
Abstract
Purpose
The objective of this systematic review was to describe the prevalence and magnitude of response shift effects, for different response shift methods, populations, study designs, and patient-reported outcome measures (PROM)s.
Methods
A literature search was performed in MEDLINE, PSYCINFO, CINAHL, EMBASE, Social Science Citation Index, and Dissertations & Theses Global to identify longitudinal quantitative studies that examined response shift using PROMs, published before 2021. The magnitude of each response shift effect (effect sizes, R-squared or percentage of respondents with response shift) was ascertained based on reported statistical information or as stated in the manuscript. Prevalence and magnitudes of response shift effects were summarized at two levels of analysis (study and effect levels), for recalibration and reprioritization/reconceptualization separately, and for different response shift methods, and population, study design, and PROM characteristics. Analyses were conducted twice: (a) including all studies and samples, and (b) including only unrelated studies and independent samples.
Results
Of the 150 included studies, 130 (86.7%) detected response shift effects. Of the 4868 effects investigated, 793 (16.3%) revealed response shift. Effect sizes could be determined for 105 (70.0%) of the studies for a total of 1130 effects, of which 537 (47.5%) resulted in detection of response shift. Whereas effect sizes varied widely, most median recalibration effect sizes (Cohen’s d) were between 0.20 and 0.30 and median reprioritization/reconceptualization effect sizes rarely exceeded 0.15, across the characteristics. Similar results were obtained from unrelated studies.
Conclusion
The results draw attention to the need to focus on understanding variability in response shift results: Who experience response shifts, to what extent, and under which circumstances?
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Longitudinal measurements of patient-reported outcomes (PROs) can be affected by response shift. Whereas several definitions of response shift exist [1], they all draw upon the working definition provided by Sprangers and Schwartz in 1999 [2, 3], where response shift refers to a change in the meaning of one’s self-evaluation of a target construct as a result of (a) a change in the respondent’s internal standards of measurement (i.e., recalibration); (b) a change in the importance of component domains constituting the target construct (i.e., reprioritization); or (c) a redefinition of the target construct (i.e., reconceptualization). When response shift occurs, the responses to a PROM at one point in time do not have the same meaning as the responses to that PROM at another point in time (see illustrative vignette in Fig. 1, based on [4]; also see [5]). Response shift has important implications when inferences, actions and decisions in health care are made based on the use of PROMs to measure change in QOL [6]. However, despite a proliferation of research on response shift spanning several decades, a comprehensive descriptive synthesis of quantitative response shift results has thus far not been reported.

Vignette illustrating recalibration, reprioritization, and reconceptualization response shifts
There are many different statistical methods for detecting and quantifying the magnitudes of response shift effects. Informed by our previous work [7,8,9], we a priori classified the methods broadly as follows: design-based methods, latent-variable methods, and regression-based methods (Table 1 for detailed descriptions and explanations). Design-based methods involve collection of data for the specific purpose of detecting response shift effects. Common examples include the then-test and individualized methods. Latent-variable methods allow for testing response shift effects by longitudinally examining the consistency (or invariance) of measurement models (e.g., structural equation models or item response theory or Rasch models). Regression-based methods involve the use of various regression analytical techniques to classify people or test for hypothesized response shift effects. Sébille et al. [8] have shown that all these methods operationalize the working definition of Sprangers and Schwartz [2, 3], albeit in different ways.
Most studies on response shift have focused on response shift detection, and relatively fewer studies have focused on estimating the magnitudes of response shift effects. A previous scoping review by Sajobi et al. [7] on 101 studies using quantitative response shift methods published through 2016 indicated that 96 studies (95%) had detected response shift. Of these studies, 82 (85.4%) detected recalibration response shift, 20 studies (20.8%) detected reprioritization response shift, four studies (4.2%) detected reconceptualization response shift, and seven studies (7.3%) reported a general response shift effect without indicating a particular pathway. A more recent systematic review of 107 studies, also using quantitative methods, which were published between 2010 and 2020 [10] found that only 91 studies (70.5%) had detected response shift. Less than half of the studies (51 studies) overlapped with the former review by Sajobi et al. [7]. Recalibration response shift was found in 73 studies, with 27 (37%) studies using the then-test, 24 (33%) applying structural equation modeling (SEM), and 22 (30%) adopting other methods. In both reviews, reprioritization and reconceptualization response shifts were detected less frequently and if they were, they were predominantly identified by Oort’s SEM method [11, 12].
Previous meta-analyses of response shift effects have focused on estimating the magnitudes of the effects, with results suggesting that effect sizes are relatively small on average. However, the meta-analyses also reveal substantial heterogeneity. A meta-analysis of studies published up to 2005 that used the then-test revealed Cohen’s d effect sizes ranging from 0.08 to 0.32 [13]. A more recent systematic review examined response shift effects in persons with cancer [14]. Seventeen of the 35 studies reported effect sizes of which 12 studies found negligible to small effect sizes, four studies found moderate effect sizes, and one study identified a single effect size of large magnitude. A systematic review on nine studies that examined response shift in people with orthopedic conditions after rehabilitation [15], found effect sizes varying in magnitude although most were small. To date, systematic reviews on the magnitudes of response shift effects included only studies focusing on either a particular response shift method (i.e., the then-test) or a specific patient population (i.e., persons with cancer or an orthopedic condition).
