
Abstract
Background
Vascular calcification (VC) is common and is both a marker and a cause of increased cardiovascular morbidity and mortality, especially so in chronic kidney disease (CKD) patients. Renal transplantation is the cornerstone of the successful long-term management of CKD, and in order to satisfy transplantation needs, more use is made now of living kidney donors (LKD). Prior to selection for transplantation, much screening of potential LKD takes place, including for cardiovascular issues. It is not known; however, how much these potentially healthy LKD may be prone to clinically silent VC.
Methods
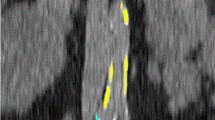
We identified 103 living kidney donors from 2011 renal transplant records. Abdominal aortic calcification (AAC) was assessed using existing abdominal CT imaging using multi-channel CT aortograms (used primarily to assess renal vascular anatomy). Using these CT scans, manual calcium scoring was undertaken to calculate total aortic calcium load (AAC severity score). The prevalence, severity and associations of AAC between calcified and non-calcified donors were then compared.
Results
A total of 103 donors were identified from records. Ninety three of these had detailed clinical records to complement their CT scans. Fifty of ninety-three donors were male, and the mean age was 45.9 ± 1.8 years. Mean MDRD eGFR was 88.73 ± 2.97 ml/min/1.73 m2. 7.14 ± 3.07 % of the aorta in these donors was calcified with a mean AAC severity score of 0.98 ± 0.56. In kidney donors >50 years of age, there was significantly more AAC than in those <50: 2.47 ± 1.56 versus 0.31 ± 0.29, p < 0.001. There was no relationship between the presence or severity of aortic VC and donor GFR, systolic blood pressure, pulse pressure, calcium–phosphate product or smoking.
Conclusions
AAC prevalence, patterns and severity in this important donor population have not previously been described in the literature. There was relatively little VC in what would be regarded as a “healthy” donor population. VC was more common with age, but the other possible risk factors for the presence or severity of VC did not impact on overall AAC scores. VC did not influence vascular stiffness as represented by pulse pressure. Following the evolution of AAC over time in those who have donated a kidney, and lost some global renal function as a consequence, would be of considerable interest.




Similar content being viewed by others


References
Galliford J, Game DS (2009) Modern renal transplantation: present challenges and future prospects. Postgrad Med J 85(1000):91–101
Hajhosseiny R, Khavandi K, Goldsmith DJ (2013) Cardiovascular disease in chronic kidney disease: untying the Gordian knot. Int J Clin Pract 67(1):14–31
Satyan S, Rocher LL (2004) Impact of kidney transplantation on the progression of cardiovascular disease. Adv Chronic Kidney Dis 11(3):274–293
Matas AJ, Delmonico FL (2012) Living donation: the global perspective. Adv Chronic Kidney Dis 19(4):269–275. doi:10.1053/j.ackd.2012.05.003
Garg AX, Meirambayeva A, Huang A, Kim J, Prasad GV, Knoll G, Boudville N, Lok C, McFarlane P, Karpinski M, Storsley L, Klarenbach S, Lam N, Thomas SM, Dipchand C, Reese P, Doshi M, Gibney E, Taub K, Young A (2012) Donor nephrectomy outcomes research network. Cardiovascular disease in kidney donors: matched cohort study. BMJ 344:e1203. doi:10.1136/bmj.e1203
Chang P, Gill J, Dong J, Rose C, Yan H, Landsberg D, Cole EH, Gill JS (2012) Living donor age and kidney allograft half-life: implications for living donor paired exchange programs. Clin J Am Soc Nephrol 7(5):835–841
