
Abstract
Background
Educating medical trainees across the continuum is essential to a multifaceted strategy for addressing the opioid epidemic.
Objective
To assess the current state of internal medicine clerkship content on safe opioid prescribing and opioid use disorder, and barriers to curriculum implementation.
Design
National Annual (2018) Clerkship Directors in Internal Medicine (CDIM) cross-sectional survey.
Participants
One hundred thirty-four clerkship directors at all Liaison Committee of Medical Education accredited US medical schools with CDIM membership as of October 1, 2018.
Main Measures
The survey section on safe opioid prescribing and opioid use disorder education in the internal medicine clerkship addressed assessment of current curricula, perceived importance of curricula, barriers to implementation, and plans to start or expand curricula. Descriptive statistics were used to summarize responses, and Pearson’s chi-square and Fisher’s exact tests for statistical comparisons.
Key Results
The survey response rate was 82% (110/134). Overall 54.1% of responding institutions reported covering one or more topics related to safe opioid prescribing or opioid use disorder in the internal medicine clerkship. A preponderance of clerkship directors (range 51–86%) reported that various opioid-related topics were important to cover in the internal medicine clerkship. Safe opioid prescribing topics were covered more frequently than topics related specifically to opioid use disorder. The main barriers identified included time (80.9%) and lack of faculty expertise (65.5%).
Conclusions
Clerkship directors agreed that incorporating safe opioid prescribing and opioid use disorder topics in the internal medicine clerkship is important, despite wide variation in current curricula. Addressing curricular time constraints and lack of faculty expertise in internal medicine clerkships will be key to successfully integrating content to address the opioid epidemic.
Similar content being viewed by others


INTRODUCTION
The USA is grappling with two highly publicized and intertwined problems. First, chronic pain affects millions of Americans, many of whom are prescribed chronic opioid therapy, medications with potential benefit but clear risks. In 2016, more than 11 million Americans misused prescription opioids, and opioid pain reliever medications were involved in about half of the over 40,000 opioid overdose deaths.1, 2 Second, 21 million people in the USA have substance use disorders, but most individuals do not receive treatment despite the availability of effective treatments.3
In response to the opioid epidemic, the Association of American Medical Colleges (AAMC) committed to “better educate the next generation of health care workers on opioid misuse and substance use disorders.”4 A 2016 AAMC statement highlighted that to be “maximally effective,” education on substance abuse and pain management must be “reinforced throughout the continuum of medical education,” and across the many different specialties that intersect with pain and addiction.4 According to the Liaison Committee on Medical Education (LCME) 2014–2015 Annual Medical Student Questionnaire, 131 of 141 medical schools reported content on substance abuse in one or more required clerkships, and 130 reported including content on pain management.4 A national telephone survey of curriculum deans undertaken by the AAMC in 2017 revealed 87% of responding medical schools cover all four assessed domains related to pain and substance use disorders in their institutions’ curricula (100% cover at least two), with the majority of institutions reporting content across all 4 years of medical school.5 Nearly all respondents highlighted challenges in faculty development/expertise, curricular time, and assessment.5 However, current coverage is likely insufficient in quantity, may be ineffectively taught, and focused more on basic science topics than the clinical conditions, attitudes, and treatment skills needed to adequately care for patients.5,6,7 Individual medical schools and state-wide collaborations, often in areas particularly affected by the opioid epidemic, have begun to address this topic in more comprehensive and innovative ways, developing core competencies and progressive, integrated content.4, 8, 9
Medical trainees in internal medicine (IM) frequently encounter patients with chronic pain, acute intoxication, withdrawal, and substance use disorders. A 2013 study of IM residents at Massachusetts General Hospital reported that residents estimated ~ 25% of inpatients they cared for met criteria for a substance use disorder.10 While all physicians need to understand how chronic pain and substance use affect their specialty’s conditions and patient population, internists are well-trained in many skills needed to care for this population successfully. Skills central for chronic disease management of other conditions including screening for chronic health problems, managing multiple conditions, knowing when patients need specialty care, and integrating the patient’s social situation into the biomedical model can be transferred effectively to patients with chronic pain and substance use disorders.6, 11 Given the combination of frequent exposure to substance use disorders and key competencies of the specialty, IM clinical education is an important point along the training continuum for this education to occur.