The above reviews reveal considerable heterogeneity in characteristics of response shift studies as they were conducted in different populations, employed different study designs, used different PROMs, and applied different response shift methods. These observations give rise to the question: What is the prevalence (i.e., relative frequency) and magnitude of response shift effects for different response shift methods and across different characteristics of response shift studies? To answer this question, it is important to consider the results from quantitative response shift studies, including results from studies for which effect sizes cannot be obtained. However, a descriptive synthesis of all quantitative response shift results has thus far not been reported.
To address this gap, we conducted a systematic review of all published quantitative studies that investigated response shift using PROMs. Our aim was to describe evidence about response shift results including distributions of response shift prevalence and, where possible, effect sizes, for different response shift methods, and population, study design, and PROM characteristics. We recognize that there continues to be a debate about the conceptualization of response shift in the QOL and health measurement literature. We therefore initiated the Response Shift – in Sync Working Group that aims to synthesize the work on response shift to date [16], including the definitional and theoretical underpinnings of response shift [17], the critical examination of response shift detection methods and their underlying operationalizations of response shift [8], and the implications of response shift for healthcare decision-making based on PROMs [6]. The descriptive systematic review reported herein is part of this initiative. With this review we do not intend to make recommendations of what response shift is or what metrics should be used. Rather, our aim is to describe and synthesize the results of response shift research to date, including the inherent heterogeneity in operationalization. This type of descriptive synthesis is important for identifying gaps, formulating new research questions, designing new longitudinal studies, and guiding future research directions.
Methods
We conducted a systematic review (registered retrospectively in INPLASY at time of data analysis: #202290033) [18] following guidelines by Cooper, Hedge, and Valentine [19] and used the PRISMA statement as a guide for reporting the results [20].
Search strategy and eligibility criteria
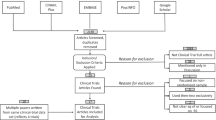
Studies on response shift were identified by searching the following library databases: (a) MEDLINE, PSYCINFO, and CINAHL using the EBSCO interface; (b) EMBASE using the OVID interface; (c) Social Science Citation Index using the Web of Science interface; and (d) Dissertations & Theses Global using the ProQuest interface (see Fig. 2). All searches were conducted using the same combination of the following terms and corresponding abbreviations in all indexed fields: “response shift” OR “longitudinal measurement invariance” OR “retrospective bias” OR “longitudinal differential item” OR “longitudinal DIF.” The searches were limited to English language and a date of publication before January 1, 2021. For the Social Science Citation Index, an additional limit was applied to exclude meeting abstracts. No other filters were applied to any of the searches. Duplicate records were identified and removed using the duplicate screening tool in the EPPI Reviewer Platform [21]. Manuscripts that reported on errata or on the same study as reported in another manuscript were identified as duplicates during the data extraction process after confirming that no additional relevant information could be extracted. We retained the manuscripts that reported the most detailed results.

PRISMA flow diagram. RS response shift, PROM patient-reported outcome measure, HRQOL Health-related quality of life. aReasons are ranked by the first identified reason for exclusion. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. https://doi.org/10.1136/bmj.n71 For more information, visit: http://www.prisma-statement.org/
We aimed to include all longitudinal quantitative studies that examined response shift using a PROM. Exclusion criteria were sequentially applied in the order shown in Fig. 2. The titles and abstracts of each citation were randomly assigned for independent screening by two team members (RS, LR, MEGV, VS, MAGS), all of whom were thoroughly familiar with response shift, using the EPPI Reviewer platform [21]. The full text was subsequently retrieved for each citation identified as potentially relevant and each was screened randomly by two of the same team members. Disagreements were reconciled via consensus.
Data extraction
Data extraction for each included study was completed by one of three team members (LR, MV, RS). Ambiguities were discussed among team members to achieve agreement. Study-level information was extracted using the EPPI reviewer application and detailed information about each response shift effect was extracted and entered into a spreadsheet. The following study-level data extraction characteristics (see Tables 2, 3, 4, 5, 6 for details) were defined in advance and further refined to resolve emerging ambiguities during the data extraction process:
-
1.
Response shift methods: design-based methods, latent-variable methods, regression methods, and study-specific methods (see Table 1 for details).
-
2.
Population characteristics: sex, age, medical condition, and intervention.
-
3.
Study design characteristics: experimental/observational, primary/secondary analysis, sample size, and duration of time between measurement occasions.
-
4.
PROMs characteristics (only including PROMs used for the response shift analysis): name of PROM, type of PROM (generic/disease-specific/individualized/other, where the category individualized PROMs supersedes the categories generic/disease-specific PROMs), and PROM domains.
-
5.
Study results: detection (yes/no) and magnitude (see under statistical analyses) of recalibration, reconceptualization, and reprioritization and dependencies, i.e., whether the response shift effect pertained to a subsample (or group) of an overall sample reported in the same manuscript or the same or overlapping sample from another study.