Luft FC (2012) Molecular mechanisms of arterial stiffness: new insights. J Am Soc Hypertens 6(6):436–438
Goldsmith D, Ritz E, Covic A (2004) Vascular calcification: a stiff challenge for the nephrologist: does preventing bone disease cause arterial disease? Kidney Int 66(4):1315–1333
Bastos Gonçalves F, Voûte MT, Hoeks SE, Chonchol MB, Boersma EE, Stolker RJ, Verhagen HJ (2012) Calcification of the abdominal aorta as an independent predictor of cardiovascular events: a meta-analysis. Heart 98(13):988–994
Chue CD, Wall NA, Crabtree NJ, Zehnder D, Moody WE, Edwards NC, Steeds RP, Townend JN, Ferro CJ (2012) Aortic calcification and femoral bone density are independently associated with left ventricular mass in patients with chronic kidney disease. PLoS ONE 7(6):e39241
Figueiredo CP, Rajamannan NM, Lopes JB, Caparbo VF, Takayama L, Kuroishi ME, Oliveira IS, Menezes PR, Scazufca M, Bonfá E, Pereira RM (2013) Serum phosphate and hip bone mineral density as additional factors for high vascular calcification scores in a community-dwelling: the São Paulo Ageing & Health Study (SPAH). Bone 52(1):354–359. doi:10.1016/j.bone.2012.10.019
Andrews PA, Burnapp L, Manas D, Bradley JA, Dudley C (2012) British transplantation society; Renal Association. Summary of the British Transplantation Society/Renal Association UK guidelines for living donor kidney transplantation. Transplantation 93(7):666–673
Yashi T, Itoh Y, Gao B, Okada A, Tozawa K, Kohri K (2007) Aortic calcification in urolithiasis patients. Scandinavian J Urol Nephrol 41(5):419–421
Bellasi A, Raggi P (2012) Vascular imaging in chronic kidney disease. Curr Opin Nephrol Hypertens 21(4):382–388
Roy SK, Cespedes A, Li D, Choi TY, Budoff MJ (2011) Mild and moderate pre-dialysis chronic kidney disease is associated with increased coronary artery calcium. Vasc Health Risk Manag 7:719–724
Benetos A, Safar M, Rudnichi A, Smulyan H, Richard JL, Ducimetieère P, Guize L (1997) Pulse pressure: a predictor of long-term cardiovascular mortality in a French male population. Hypertension 30(6):1410–1415
Perlini S, Naditch-Brule L, Farsang C, Zidek W, Kjeldsen SE (2013) Pulse pressure and heart rate in patients with metabolic syndrome across Europe: insights from the GOOD survey. J Hum Hypertens 27(7):412–416. doi:10.1038/jhh.2012.61
Bahous SA, Stephan A, Blacher J, Safar M (2012) Cardiovascular and renal outcome in recipients of kidney grafts from living donors: role of aortic stiffness. Nephrol Dial Transplant 27(5):2095–2100
McEvoy JW, Blaha MJ, Rivera JJ, Budoff MJ, Khan AN, Shaw LJ, Berman DS, Raggi P, Min JK, Rumberger JA, Callister TQ, Blumenthal RS, Nasir K (2012) Mortality rates in smokers and nonsmokers in the presence or absence of coronary artery calcification. JACC Cardiovasc Imaging 5(10):1037–1045
Seyahi N, Kahveci A, Bolayirli M, Akman C, Altiparmak MR, Apaydin S, Ataman R, Sariyar M, Serdengecti K, Erek E (2007) Coronary artery calcification and chronically decreased GFR in living kidney donors. Am J Kidney Dis 49(1):143–152
Lamprea-Montealegre JA, McClelland RL, Astor BC, Matsushita K, Shlipak M, de Boer IH, Szklo M (2013) Chronic kidney disease, plasma lipoproteins, and coronary artery calcium incidence: the Multi-Ethnic Study of Atherosclerosis. Arterioscler Thromb Vasc Biol 33(3):652–658
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Leckstroem, D.C.T., Bhuvanakrishna, T., McGrath, A. et al. Prevalence and predictors of abdominal aortic calcification in healthy living kidney donors. Int Urol Nephrol 46, 63–70 (2014). https://doi.org/10.1007/s11255-013-0485-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-013-0485-0