Despite the recent attention and commitment to this topic, the current state of medical student training in opioid use disorder and safe opioid prescribing during the IM clerkship is unknown. Improved understanding of the scope and importance of this topic’s representation within IM is an important step to plan future areas for curricular design. This study aimed to first assess the current state of IM clerkship content on safe opioid prescribing and opioid use disorder. Second, we evaluated core clerkship directors’ perspectives on the ideal state of IM clerkship coverage of these topics, barriers to implementation, and planned changes given the backdrop of the opioid epidemic.
METHODS
On October 1, 2018, the Clerkship Directors in Internal Medicine (CDIM) conducted its annual, voluntary, and confidential survey of clerkship directors (CD) at all LCME-accredited US medical schools with current CDIM membership. CDIM members designated as “clerkship director” received a personal email invitation to complete the web-based survey. Only one individual per member school received the invitation. Approximately 88% (136/154) of LCME-accredited schools were represented in CDIM during the survey period.
The survey questions were written and revised for content validity in reference to past CDIM Annual Survey questions using best practices of survey design by the authors and the CDIM Survey and Scholarship Committee. The elected CDIM Council reviewed the questions and made further revisions before final approval. The authors, survey committee members, and Council members consisted of subject matter experts with extensive experience in the clinical clerkship setting. The survey consisted of four thematic sections as well as a section on respondents’ demographic characteristics including attributes such as their faculty rank, and a two-item screening question for possible burnout. The section “Safe Opioid Prescribing and Opioid Use Disorder” consisted of 10 questions, including multiple-choice, 5-point Likert scale (ranging from very important to very unimportant), and open-text response options, and included logical skip and display patterns (Appendix). Question domains included current topics of formal instruction on safe opioid prescribing and opioid use disorder, perceived importance to teaching this content in the IM clerkship and across the medical school curriculum, barriers to curriculum implementation, and plans to start or expand content in this area.
The survey was administered to 134 of 136 possible respondents (due to two opt-outs) via Qualtrics survey software using Secure Socket Layer encryption, with unique survey participation URLs sent to the survey population via email. The survey launched on October 2, 2018, and closed on November 30, and included five email reminders to non-respondents. The study (number: 18-AAIM-102) was submitted to Pearl IRB for exemption determination in accordance with FDA 21 CFR 56.104 and DHHS 45 CFR 46.101 regulations, and was deemed exempt under 45 CFR 46.101(b) category 2. Only Alliance for Academic Internal Medicine (AAIM) surveys staff (MK) had access to the survey software and dataset during fielding. Following data collection, a variable to denote respondents’ and non-respondents’ medical school as “public” or “private” was merged into the dataset, using publicly available data and visits to medical school websites.12 Using CDIM membership files, data on respondents’ and non-respondents’ self-reported gender, and US Census Bureau geographic region of their school were merged into the dataset.13 All respondent contact information was handled by MK. Upon survey closure, all survey data were downloaded to a local network drive accessible only to MK, deleted from the survey software, and de-identified prior to analysis. No other co-authors had access to the survey dataset prior to de-identification. Due to the high survey response rate and lack of statistically significant differences between survey respondents and non-respondents, the data were not weight-adjusted for non-response. Due to item non-response or survey conditional logic, some denominators vary and do not sum to 110. We used descriptive statistics to summarize our responses, and Pearson’s chi-square and Fisher’s exact tests for statistical comparisons. Statistical analysis was performed in Stata 14.2 for Windows (Stata Corp, College Station, TX).
RESULTS
The survey response rate was 82% (110/134). There were no statistically significant differences between respondents and non-respondents based on the three variables merged into the dataset after fielding: medical school type (public/private), US Census Bureau region, and gender of respondent. Not all respondents answered all questions; denominators other than 110 are denoted below. Of the respondents, 65/110 (59.1%) were employed at public medical schools, and 50/110 (45.5%) were female. Distribution of respondents (n = 110) by US Census Bureau Region included 24 (21.8%) from the Northeast, 29 (26.4%) from the Midwest, 45 (40.9%) from the South, and 12 (10.9%) from the West.