Statistical analyses
In all studies, authors concluded whether response shift was found or not, although the conclusions may have been based on different grounds, e.g., statistical significance, where different studies adopted different alpha levels or verbal conclusions in the absence of statistical tests. We followed the authors’ conclusions regarding the existence or non-existence of a response shift effect. Where possible, we determined the magnitude of each response shift effect based on reported statistical information from which an effect size could be derived. Table 1 includes a description of response shift detection and effect size calculation (if possible) for each method. We used reported effect sizes, if provided, when insufficient information was available to calculate effect sizes. Standardized mean differences (Cohen’s d) were calculated for the then-test and latent-variable methods based on information reported in each study based on the difference between baseline (\({\overline{X} }_{1})\) and follow-up (then-test) (\({\overline{X} }_{2})\) scores as follows: Cohen’s d = \(\frac{{\overline{X} }_{1}-{\overline{\overline{X}}}_{2}}{\text{SD}}\) (where SD = standard deviation). For some studies, this meant that we first had to transform medians, interquartile ranges (IQR), and t or z statistics into means and standard deviations [19, 22]. We used the following hierarchy to standardize the mean difference, based on (1) the standard deviation of the difference, (2) the pooled standard deviation, or (3) the standard deviation of the baseline measurements (see footnote to Table 1 for details). For SEM, response shift effects were based on parameter estimates of models that adjust for a lack of longitudinal measurement invariance (for more information see [23]). All effect sizes were converted to absolute values. We followed Cohen’s guidelines [24] to interpret effect sizes of 0.2, 0.5, and 0.8 to be small, moderate, and large, respectively. For regression methods that do not use classification of people as having response shift or not, the reported R-squared was used as a measure of effect size, with values of 0.01, 0.06, and 0.14 being indicative of a small, moderate, and large magnitude, respectively [24]. For regression-based response shift methods that do use classification, the proportion of people having undergone response shift was extracted as an indication of the magnitude of effects.
Response shift results and effect sizes were summarized for recalibration and reprioritization or reconceptualization effects at different levels of analysis (study and effect levels). Accordingly, the synthesis focused on describing distributions of prevalence (relative frequency) and magnitude of response shift effects, based on (a) the proportion of studies detecting response shift (study level) and (b) the proportion of response shift effects identified (effect level) for different response shift methods and population, study design, and PROM characteristics. Consistent with our descriptive aim and recognizing the inherent heterogeneity in operationalizations, we used non-parametric statistics to describe the distributions of the effect sizes, including their medians and IQRs for continuous effect sizes and percentages for classification (i.e., we did not pool effect sizes statistically).
Although we sought to describe all response shift effects, we also wanted to account for situations where multiple analyses and studies were done on the same sample. To do so, we first conducted the analyses based on all response shift effects and subsequently repeated the same analyses on the subset of response shift effects from unrelated studies and samples that do not overlap with samples from the same (e.g., subsamples) or other studies (with details reported in Supplementary Tables S1 to S5). Studies were considered related when analyses from different studies are conducted on the same or overlapping samples or when the same results are reported in multiple manuscripts. For related studies, only the first (original) study was counted. Independent samples do not have overlap with other samples. When samples are overlapping, only the overall sample was counted (subsamples were not counted). Analyses were conducted using SPSS [25] with violin plots created using the ggplot2 package in R [26].
Results
Studies
Of the 1906 records screened, 150 studies fulfilled the eligibility criteria and were included (see Fig. 2). Of these studies, 125 were unrelated to any of the other studies and 25 related studies involved analyses of the same or overlapping samples, of which 9 were identified as the primary (first published) studies and 16 as secondary (related studies that were published after the corresponding primary study). We identified a total of 4868 response shift effects (Table 2), of which 917 were from secondary related studies and 284 from primary related studies (3667 effects were from unrelated studies). Results of the 150 studies and 4868 response shift effects are described first, followed by a description of the results based on the 134 unrelated and primary related studies and 3579 response shift effects from independent samples (excluding 372 effects from subsamples), with further details provided in Supplementary Tables S1 to S5.
Response shift methods
Prevalence
Of 150 studies, 130 (86.7%) reported detection of one or more response shift effects (Table 2), based on criteria defined by the authors. However, response shift effects were detected for only 793 (16.3%) of the total 4868 effects investigated. Most response shift results were based on 82 studies that utilized the then-test method, with 86.6% of the studies and 39.2% of 1004 corresponding effects resulting in detection of recalibration response shift. SEM methods were applied in 44 of the studies of which 79.5% resulted in detection of at least one response shift effect. However, only 7.7% of all corresponding 3139 effects revealed response shift, including 16.4% of 986 recalibration effects and 3.7% of 2153 reprioritization or reconceptualization effects.
Other methods were less frequently applied, ranging from 3 to 13 studies. When considering methods that were based on at least 10 studies (i.e., not IRT/Rasch and other study-specific methods), the highest percentage of detected response shift effects at study level was found for individualized methods (100%, 12 studies). At effect level, the percentage of detected response shift effects was also relatively high for individualized methods (74.2%) despite the small number of 31 effects. In general, the prevalence of response shift detection was lower when the number of investigated response shift effects was larger for all response shift pathways.
