
Abstract
Introduction
Severe acute kidney injury (AKI-D) is common in critically ill patients and contributes substantially to short- and long-term morbidity and mortality. Acute renal replacement therapy (RRT) is an increasingly widely utilized life-sustaining support strategy for AKI-D patients, providing a bridge to renal recovery in many survivors of AKI. However, key aspects (when and how) of this therapy’s appropriate cessation remain unclear. Today, wide variation in clinical practice exists regarding the indication for and the timing of RTT discontinuation, likely due to the poor current evidence base.
Methods
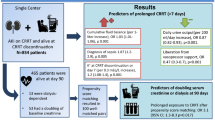
Few studies have evaluated the process of weaning or ideal markers (clinical factors or parameters that may suggest renal recovery, such as urine output, urine chemistry, and creatinine clearance) to predict sufficient recovery of renal function following AKI and to avoid re-institution of RRT. However, translation of the current evidence to clinical practice is hampered by considerable limitations of the retrospective, post hoc secondary design of cohort studies, small sample sizes, heterogeneity across study populations and illness severity, variations of the thresholds of predictive markers and conflicting results for given markers. Currently, 24-h creatinine clearance greater than 20 ml/min combined with spontaneously decreasing serum creatinine concentrations in the context of fixed RRT and a clinically stable intensive care unit (ICU) patient may be the best predictor of recovery of excretory renal function.
Conclusion
The decision regarding the appropriate time to wean acute RRT is complex, integrating numerous clinical variables and renal functional parameters. Cessation of RRT should largely be individualized in critically ill patients. Large randomized multicentre trials are needed to definitively answer the vitally important question of whether inappropriate discontinuation of RRT in ICU patients with AKI-D impacts patient outcomes. Future work should integrate novel kidney damage and repair biomarkers and techniques to measure real-time glomerular filtration rates.

Similar content being viewed by others

References
Hoste EA, Bagshaw SM, Bellomo R, Cely CM, Colman R, Cruz DN, Edipidis K, Forni LG, Gomersall CD, Govil D, Honore PM, Joannes-Boyau O, Joannidis M, Korhonen AM, Lavrentieva A, Mehta RL, Palevsky P, Roessler E, Ronco C, Uchino S, Vazquez JA, Vidal Andrade E, Webb S, Kellum JA (2015) Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study. Intensive Care Med 41(8):1411–1423. https://doi.org/10.1007/s00134-015-3934-7
Bellomo R, Ronco C, Mehta RL, Asfar P, Boisrame-Helms J, Darmon M, Diehl JL, Duranteau J, Hoste EAJ, Olivier JB, Legrand M, Lerolle N, Malbrain M, Martensson J, Oudemans-van Straaten HM, Parienti JJ, Payen D, Perinel S, Peters E, Pickkers P, Rondeau E, Schetz M, Vinsonneau C, Wendon J, Zhang L, Laterre PF (2017) Acute kidney injury in the ICU: from injury to recovery: reports from the 5th Paris International Conference. Ann Intensive Care 7(1):49. https://doi.org/10.1186/s13613-017-0260-y
Schiffl H, Lang SM, Fischer R (2012) Long-term outcomes of survivors of ICU acute kidney injury requiring renal replacement therapy: a 10-year prospective cohort study. Clin Kidney J 5(4):297–302. https://doi.org/10.1093/ckj/sfs070
Romagnoli S, Clark WR, Ricci Z, Ronco C (2017) Renal replacement therapy for AKI: when? how much? when to stop? Best Pract Res Clin Anaesthesiol 31(3):371–385. https://doi.org/10.1016/j.bpa.2017.10.001
Klouche K, Gibney RTN, Forni LG (2017) Can this patient be safely weaned from RRT? Intensive Care Med. https://doi.org/10.1007/s00134-017-4948-0
Group KDIGOKAKiW (2012) KDIGO clinical practice guideline for acute kidney injury. Kidney Int 2:1–138
Clark EG, Bagshaw SM (2015) Unnecessary renal replacement therapy for acute kidney injury is harmful for renal recovery. Semin Dial 28(1):6–11. https://doi.org/10.1111/sdi.12300
Jones SL, Devonald MA (2013) How acute kidney injury is investigated and managed in UK intensive care units–a survey of current practice. Nephrol Dial Transplant 28(5):1186–1190. https://doi.org/10.1093/ndt/gft015
Wu VC, Ko WJ, Chang HW, Chen YW, Lin YF, Shiao CC, Chen YM, Chen YS, Tsai PR, Hu FC, Wang JY, Lin YH, Wu KD (2008) Risk factors of early redialysis after weaning from postoperative acute renal replacement therapy. Intensive Care Med 34(1):101–108. https://doi.org/10.1007/s00134-007-0813-x
Uchino S, Bellomo R, Morimatsu H, Morgera S, Schetz M, Tan I, Bouman C, Macedo E, Gibney N, Tolwani A, Straaten HO, Ronco C, Kellum JA (2009) Discontinuation of continuous renal replacement therapy: a post hoc analysis of a prospective multicenter observational study. Crit Care Med 37(9):2576–2582. https://doi.org/10.1097/CCM.0b013e3181a38241
