) and randomly assigned to either GCP-DJB (n = 12) or Sham surgery (n = 10). Body weight, peripheral blood glucose, and fasting serum insulin were assayed, and insulin resistance index (IRI) was calculated, before and at 1, 2, 4, and 8 weeks after surgery.
Results
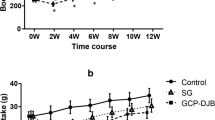
No differences were found in the preoperative characteristics of the two groups (P > 0.05). At week 1, the body weights decreased significantly, but there was no significant difference between the two groups (P > 0.05).The fasting blood glucose was significantly lower in the GCP-DJB than in the Sham group (P < 0.05), serum insulin levels were higher (P < 0.05), and IRI began to decline (P < 0.05). From 2 to 8 weeks, the body weight of Sham group gradually recovered and continued to rise, while the GCP-DJB group remained at a relatively lower state. Compared to the Sham group, the body weight, fasting blood glucose as well as IRI of GCP-DJB rats had significantly decreased (P < 0.05). But, the fasting insulin concentrations had significantly increased (P < 0.05).
Conclusion
This novel GCP-DJB procedure established a stable animal model for the study of metabolic surgery to treat type 2 diabetes mellitus (T2DM).






Similar content being viewed by others


References
Organization W H. Global report on diabetes. Working Papers, 2016.
Rubino F, Nathan DM, Eckel RH, et al. Metabolic surgery in the treatment algorithm for type 2 diabetes: a joint statement by international diabetes organizations. Diabetes Care. 2016;39(6):861–77. https://doi.org/10.2337/dc16-0236.
Angrisani L, Santonicola A, Iovino P, et al. Bariatric surgery and endoluminal procedures: IFSO worldwide survey 2014. Obes Surg. 2017;27(9):2290–2. https://doi.org/10.1007/s11695-017-2773-8.
Angrisani L, Santonicola A, Iovino P, et al. Bariatric surgery worldwide 2013. Obes Surg. 2015;25(10):1822–32. https://doi.org/10.1007/s11695-015-1657-z.
Mahawar KK, Kumar P, Carr WR, et al. Current status of mini-gastric bypass. J Minim Access Surg. 2016;12(4):305–10. https://doi.org/10.4103/0972-9941.181352.
Sánchez-Pernaute A, Rubio MÁ, Cabrerizo L, et al. Single-anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S) for obese diabetic patients. Surg Obes Relat Dis. 2015;11(5):1092–8. https://doi.org/10.1016/j.soard.2015.01.024.
Skrekas G, Antiochos K, Stafyla VK. Laparoscopic gastric greater curvature plication: results and complications in a series of 135 patients. Obes Surg. 2011;21(11):1657–63. https://doi.org/10.1007/s11695-011-0499-6.
Nguyen NT, Varela JE. Bariatric surgery for obesity and metabolic disorders: state of the art. Nat Rev Gastroenterol Hepatol. 2016;14(3):160–9. https://doi.org/10.1038/nrgastro.2016.170.
Concors SJ, Ecker BL, Maduka R, et al. Complications and surveillance after bariatric surgery. Curr Treat Options Neurol. 2016;18(1):5. https://doi.org/10.1007/s11940-015-0383-0.
Ponce J, Nguyen NT, Hutter M, et al. American Society for Metabolic and Bariatric Surgery estimation of bariatric surgery procedures in the United States, 2011-2014. Surg Obes Relat Dis. 2015;11(6):1199–200. https://doi.org/10.1016/j.soard.2015.08.496.
Himpens J, Cadière GB, Bazi M, et al. Long-term outcomes of laparoscopic adjustable gastric banding. Arch Surg. 2011;146(7):802–7. https://doi.org/10.1001/archsurg.2011.45.
Kindel T, Martin E, Hungness E, et al. High failure rate of the laparoscopic-adjustable gastric band as a primary bariatric procedure. Surg Obes Relat Dis. 2014;10(6):1070–5. https://doi.org/10.1016/j.soard.2013.11.014.
Altieri MS, Yang J, Telem DA, et al. Lap band outcomes from 19,221 patients across centers and over a decade within the state of New York. Surg Endosc. 2016;30(5):1725–32. https://doi.org/10.1007/s00464-015-4402-8.
Fusco PEB, Poggetti RS, Younes RN, et al. Evaluation of gastric greater curvature invagination for weight loss in rats. Obes Surg. 2006;16(2):172–7. https://doi.org/10.1381/096089206775565203.
Talebpour M, Motamedi SM, Talebpour A, et al. Twelve year experience of laparoscopic gastric plication in morbid obesity: development of the technique and patient outcomes. Ann Surg Innov Res. 2012;6(1):1–16.