Magnitude
Effect sizes could be determined for 105 (70.0%) of the studies and a total of 1130 response shift effects, with 96 (91.4%) of these studies resulting in detection of 537 (47.5%) response shift effects. Cohen’s d (standardized mean difference) was the most common effect size metric, which was obtained for 1062 effects from 91 studies (see Table 3). Most of these effect sizes were based on studies using the then-test (72 studies and 929 effects), resulting in an overall median effect size of 0.22 with substantial dispersion (IQR 0.10–0.38) for recalibration effects. Cohen’s d effect sizes were also determined for 111 effects from 19 studies using SEM, where response shift was detected for all of these studies and 95.5% of the effects, with median effect sizes of 0.22 (IQR 0.14–0.35) for recalibration and 0.10 (IQR 0.00–0.14) for reprioritization or reconceptualization. Other methods enabling the calculation of Cohen’s d effect sizes included other design-based methods (3 studies and 15 effects) and individualized methods (1 study and 7 effects) (see Table 3). The distribution of effect sizes across these methods is visualized as violin plots in Fig. 3. Additionally, two studies (27 effects) provided the R-squared statistic as an effect size for regression methods without classification, resulting in a median effect size of 0.01 (IQR 0.00–0.02) for reprioritization/reconceptualization. Response shift effect sizes could also be obtained for 27 effects from 17 studies using classification methods, of which all resulted in detection of response shifts. The greatest effect size was obtained for the design-based individualized classification method, which also had the largest number of effects (13), resulting in 68.2% of the pooled sample size indicating reprioritization/reconceptualization response shift. Finally, three studies (14 effects) reported study-specific effect size metrics (see Table 3).

Distribution of absolute effect sizes across types of response shift methods. Note All violin plots have the same area, which is determined by the distribution of effects within each method. Four effect sizes for which the response shift pathway is unknown are excluded. Two extreme effect sizes of 6.9 [63] and 2.9 [64] for the then-test are not shown to ensure other distributions remain discernable (instead of becoming flat lines). The outliers were only removed for this visualization, they were included in the statistical analysis
Study population characteristics
Prevalence
At study level, most studies involved participants with mixed sex (121 studies), who were mostly adults (100 studies), with a medical condition (141 studies), and/or undergoing a medical intervention (69 studies) (Table 4). The study-level prevalence of detected response shift ranged from 66.7% (only male; 12 studies) to 90.0% (medical condition: stroke; 11 studies), when excluding population characteristics with fewer than 10 studies. The corresponding effect-level prevalence values were much lower and ranged from 5.9% (mental health condition; 472 effects) to 32.9% (other/unspecified intervention; 149 effects) for population characteristics with minimally 100 effects.
Magnitude
When considering population characteristics for which at least 100 effects sizes could be determined, median recalibration effect sizes ranged from 0.17 (IQR 0.09–0.28) (381 effects for female samples) to 0.31 (IQR 0.22–0.42) (101 effects for male samples). The reprioritization or reconceptualization effect sizes are based on fewer effects (ranging from 2 to 30 per population characteristic), with median effect sizes ranging from 0.03 (IQR 0.00–0.11), based on 17 effects from samples with medical interventions, to 0.20 (IQR 0.10–0.39) for 8 effects from samples with other/unspecified interventions.
Study design characteristics
Prevalence
Most studies employed an observational design (122 studies), conducted primary analysis (90 studies), had a sample size between 57 and 254 (79 studies), and employed an observation period greater than 12 months (90 studies). Across the four study design characteristics, the study-level prevalence of detected response shift ranged from 72.2% (time period from 6 to 12 months) to 91.3% (time period from 1 to 6 months) (excluding the one study with unknown data analysis) (Table 5). Again, the corresponding effect-level prevalence values were lower and ranged from 8.4% (1132 effects for sample size > 411) to 30.2% (1590 effects for primary analysis).
Magnitude
When considering study design characteristics with at least 100 effect sizes, the smallest median recalibration effects (Cohen’s d effect sizes) was 0.15 (IQR 0.09–0.24) based on 194 effects from studies with sample sizes between 255 and 410. The largest median effect size was 0.26 (IQR 0.16–0.41) based on 145 effects from studies adopting an experimental design and 0.26 (IQR 0.13–0.45) based on 391 effects for studies with sample sizes less than 57. The reprioritization or reconceptualization effect sizes are based on fewer effects (ranging from 4 to 33 per study design characteristic), with median effect sizes ranging from 0.01 (for 7 effects from studies employing a time frame of < 1 month) to 0.14 (based on 15 effects from studies conducting primary analysis and 13 effects of studies using a sample size between 57 and 254) (excluding the time period classification “not reported,” since this is essentially a missing data category).
PROM characteristics
Prevalence
With respect to PROM type, most studies employed a generic PROM (76 studies) with the SF family of PROMs (47 studies) and the EQ-5D (14 studies) being most prevalent (Table 6). Disease-specific PROMs were used in 57 studies, with the EORTC measures being used most often (17 studies). Of the PROM domains, physical (96 studies), general health/QOL (95 studies), and psychological other than depression (85 studies) domains were measured most frequently. When excluding PROM types used in 10 or less studies, study-level prevalence of detected response shift for PROM types ranged from 69.6% (46 studies using other types of PROMs) to 90.0% (10 studies using individualized PROMs). Regarding the different PROM domains, study-level prevalence was within a range of 12 percentage points for the major domains, ranging from 56.7% for ‘other’ domain to 70.8% for the physical domain (excluding those with 10 or less studies).
When considering PROM types with at least 100 effect sizes, the effect-level prevalence of detected response shift for PROM types ranged from 10.5 (611 effects for ‘other’ generic PROMS) to 25.2% (616 effects generated by studies employing EORTC measures). The corresponding effect-level prevalence values for the PROM domains (excluding those with less than 100 effects) ranged from 10.5% for other PROM domains (440 effects) to 28% for both general health/QOL and pain (561 and 236 effects, respectively).