Katayama S, Uchino S, Uji M, Ohnuma T, Namba Y, Kawarazaki H, Toki N, Takeda K, Yasuda H, Izawa J, Tokuhira N, Nagata I (2016) Factors predicting successful discontinuation of continuous renal replacement therapy. Anaesth Intensive Care 44(4):453–457
Tsukamoto I, Tsuchiya Y, Suzuki H, Watanabe Y, Sueyoshi K, Okada H (2014) Evaluation of the time to terminate continuous renal replacement therapy in patients with acute kidney injury following cardiovascular surgery in association with or without a mechanical ventilation support. J Nephrol Ther 5(1):1000188
Raurich JM, Llompart-Pou JA, Novo MA, Talavera C, Ferreruela M, Ayestaran I (2018) Successful weaning from continuous renal replacement therapy. Associated risk factors. J Crit Care 45:144–148. https://doi.org/10.1016/j.jcrc.2018.02.009
Bouman CS, Oudemans-Van Straaten HM, Tijssen JG, Zandstra DF, Kesecioglu J (2002) Effects of early high-volume continuous venovenous hemofiltration on survival and recovery of renal function in intensive care patients with acute renal failure: a prospective, randomized trial. Crit Care Med 30(10):2205–2211. https://doi.org/10.1097/01.ccm.0000030444.21921.ef
Gaudry S, Hajage D, Schortgen F, Martin-Lefevre L, Pons B, Boulet E, Boyer A, Chevrel G, Lerolle N, Carpentier D, de Prost N, Lautrette A, Bretagnol A, Mayaux J, Nseir S, Megarbane B, Thirion M, Forel JM, Maizel J, Yonis H, Markowicz P, Thiery G, Tubach F, Ricard JD, Dreyfuss D (2016) Initiation strategies for renal-replacement therapy in the intensive care unit. N Engl J Med 375(2):122–133. https://doi.org/10.1056/NEJMoa1603017
Zarbock A, Kellum JA, Schmidt C, Van Aken H, Wempe C, Pavenstadt H, Boanta A, Gerss J, Meersch M (2016) Effect of early vs delayed initiation of renal replacement therapy on mortality in critically ill patients with acute kidney injury: the ELAIN Randomized Clinical Trial. Jama 315(20):2190–2199. https://doi.org/10.1001/jama.2016.5828
Viallet N, Brunot V, Kuster N, Daubin D, Besnard N, Platon L, Buzancais A, Larcher R, Jonquet O, Klouche K (2016) Daily urinary creatinine predicts the weaning of renal replacement therapy in ICU acute kidney injury patients. Ann Intensive Care 6(1):71. https://doi.org/10.1186/s13613-016-0176-y
Aniort J, Ait Hssain A, Pereira B, Coupez E, Pioche PA, Leroy C, Heng AE, Souweine B, Lautrette A (2016) Daily urinary urea excretion to guide intermittent hemodialysis weaning in critically ill patients. Crit Care 20:43. https://doi.org/10.1186/s13054-016-1225-5
Frohlich S, Donnelly A, Solymos O, Conlon N (2012) Use of 2-hour creatinine clearance to guide cessation of continuous renal replacement therapy. J Crit Care 27(6):744.e741–744.e745. https://doi.org/10.1016/j.jcrc.2012.08.012
Palevsky PM, Zhang JH, O’Connor TZ, Chertow GM, Crowley ST, Choudhury D, Finkel K, Kellum JA, Paganini E, Schein RM, Smith MW, Swanson KM, Thompson BT, Vijayan A, Watnick S, Star RA, Peduzzi P (2008) Intensity of renal support in critically ill patients with acute kidney injury. N Engl J Med 359(1):7–20. https://doi.org/10.1056/NEJMoa0802639
Schiffl H, Lang SM (2013) Severe acute hypophosphatemia during renal replacement therapy adversely affects outcome of critically ill patients with acute kidney injury. Int Urol Nephrol 45(1):191–197. https://doi.org/10.1007/s11255-011-0112-x
Wheeler TS, Tolwani AJ (2007) 165 The 24-hour urine creatinine clearance predicts successful discontinuation of continuous renal replacement therapy in acute renal failure. J Investig Med 55(1):S274–S274
Yang T, Sun S, Zhao Y, Liu Q, Han M, Lin L, Su B, Huang S, Yang L (2018) Biomarkers upon discontinuation of renal replacement therapy predict 60-day survival and renal recovery in critically ill patients with acute kidney injury. Hemodialysis Int 22(1):56–65. https://doi.org/10.1111/hdi.12532
Yang T, Zhao Y, Liu Q, Han M, Sun S, Lin L, Su B, Huang S (2016) Prognostic biomarkers at discontinuation of renal replacement therapy in acute kidney injury patients in the intensive care unit. Blood Purif 42(4):347–348. https://doi.org/10.1159/000452242
Han SS, Bae E, Song SH, Kim DK, Kim YS, Han JS, Joo KW (2016) NT-proBNP is predictive of the weaning from continuous renal replacement therapy. Tohoku J Exp Med 239(1):1–8. https://doi.org/10.1620/tjem.239.1
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The author declares that he has no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Schiffl, H. Discontinuation of renal replacement therapy in critically ill patients with severe acute kidney injury: predictive factors of renal function recovery. Int Urol Nephrol 50, 1845–1851 (2018). https://doi.org/10.1007/s11255-018-1947-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-018-1947-1