Wang YD, Ye ZY, Zhu YW, et al. Clinical application of laparoscopic greater curvature plication. Zhejiang Med. 2011;33(3):358–9. (In Chinese)
Tang Y, Tang S, Comparative Efficacy HS. Safety of laparoscopic greater curvature plication and laparoscopic sleeve gastrectomy: a meta-analysis. Obes Surg. 2015;25(11):1–7.
Ahluwalia JS, Kuo HC, Chang PC, et al. Standardized technique of laparoscopic adjustable gastric banded plication with 4-year results. Obes Surg. 2015;25(9):1756–7. https://doi.org/10.1007/s11695-015-1756-x.
Cohen RV, Rubino F, Schiavon C, et al. Diabetes remission without weight loss after duodenal bypass surgery. Surg Obes Relat Dis. 2012;8(5):e66–8. https://doi.org/10.1016/j.soard.2011.07.007.
Steinert RE, Feinlebisset C, Asarian L, et al. Ghrelin, CCK, GLP-1, and PYY(3-36): secretory controls and physiological roles in eating and glycemia in health, obesity, and after RYGB. Physiol Rev. 2017;97(1):411–63. https://doi.org/10.1152/physrev.00031.2014.
Tack J, Arts J, Caenepeel P, et al. Pathophysiology, diagnosis and management of postoperative dumping syndrome. Nat Rev Gastroenterol Hepatol. 2009;6(10):583–90. https://doi.org/10.1038/nrgastro.2009.148.
Mui WL, Lee DW, Lam KK, et al. Laparoscopic greater curve plication in Asia: initial experience. Obes Surg. 2013;23(2):179–83. https://doi.org/10.1007/s11695-012-0761-6.
Shen D, Ye H, Wang Y, et al. Laparoscopic greater curvature plication: surgical techniques and early outcomes of a Chinese experience. Surg Obes Relat Dis. 2014;10(3):432–7. https://doi.org/10.1016/j.soard.2013.09.004.
Sang KL, Heo Y, Park JM, et al. Roux-en-Y gastric bypass vs. sleeve gastrectomy vs. gastric banding: the first multicenter retrospective comparative cohort study in obese Korean patients. Yonsei Med J. 2016;57(4):956–62.
Chiappetta S, Stier C, Scheffel O, et al. The first case report of failed single-anastomosis-duodeno-ileal bypass converted to one anastomosis gastric bypass/mini-gastric bypass. Int J Surg Case Rep. 2017;35(C):68–72. https://doi.org/10.1016/j.ijscr.2017.04.020.
Vilallonga R, Balibrea JM, Curell A, et al. Technical options for malabsorption issues after single anastomosis duodenoileal bypass with sleeve gastrectomy. Obes Surg. 2017:1–5.
Acknowledgements
This work was supported by grants from the NSFC (Natural Science Foundation of China) No. 81300723, No.81270969, and No.81370984. Nian-Cun Qiu, Xiao-Xia Cen, and Miao-E Liu had the original conception, carried out the experimental work, and wrote the article. They contributed equally to this work and should be considered as co-first authors. Si-Luo Zha and Ling-Di Wang participated in the data analysis and interpretation. Cheng-Xiang Shan and Wei Zhang participated in data collection and coordination of experimental work. Qing Liu, Yang Wang, and Ming Qiu were involved in the revision of the article. Yang Wang and Ming Qiu were the corresponding authors. All authors had read and approved the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Informed Consent
Informed consent was obtained from individual participants included in the study.
Animal Rights Statement and Ethical Approval
This study was approved by the Animal Ethics Committee of Changzheng Hospital Affiliated to the Secondary Military Medical University. For this type of study, formal consent is not required.
Conflict of Interest
The authors declare that they have no conflict of interest.
Electronic supplementary material
Fig. A
Dissociate the great curvature of stomach (JPEG 6904 kb)
Fig. B
Dissociate the surrounding area of duodenum and pylorus (JPEG 6444 kb)
Fig. C
The unfolded great curvature (JPEG 3692 kb)
Fig. D
First-layer plication (JPEG 4377 kb)
Fig. E
Second-layer plication (JPEG 382 kb)
Fig. F
Disconnect the duodenum and ligate the stump (JPEG 5006 kb)
Fig. G
End-to-side anastomosis (JPEG 4145 kb)
Fig. H
Duodenum–jejunostomy (JPEG 6127 kb)
Rights and permissions
About this article

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cite this article
Qiu, NC., Cen, XX., Liu, ME. et al. Greater Curvature Plication with Duodenal–Jejunal Bypass: a Novel Metabolic Surgery for Type 2 Diabetes Mellitus. OBES SURG 28, 1595–1601 (2018). https://doi.org/10.1007/s11695-017-3057-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-017-3057-z