Magnitude
When considering PROM types with at least 100 effect sizes, median recalibration effect sizes (Cohen’s d) ranged from 0.17 (IQR 0.09–0.28) for 315 effects from studies using the EORTC PROMs to 0.29 (IQR 0.12–0.48) for 115 effects based on studies using ‘other’ disease-specific PROMs. Median reprioritization/reconceptualization effect sizes ranged from 0.07 (IQR 0.03–0.14) based on 16 effects for other types of PROMs to 0.17 (IQR 0.09–0.47) based on 4 effects for the EORTC family. For PROM domains, median recalibration effects based on at least 100 effects, ranged from 0.20 (IQR 0.10–0.35) based on 429 effects for the physical domain to 0.23 (IQR 0.09–0.41) based on 182 effects for general health/QOL and 0.23 (IQR 0.11–0.33) for 199 effects for the psychological domain other than depression. The reprioritization or reconceptualization effect sizes are based on fewer effects (ranging from 2 (‘other’ PROM domain) to 18 (SF family) across all PROM characteristics), with median effect sizes ranging from 0.05 (IQR 0.00–0.09) based on 2 effects for the PROM domain other to 0.17 (IQR 0.19 – 0.47) based on 4 effects for the EORTC PROMs.
Unrelated studies and non-overlapping samples
Prevalence and effect size estimates were similar for most methods and population, study design, and PROM characteristics when only unrelated studies and non-overlapping samples were considered (see Table S1–S5). Study-level differences in prevalence ranged from 0.0 to 5.9% (when considering methods and characteristics with at least 10 studies) for most methods and characteristics, with the exception of the characteristics ‘only males’ or a ‘sample size of 255–410,’ which had greater % prevalence when considering only independent effects. Effect-level differences in prevalence ranged from 0.0 to 14.9%, with 15 of the effect-level differences exceeding 5% (when considering methods and characteristics with at least 100 effects). The median difference in Cohen’s d estimates of recalibration response shift is 0.02 (when considering methods and characteristics with at least 100 effects), with the largest differences for effects for the characteristics ‘unknown sex’ and a ‘mental health condition.’ For reprioritization/recalibration, the number of effects was too small to warrant meaningful comparisons.
Discussion
To further find the field of response shift research, this study described variation in prevalence of response shift results and where possible, magnitude of response shift effects for quantitative studies using PROM data. Consistent with earlier reviews [7, 10], the most frequently applied response shift method was the then-test, followed by SEM, other design-based methods, regression methods without classification, individualized methods, regression methods with classification, IRT/Rasch, and other study-specific methods. Most studies reported detection of one or more response shift effects. However, response shift effects were detected for only a sixth of all effects investigated. Clearly study-level prevalence is expected to be higher than effect-level prevalence because a study was classified as having detected response shift when response shift was detected for any of the multiple effects being studied. However, it is noteworthy that the prevalence distributions at the study level as compared to the effect-level were also different across the different methods, population, study design, and PROM characteristics, i.e., different methods and characteristics would be identified as having higher or lower prevalence of response shift effects when this is determined at the study as compared to the effect-level. Individual studies and previous reviews primarily focused on study-level results, drawing binary conclusions about whether response shift is present or not. Our results show that such a one-sided focus may be misleading, and only the combined information at study and effect level provides a comprehensive overview of response shift results.
Effect sizes were determined for 105 of the 150 studies. Whereas, the median effect sizes varied per method, population, study design, and PROM characteristic, they were all of a small magnitude, with most recalibration effect sizes between 0.20 and 0.30 and reprioritization/reconceptualization effect sizes rarely exceeding 0.15. There may be methodological explanations for the small effect sizes found. One explanation would be the presence of heterogeneous samples where response shifts may occur at the individual level but in different directions that cancel each other out at the group level. Nonetheless, given the small median effect sizes, we need to acknowledge that there are empirical situations where the impact of response shift may be quite small, or even negligible, when we are only interested in results for the entire group. But even in such contexts, there is reason to consider such effect sizes as relevant. Many effects in PROM research have a comparable magnitude. For example, a systematic review aimed to investigate, among other things, whether patients who share their responses to PROMs with their health care provider have better health. The results indicated small effect sizes for such PROMs feedback on patient-reported health outcomes [27]. This review illustrates that the target signal (in this case PROMs feedback) may not be substantially different in magnitude than other processes triggered using PROMs, such as response shift.
The most striking finding is that the effect sizes varied widely, ranging from zero to large, both within and between studies. This observation draws attention to the importance of considering the dispersion of response shift effects within studies rather than relying exclusively on within-study pooled results. The large variability in effect size estimates may also have methodological explanations, including variability in response shift methods (e.g., SEM methods lead to smaller effect sizes than then-tests), study populations, sample sizes, and PROMs. The proportion of variability in effect sizes attributable to such study characteristics is currently unknown. When part of the variability in effect sizes would indeed be caused by differences between study populations, then substantial effects may be experienced by some groups or individuals or in specific contexts or with certain PROMs. Ignoring such variability would not pay credit to the experiences of the respondents and the richness of the data. In other words, variability can be highly meaningful. A parallel can be drawn with precision medicine, e.g., in cancer treatment. Whereas some treatments may hardly affect the survival of a particular population, further investigation into the variability of effects may reveal that the treatment can be highly effective in a subgroup of patients whose tumor DNA matches the working mechanisms of those treatments. Hence, information about the variability of treatment effects enables the development of targeted therapy, which ultimately results in more life years gained. Whereas research into response shift will not lead to such dramatic gains, we may need to be moving into ‘precision methodology’ for response shift. The key message is that, rather than focusing on effect sizes for the entire group, we should focus on describing and understanding variability in effects: in terms of identification (who experience response shift?), magnitude (to what extent?), and under which circumstances. Moreover, arguments around social justice and societal inequalities would require such subgroup analyses investigating whether response shift effects systematically favor or disadvantage some groups of people [6, 28].