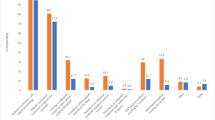
At the time of the survey, 54.1% (59/109) of responding institutions reported covering one or more topics related to safe opioid prescribing or opioid use disorder in the IM clerkship. A wide variety of topics are covered (Table 1), most frequently opioid dosing, communicating effectively with patients about the safe use of opioids, and safe opioid prescribing. Topics related more specifically to opioid use disorder, including screening, brief intervention and referral to treatment (SBIRT), and medication-assisted treatment were less frequently covered. Coverage of at least some opioid topics varied by geographic region (range 33.3–72.4%, Fig. 1), with only Midwest medical schools covering content at a statistically higher rate than would be expected based on the distribution of medical schools by region (p = 0.02). There was no difference in coverage of some topics between public and private medical schools (59.4% vs 46.7%, p = 0.19).

Safe opioid prescribing and opioid use disorder topic offering in the Internal Medicine Clerkship by Geographic Region of Medical Schools (percent reporting “Yes”).
All topics were reported to be either somewhat important or very important to cover in the IM clerkship by a preponderance of respondents (range 51–86%) (Table 1). There was a sizable gap between percent currently covering and percent reporting importance to cover (range 37–64%). Respondents whose clerkships do not currently offer specific topic coverage had a statistically lower rate of self-reported importance compared to those whose clerkships are currently covering for seven of eight topics (all except opioid use disorder screening) (Table 2). There was a relatively even distribution of respondents who thought content should also be taught in the pre-clerkship setting (range 28–56%), core clerkships other than IM (range 36–58%), and after core clerkships (range 36–53%). Several open-ended comments stated that this content should be taught longitudinally and horizontally (e.g., threads, intersessions, annual “opioid day,” doctoring courses).
The main barriers identified to incorporating content on safe opioid prescribing and opioid use disorder included lack of time (80.9%, 89/110) and lack of faculty expertise (65.5%, 72/110) (Table 3). Of those institutions not currently covering this topic in the IM clerkship, only 12% (6/50) reported plans to begin covering this content in the next 12 months with the remainder either unsure or not planning to begin covering (Table 4). Reasons to begin covering topics included more information about the opioid epidemic, increased availability of educators, institutional directives, and curricular changes. A larger percentage (34%, 20/58) of those currently covering this topic had plans to expand content (Table 4).
Most respondents indicated that educational resources would be either be helpful (48.6%, 53/109) or possibly helpful (41.3%, 45/109). The most commonly requested resources included sample cases for discussion (81.7%, 76/93), educational videos (66.7%, 62/93), and standardized patient cases (61.3%, 57/93).
DISCUSSION
The results of this survey are the most comprehensive assessment of IM clerkship curricula addressing safe opioid prescribing and opioid use disorder topics to date, and can help guide planning for medical school clerkship directors. Although specialty focused, the results provide specific insight into IM education leaders’ current and perceived ideal coverage of this topic and highlights key barriers to successful education across the continuum.
Only 54.1% of responding institutions reported covering one or more topics related to safe opioid prescribing or opioid use disorder in the IM clerkship. Some topics (opioid dosing, communicating effectively with patients about the safe use of opioids, safe opioid prescribing) were more frequently covered compared to other topics (opioid use disorder screening, SBIRT, medication-assisted treatment). In contrast to our findings, the 2017 AAMC survey reported higher levels of curricular coverage during the third year of medical school on four domains of pain: the nature of pain (67%), pain assessment and measurement (81%), management of pain including SUD treatment and opioid overdose (86%), and the context of pain and SUDs (75%).5 This suggests that content is more frequently being taught in non-IM parts of the third year. Although there was no difference in coverage between public and private medical schools, there was some regional variation. Based on the distribution of medical schools, we expected a smaller percentage of schools that offer content to be composed of Midwest schools, but it was higher than expected. This may be due to regional specific initiatives to address this issue.4, 8, 9
Notably, all topics were reported as important to cover in the IM clerkship by a majority of respondents, even among institutions without curricula, though the rate was higher among clerkships that are already covering topics on 7 of 8 topics. The percentage gap between current coverage and perceived importance of coverage in the IM clerkship curriculum was sizable for all topics (37–64%). This indicates a gap between the current and ideal states of IM clerkship curricula and a potential need for curriculum reform.
Similar to past data, lack of time and lack of faculty expertise were the most commonly cited barriers to further curriculum implementation.5 Interestingly, of the nearly half of institutions not currently covering this content, very few reported plans to begin though it is unclear whether this is due to more established coverage in non-IM clerkship parts of the curriculum or cited barriers. It is also possible that this topic is already being covered on an ad hoc basis as individual patients are treated on the wards and in the clinic. Those who were already covering some content were statistically associated with having plans to expand coverage, possibly due to in-house faculty expertise or institutional momentum. Forty-nine percent of respondents reported that education resources such as sample cases for discussion, educational videos, and standardized patient cases would be helpful to address educational gaps. Existing local expertise, within hospitalist and primary care internist groups, should also be sought out and accessed to address implementation barriers.
