
Abstract
BACKGROUND
Despite mounting evidence that peer coaches can make significant contributions to patient health, little is known about factors that must be addressed to engage and retain them in their role.
OBJECTIVE
To identify motivators and barriers to serving as a peer coach.
DESIGN
Open ended semi-structured interviews.
PARTICIPANTS AND SETTING
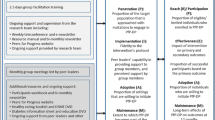
In a randomized trial of peer support, patients with well controlled hypertension and good interpersonal skills were recruited and trained to serve as peer coaches for African-American patients from the same practices who had poorly controlled hypertension. Peer coaches spoke by telephone at least three times with their same sex patient–clients on alternate months during the 6-month intervention and counseled about medication adherence as well as other healthy lifestyles.
KEY RESULTS
Of 15 trained peer coaches, ten were contacted and agreed to participate in the qualitative interview. Peer coaches had a mean age of 66 years, 50% were women, and 80% were African-American. Themes regarding favorable aspects of the peer coach experience included: meaning and satisfaction derived from contributing to community health and the personal emotional and physical benefits derived from serving as a peer coach. Negative aspects centered on: challenges in establishing the initial telephone contact and wanting more information about their patient–clients’ personal health conditions and status. Peer coaches endorsed gender matching but were less clear about race-matching.
CONCLUSIONS
Programs that utilize peer support to enhance positive health behaviors should recognize that a spirit of volunteerism motivates many successful peer coaches. Program planners should acknowledge the special characteristics required of successful peer coaches when selecting, motivating and training individuals for this role.

Similar content being viewed by others


References
Feierman S, Janzen JM, eds. The social basis of health and healing in Africa. Berkeley: University of California Press; 1992.
Donelan K, Mailhot JR, Dutwin D, et al. Patient perspectives of clinical care and patient navigation in follow-up of abnormal mammography. J Gen Intern Med. 2011;26(2):116–22.
Steinberg ML, Fremont A, Khan DC, et al. Lay patient navigator program implementation for equal access to cancer care and clinical trials. Cancer. 2006;107(11):2669–77.
Hiatt RA, Pasick RJ, Stewart S. Community-based cancer screening for underserved women: design and baseline findings from the breast and cervical cancer intervention study. Prev Med. 2001;33(3):190–203.
Jandorf L, Gutierrez Y, Lopez J, Christie J, Itzkowitz SH. Use of a patient navigator to increase colorectal cancer screening in an urban neighborhood health clinic. J Urban Health. 2005;82(2):216–24.
Perac-Lima S, Grant RW, Green AR, et al. A culturally tailored navigator program for colorectal cancer screening in a community health center: a randomized, controlled trial. J Gen Intern Med. 2009;24(2):211–7.
Ferrante JM, Chen P, Kim S. The effect of patient navigation on time to diagnosis, anxiety, and satisfaction in urban minority women with abnormal mammograms: a randomized controlled trial. J Urban Health. 2008;85(1):114–24.
Heisler M, Piette JD. “I help you, and you help me”: facilitated telephone peer support among patients with diabetes. Diabetes Educ. 2005;31:869–79.
Vale M, Jelinek MV, Best JD. Impact of coaching patients on coronary risk factors: lessons from the COACH program. Dis Manag Health Outcomes. 2005;13(4):225–44.
Douglas JG, Bakris GL, Epstein M. Management of high blood pressure in African Americans: consensus statement of the hypertension in African Americans working group of the international society on hypertension in blacks. Arch Intern Med. 2003;163:525–41.
Freund KM. Patient navigation: the promise to reduce health disparities. J Gen Intern Med. 2010;26(2):110–2.
Phillips CE, Rothstein JD, Beaver K, et al. Patient navigation to increase mammography screening among inner city women. J Gen Intern Med. 2010;26(2):123–9.
Thoits PA. Social support as coping assistance. J Consult Clin Psychol. 1986;54(4):416–23.
Charmaz K. Grounded theory: objectivist and constructivist methods. In: Denzin NK, Lincoln YS, eds. Handbook of qualitative research. Thousand Oaks: Sage; 2000.
Wells KJ, et al. Innovative approaches to reducing cancer health disparities: the moffitt cancer center patient navigator research program. J Cancer Educ. 2011; epub ahead of print.
Turner BJ, et al. Overcoming poor attendance to first scheduled colonoscopy: a randomized trial of peer coach or brochure support. J Gen Intern Med. 2008;23(1):58–63.
Frimer JA, Walker LJ, Dunlop WL, et al. The integration of agency and communion in moral personality: evidence of enlightened self-interest. J Personal Soc Psychol. 2011;101(1):149–63.
Haski-Leventhal D, Ben-Arieh A, Melton GB. Between neighborliness and volunteerism. Fam Community Health. 2008;31(2):150–61.
Heisler M, Vijan S, Makki F, Piette JD. Diabetes control with reciprocal peer support versus nurse care management: a randomized trial. Ann Intern Med. 2010;153(8):507–15.
Patient Protection and Affordable Care Act of 2010 Public Law 111–148, 24 Stat. 119 (March 23, 2010)
Meir ER, Olson BH, Benton P, Eghtedary K, Song WO. A qualitative evaluation of a breastfeeding peer counselor program. J Hum Lact. 2007;23(3):262–8.
Nguyen TN, Jacqueline TH, Marjorie K, Mary AF. A qualitative assessment of community-based breast health navigation services for Southeast Asian women in Southern California: recommendations for developing a navigator training curriculum. Am J Public Health. 2011;101(1):87–93.
Blanchard J, Nayar S, Lurie N. Patient-provider and patient-staff racial concordance and perceptions of mistreatment in the health care setting. J Gen Intern Med. 2007;22(8):1184–9.
Kneipp SM, Lutz BJ. Means. Reasons for enrollment, the informed consent process, and trust among low-income women participating in a community-based participatory research study. Public Health Nurs. 2009;26(4):362–9.
Street RL, O'Malley KJ, Cooper LA, Haidet P. Understanding concordance in patient-physician relationships: personal and ethnic dimensions of shared identity. Ann Fam Med. 2008;6(3):198–205.
Hilfinger Messias DK, Moneyham L, Vyavaharkar M, Murdaugh C, Phillips KD. Embodied work: insider perspectives on the work of HIV/AIDS peer counselors. Health Care Women Int. 2009;30(7):572–94.
Funding Source
Funded by the Robert Wood Johnson Foundation Informing Disparities Program
Prior Presentations
Material included in this paper was presented in a poster session at the SGIM meeting in Minneapolis, MN, April 2010.
The authors wish to acknowledge the contribution of the Mixed Methods Research Lab (MMRL) at the University of Pennsylvania, Department of Family Medicine and Community Health, in the management and analysis of the data.
Conflict of Interest
None disclosed.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Appendix 1
(DOC 24 kb)
Appendix 2
(PPT 462 kb)
Appendix 3
(DOC 28 kb)
Rights and permissions
About this article
Cite this article
Barg, F.K., Weiner, M.G., Joseph, S. et al. Qualitative Analysis of Peer Coaches’ Experiences with Counseling African Americans About Reducing Heart Disease Risk. J GEN INTERN MED 27, 167–172 (2012). https://doi.org/10.1007/s11606-011-1883-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-011-1883-6