A number of limitations of this systematic review merit attention. We omitted studies that were not reported in English. We also cannot preclude the possibility that we may have missed relevant papers despite our extensive literature search. The synthesis of included studies was challenged due to different operationalizations of response shift and inadequate reporting of study results and/or methodology. A substantial number of studies required a disproportionate amount of effort from the team to ensure consensus about the extracted data or considering information as missing. Moreover, dependencies in the data arose from multiple studies (often secondary analyses) being conducted on the same or overlapping samples. We therefore repeated the analyses on independent data only. Further, we cannot be certain that our classifications of study populations, designs, and PROMs represent the best characteristics to highlight heterogeneity. A more important caveat is related to a recent review of response shift methods [8], which concluded that for each response shift method extra steps need to be taken to ensure that the results can indeed be qualified as response shift, i.e., the effects need to be caused by change in meaning of the self-report (see also Vanier et al. [17] and Sprangers et al. [29]). In the present study, we considered all detected effects as response shift effects, although their substantiation may be questioned. However, this limitation is inherent to the current stage of response shift research rather than this systematic review. Further, the heterogeneity of the results may, in part, be due to the variety of detection methods. However, this systematic review cannot disentangle the heterogeneity induced by variation of methods, study context, and design. Another limitation is that the use of different methods and metrics may preclude a clear view of how the resulting numbers compare. We therefore have provided a table where each method is described, response shift detection is detailed, the two most prevalent methods (then-test and Oort’s SEM approach) are further explained, and the effect size metric for all applicable methods are provided (see Table 1). We would like to add that we provided an overview of the various methods and metrics as intended and did not aim to solve the inherent heterogeneity of response shift research. We acknowledge the plea for conceptual and operational clarity of what response shift is, but this is beyond the scope of this systematic review. We also would like to highlight that such a plea is not limited to response shift, but equally applicable to the quality-of-life research field at large and for that matter also to other behavioral and social science research [30]. Further, we did not perform an assessment of methodological quality of individual studies. The heterogeneity of the included studies with regard to response shift methods, population characteristics, study design, and PROMs used precludes such an unambiguous assessment. For example, sample size does not apply as a quality criterion to individual methods. Rather than weighing different study aspects as an indication of study quality, we made them the focus of our main analyses, by describing the prevalence and, where possible, the magnitude of response shift effects for each response shift method, population, study designs, and PROM characteristic. Finally, whereas this descriptive review provides insight into how response shift effects and effect sizes vary per characteristic, it does not allow for direct comparison of effects across characteristics, however, tempting. Studies examining the same characteristic may differ in many other relevant aspects. For example, the number of response shift parameters in a SEM model is a multitude of those of other methods (e.g., the then-test). Moreover, latent-variable methods can only detect response shift when it affects a minority of items and a majority of study participants [31]. Hence, the percentage of detected response shift effects is generally lower and not directly comparable to other methods. Moreover, response shift effects or effect sizes are based on different numbers of studies. Generally, more extreme numbers were found for methods and characteristics based on fewer studies or response shift effects. We therefore only described the results of recalibration response shift when they were based on at least 10 studies and 100 effects. This arbitrary cut-off was intended to guard against over-interpretation of the results. In the case of reprioritization and reconceptualization response shift, the small number of effects reported precluded the application of such criteria. We also refrained from using qualifiers as a higher or lower prevalence and magnitude of response shift effects and provided the minimum and maximum numbers instead.
The current descriptive review on results of quantitative response shift studies is the most comprehensive to date. The data provide insight into the heterogeneity of response shift results, i.e., how the number and magnitude of response shift effects differ across studies employing different response shift methods, populations, research designs, and PROMs. In this sense, this paper draws attention to what some scholars may find a foundational issue in response shift research—the longstanding challenge to harmonize different metrics of response shift across the various measurement procedures from which it is derived. But even in the absence of such harmonization, insight into response shift effects and effect sizes can inform future planning of longitudinal PROM studies, guide the selection of the requisite PROM(s), provide important information for analyzing PROM data in diverse populations, and most importantly, will identify those respondents susceptible to response shift effects for whom different healthcare decision may need to be made.
Data availability
A data file including all data reported in this manuscript can be obtained by contacting the corresponding author.
Code availability
Not applicable.
References
Rapkin, B. D., & Schwartz, C. E. (2004). Toward a theoretical model of quality-of-life appraisal: Implications of findings from studies of response shift. Health and Quality of Life Outcomes, 2, 14.
Sprangers, M. A., Cull, A., Bjordal, K., Groenvold, M., & Aaronson, N. K. (1993). The European organization for research and treatment of cancer. approach to quality of life assessment: Guidelines for developing questionnaire modules. Eortc Study Group on Quality of Life. Quality of Life Research, 2(4), 287–295.
Schwartz, C. E., & Sprangers, M. A. (1999). Methodological approaches for assessing response shift in longitudinal health-related quality-of-life research. Social Science & Medicine, 48(11), 1531–1548.
Oort, F. J., Visser, M. R., & Sprangers, M. A. (2009). Formal definitions of measurement bias and explanation bias clarify measurement and conceptual perspectives on response shift. Journal of Clinical Epidemiology, 62(11), 1126–1137.