Our findings have several limitations. Although the survey response rate was high, the survey was not inclusive of all medical schools, and it obtained data from the knowledge and opinions of a single individual: the core clerkship director. Clerkship directors may not be aware of broader institutional efforts surrounding this topic, especially as it relates to longitudinal or interdisciplinary/interprofessional education. We were not able to study effectiveness or outcomes related to current curriculum. Also, as this field rapidly gains more attention with increasing calls for a larger role for medical education, answers may not be reflective of current practice. Nevertheless, the high response rate and representativeness of the survey results relative to the eligible survey population suggests that non-response bias was low, and the relatively high item response rate to survey questions further supports this.
Alongside the AAMC’s commitment to support member institutions as they advance medical research, education and clinical care to address the opioid epidemic, there have been several calls to improve medical student education surrounding safe opioid prescribing and opioid use disorder,4, 6, 7, 9 though the optimal way to deliver this education has yet to be determined. Echoing the AAMC’s belief that integration throughout the continuum of medical education is paramount for maximizing learning, respondents reported that content should also be taught in the pre-clerkship setting, core clerkships other than IM, after core clerkships, and through longitudinal threads/intersessions and interprofessional activities.4 LCME survey data indicate that a substantial majority of medical schools are covering topics related to multiple pain domains including the nature of pain, pain assessment and measurement, management of pain, including substance use disorder treatment and opioid overdose, and the context of pain and substance use disorders, and that this content is present in both pre-clerkship and clerkship curricula.4, 5 However, our survey’s more granular snapshot of IM clerkship coverage, together with other data, demonstrates that significant opportunity for improvement still exists.6, 7 These include increasing the quantity of education, focusing less on the scientific knowledge associated with addiction and more on the attitudes and treatment skills necessary to reduce stigma and provide evidence-based care, building more engaging/interactive curricular models, and responding to shifts in the evolving demographics and trends of the opioid epidemic, for example the rise of fentanyl-related overdoses.5,6,7
Given the need to optimize education surrounding pain management and opioid use disorder in the era of the opioid epidemic, one might ask whether IM clerkships are the appropriate setting in which to invest curricular time and resources, or whether this content is better housed in other clerkships (e.g., psychiatry) or later or earlier in undergraduate medical education. Given how commonly patients with chronic pain on opioids and patients with opioid use disorder are encountered on IM services, it is a natural fit to discuss aspects of screening, diagnosis, and treatment using the chronic disease framework internists use to approach other frequently encountered diseases.10, 14 Specific topics included in our survey, including SBIRT, discussions of risk reduction and communicating effectively with patients about safe use of opioids, are practical clinical skills that can be taught and demonstrated on rounds or at the bedside. It can also serve as a prime example of a topic that allows interweaving of “hidden curriculum” content related to health disparities and stigma and thus should be addressed longitudinally during clinical training.6, 14, 15
State-wide and national initiatives to bolster education on this topic for medical trainees are growing.4, 8, 9 Ensuring undergraduate medical education aligns with growth in graduate medical level training is an important step in preparing a workforce to care for patients with chronic pain safely and recognize and manage those with opioid use effectively by the end of training.16,17,18,19 Based on the survey results, IM clerkship directors believe that incorporating safe opioid prescribing and opioid use disorder topics into the IM clerkship is important. Optimal practices have yet to be established and constraints in the form of curricular time and faculty expertise exist and must be addressed. Future efforts should focus on decreasing barriers to curricular implementation, as well as disseminating and collaborating on engaging and effective evidence-based IM clerkship curricula as part of a comprehensive medical education approach to addressing the opioid epidemic.
References
Volkow N. Statement on federal efforts to combat the opioid crisis: a status update on CARA and other initiatives before the House Committee on Energy and Commerce. https://www.drugabuse.gov/about-nida/legislative-activities/testimony-to-congress/2017/federal-efforts-to-combat-opioid-crisis-status-update-cara-other-initiatives. Accessed May 21, 2019.
Centers for Disease Control and Prevention. Opioid overdose: understanding the epidemic. https://www.cdc.gov/drugoverdose/epidemic/. Revised December 18, 2018. Accessed May 21, 2019.