Kwon, J.-Y., Russell, L., Coles, T., Klaassen, R. J., Schick-Makaroff, K., Sibley, K. M., Mitchell, S. A., & Sawatzky, R. (2022). Patient-reported outcomes measurement in radiation oncology: Interpretation of individual scores and change over time in clinical practice. Current Oncology, 29(5), 3093–3103.
Sawatzky, R., Kwon, J. Y., Barclay, R., Chauhan, C., Frank, L., Van Den Hout, W. B., Nielsen, L. K., Nolte, S., & Sprangers, M. A. G. (2021). Implications of response shift for micro-, meso-, and macro-level healthcare decision-making using results of patient-reported outcome measures. Quality of Life Research, 30(12), 3343–3357.
Sajobi, T. T., Brahmbatt, R., Lix, L. M., Zumbo, B. D., & Sawatzky, R. (2018). Scoping review of response shift methods: Current reporting practices and recommendations. Quality of Life Research, 27(5), 1133–1146.
Sébille, V., Lix, L. M., Ayilara, O. F., Sajobi, T. T., Janssens, A. C. J. W., Sawatzky, R., Sprangers, M. A. G., & Verdam, M. G. E. (2021). Critical examination of current response shift methods and proposal for advancing new methods. Quality of Life Research, 30(12), 3325–3342.
Sawatzky, R., Sajobi, T. T., Brahmbhatt, R., Chan, E. K., Lix, L., & Zumbo, B. D. (2017). Longitudinal change in response processes: A response shift perspective. In B. D. Zumbo & A. M. Hubley (Eds.), Understanding and investigating response processes in validation research (pp. 251–276). New York: Springer.
Ortega-Gomez, E., Vicente-Galindo, P., Martin-Rodero, H., & Galindo-Villardon, P. (2022). Detection of response shift in health-related quality of life studies: A systematic review. Health and Quality of Life Outcomes, 20(1), 20.
Oort, F. J. (2005). Using structural equation modeling to detect response shifts and true change. Quality of Life Research, 14(3), 587–598.
Oort, F. J., Visser, M. R., & Sprangers, M. A. (2005). An application of structural equation modeling to detect response shifts and true change in quality of life data from cancer patients undergoing invasive surgery. Quality of Life Research, 14(3), 599–609.
Schwartz, C. E., Bode, R., Repucci, N., Becker, J., Sprangers, M. A., & Fayers, P. M. (2006). The clinical significance of adaptation to changing health: A meta-analysis of response shift. Quality of Life Research, 15(9), 1533–1550.
Ilie, G., Bradfield, J., Moodie, L., Lawen, T., Ilie, A., Lawen, Z., Blackman, C., Gainer, R., & Rutledge, R. D. H. (2019). The role of response-shift in studies assessing quality of life outcomes among cancer patients: A systematic review. Frontiers in Oncology, 9, 783–783.
Powden, C. J., Hoch, M. C., & Hoch, J. M. (2018). Examination of response shift after rehabilitation for orthopedic conditions: A systematic review. Journal of Sport Rehabilitation, 27(5), 469–479.
Sprangers, M. A. G., Sajobi, T., Vanier, A., Mayo, N. E., Sawatzky, R., Lix, L. M., Oort, F. J., & Sebille, V. (2021). Response shift in results of patient-reported outcome measures: A commentary to the response shift-in sync working group initiative. Quality of Life Research, 30, 3299–3308.
Vanier, A., Oort, F. J., Mcclimans, L., Ow, N., Gulek, B. G., Böhnke, J. R., Sprangers, M., Sébille, V., & Mayo, N. (2021). Response shift in patient-reported outcomes: Definition, theory, and a revised model. Quality of Life Research, 30(12), 3309–3322.
Sawatzky, R., Sajobi Tolulope, T., Russell, L., Awasoga, A. O., Ademola, A., Bohnke, J. R., Lawal, O., Brobbey, A., Lix, L. M., Anota, A., Sebille, V., Sprangers Mirjam, A. G., & Verdam Mathilde, G. E. (2022). A synthesis of response shift effects in quantitative health research: A systematic review and meta-regression protocol. Inplasy Protocol 202290033. https://Inplasy.com/Inplasy-2022-9-0033/
Cooper, H., Hedges, L. V., & Valentine, J. C. (2019). The handbook of research synthesis and meta-analysis. Russell Sage Foundation.
Page, M. J., Moher, D., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hrobjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., Mcdonald, S., … Mckenzie, J. E. (2021). Prisma 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ, 372, N160.
Thomas, J., Graziosi, G., Brunton, J., Ghouze, Z., Odriscoll, P., Bond, M. H., & Koryakina, A. (2022). Eppi-reviewer: Advanced software for systematic reviews, maps and evidence synthesis. Eppi-Centre, Ucl Social Research Institute, University College London.
Wan, X., Wang, W., Liu, J., & Tong, T. (2014). Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Medical Research Methodology, 14, 135.
Verdam, M. G. E., Oort, F. J., & Sprangers, M. A. G. (2017). structural equation modeling-based effect-size indices were used to evaluate and interpret the impact of response shift effects. Journal of Clinical Epidemiology, 85, 37–44.
Cohen, J. (1992). A power primer. Psychological Bulletin, 112(1), 155–159.