Center for Behavioral Health Statistics and Quality. Key substance use and mental health indicators in the United States: Results from the 2015 National Survey on Drug Use and Health. https://www.samhsa.gov/data/sites/default/files/NSDUH-FFR1-2015/NSDUH-FFR1-2015/NSDUH-FFR1-2015.pdf. Published September 2016. Accessed May 21, 2019.
Educating future physicians of substance abuse and pain management [news release]. Washington, DC: Association of American Medical Colleges; January, 2016. https://www.aamc.org/download/453538/data/20160129_educatingfuturephysiciansonsubstanceabuseandpainmanage.pdf. Accessed May 21, 2019.
Howley L, Whelan A, Rasouli T. Addressing the opioid epidemic: U.S. medical school curricular approaches. AAMC Analysis in Brief. 2018;18(1):1–3. https://www.aamc.org/download/485934/data/january2018addressingtheopioidepidemicu.s.medicalschoolcurricul.pdf. Accessed May 21, 2019.
Ram A, Chisolm MS. The Time is Now: Improving Substance Abuse Training in Medical Schools. Acad Psychiatry. 2016;40(3):454–460.
Ratycz MC, Papadimos TJ, Vanderbilt AA. Addressing the growing opioid and heroin abuse epidemic: a call for medical school curricula. Med Educ Online. 2018;23(1):1466574.
Antman KH, Berman HA, Flotte TR, Flier J, Dimitri DM, Bharel M. Developing Core Competencies for the Prevention and Management of Prescription Drug Misuse: A Medical Education Collaboration in Massachusetts. Acad Med. 2016;91(10):1348–1351.
Responding to the opioid epidemic through education, patient care and research [news release]. Washington, DC: Association of American Medical Colleges; May 14, 2019. https://news.aamc.org/for-the-media/article/medical-schools-address-opioid-epidemic/. Accessed May 21, 2019.
Wakeman SE, Baggett MV, Pham-Kanter G, Campbell EG. Internal medicine residents’ training in substance use disorders: a survey of the quality of instruction and residents’ self-perceived preparedness to diagnose and treat addiction. Subst Abus. 2013;34(4):363–370.
Saitz R, Daaleman TP. Now is the Time to Address Substance Use Disorders in Primary Care. Ann Fam Med. 2017;15(4):306–308.
Liasion Committee on Medical Education (LCME). Medical School Directory. http://lcme.org/directory. Accessed September 1, 2017.
US Census Bureau. Census Regions and Divisions of the United States. www.census.gov/geo/www/us_regdiv.pdf. Accessed December 1, 2017.
Rice K, Ryu JE, Whitehead C, Katz J, Webster F. Medical Trainees’ Experiences of Treating People With Chronic Pain: A Lost Opportunity for Medical Education. Acad Med. 2018;93(5):775–780.
Meltzer EC, Suppes A, Burns S, et al. Stigmatization of substance use disorders among internal medicine residents. Subst Abus. 2013;34(4):356–362.
Isaacson JH, Fleming M, Kraus M, Kahn R, Mundt M. A national survey of training in substance use disorders in residency programs. J Stud Alcohol. 2000;61(6):912–915.
Tesema L, Marshall J, Hathaway R, et al. Training in office-based opioid treatment with buprenorphine in US residency programs: A national survey of residency program directors. Subst Abus. 2018:1–7.
Tong S, Sabo R, Aycock R, et al. Assessment of Addiction Medicine Training in Family Medicine Residency Programs: A CERA Study. Fam Med. 2017;49(7):537–543.
Schwartz AC, Frank A, Welsh JW, Blankenship K, DeJong SM. Addictions Training in General Psychiatry Training Programs: Current Gaps and Barriers. Acad Psychiatry. 2018;42(5):642–647.
Contributors
The authors wish to thank the Alliance for Academic Internal Medicine (AAIM) and the Clerkship Directors in Internal Medicine (CDIM).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they do not have a conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 33 kb)
Rights and permissions
About this article

Cite this article
Ari, M., Kisielewski, M., Osman, N.Y. et al. Teaching Safe Opioid Prescribing During the Opioid Epidemic: Results of the 2018 Clerkship Directors in Internal Medicine Survey. J GEN INTERN MED 34, 2812–2817 (2019). https://doi.org/10.1007/s11606-019-05203-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-019-05203-3