Ibm Corp. (2021). Ibm Spss statistics for windows, Version 28.0. Ibm Corp.
Wickham, H. (2016). Ggplot2: Elegant graphics for data analysis. https://Ggplot2.Tidyverse.org/
Gibbons, C., Porter, I., Gonçalves-Bradley, D. C., Stoilov, S., Ricci-Cabello, I., Tsangaris, E., Gangannagaripalli, J., Davey, A., Gibbons, E. J., Kotzeva, A., et al. (2021). Routine provision of feedback from patient-reported outcome measurements to healthcare providers and patients in clinical practice. Cochrane Database of Systematic Reviews. https://doi.org/10.1002/14651858.CD011589.pub2
Hartog, I. D., Willems, D. L., Van Den Hout, W. B., Scherer-Rath, M., Oreel, T. H., Henriques, J. P. S., Nieuwkerk, P. T., Van Laarhoven, H. W. M., & Sprangers, M. A. G. (2019). Influence of response shift and disposition on patient-reported outcomes may lead to suboptimal medical decisions: A medical ethics perspective. BMC Medical Ethics, 20(1), 61.
Sprangers, M. A. G., Sawatzky, R., Vanier, A., Bohnke, J. R., Sajobi, T., Mayo, N. E., Lix, L. M., Verdam, M. G. E., Oort, F. J., & Sebille, V. (2023). Implications of the syntheses on definition, theory, and methods conducted by the Response Shift - In Sync Working Group. Quality of Life Research, 32, 2165–2178.
Reeve, B. B. (2010). An opportunity to refine our understanding of “response shift” and to educate researchers on designing quality research studies: Response to Ubel, Peeters, And Smith. Quality of Life Research, 19(4), 473–475.
Oort, F. J. (2005). Towards a formal definition of response shift (In Reply To G.W. Donaldson). Quality of Life Research, 14(10), 2353–2355.
Howard George, S., & Dailey Patrick, R. (1979). Response-shift bias: A source of contamination of self-report measures. Journal of Applied Psychology, 64, 144–150.
Edelaar-Peeters, Y., & Stiggelbout, A. M. (2013). Anticipated adaptation or scale recalibration? Health and Quality of Life Outcomes, 11, 171.
Ring, L., Hofer, S., Heuston, F., Harris, D., & O’boyle, C. A. (2005). Response shift masks the treatment impact on patient reported outcomes (Pros): The example of individual quality of life in edentulous patients. Health and Quality of Life Outcomes, 3, 55.
Dempster, M., Carney, R., & Mcclements, R. (2010). Response shift in the assessment of quality of life among people attending cardiac rehabilitation. British Journal of Health Psychology, 15(2), 307–319.
Echteld, M. A., Deliens, L., Ooms, M. E., Ribbe, M. W., & Van Der Wal, G. (2005). Quality of life change and response shift in patients admitted to palliative care units: A pilot study. Palliative Medicine, 19(5), 381–388.
Höfer, S., Pfaffenberger, N., Renn, D., Platter, M., & Ring, L. (2010). Coronary intervention improves disease specific health-related quality of life but not individualised quality of life: A potential response shift effect? Applied Research in Quality of Life, 6(1), 81–90.
Echteld, M. A., Van Zuylen, L., Bannink, M., Witkamp, E., & Van Der Rijt, C. C. D. (2007). Changes in and correlates of individual quality of life in advanced cancer patients admitted to an academic unit for palliative care. Palliative Medicine, 21(3), 199–205.
Sharpe, L., Butow, P., Smith, C., Mcconnell, D., & Clarke, S. (2005). Changes in quality of life in patients with advanced cancer: Evidence of response shift and response restriction. Journal of Psychosomatic Research, 58(6), 497–504.
Aburub, A. S., Gagnon, B., Ahmed, S., Rodríguez, A. M., & Mayo, N. E. (2018). Impact of reconceptualization response shift on rating of quality of life over time among people with advanced cancer. Supportive Care in Cancer, 26(9), 3063–3071.
Ahmed, S., Mayo, N. E., Wood-Dauphinee, S., Hanley, J. A., & Cohen, S. R. (2005). Using the patient generated index to evaluate response shift post-stroke. Quality of Life Research, 14(10), 2247–2257.
Tavernier, S. S., Beck, S. L., Clayton, M. F., Pett, M. A., & Berry, D. L. (2011). Validity of the patient generated index as a quality-of-life measure in radiation oncology. Oncology Nursing Forum, 38(3), 319–329.
Ahmed, S., Mayo Nancy, E., Wood-Dauphinee, S., Hanley James, A., & Cohen, S. R. (2005). The structural equation modeling technique did not show a response shift, contrary to the results of the then test and the individualized approaches. Journal of Clinical Epidemiology, 58(11), 1125–1133.
Machuca, C., Vettore, M. V., & Robinson, P. G. (2020). How peoples’ ratings of dental implant treatment change over time? Quality of Life Research, 29(5), 1323–1334.
Visser, M. R., Oort, F. J., & Sprangers, M. A. (2005). Methods to detect response shift in quality of life data: A convergent validity study. Quality of Life Research, 14(3), 629–639.
Dabakuyo, T. S., Guillemin, F., Conroy, T., Velten, M., Jolly, D., Mercier, M., Causeret, S., Cuisenier, J., Graesslin, O., Gauthier, M., & Bonnetain, F. (2013). Response shift effects on measuring post-operative quality of life among breast cancer patients: A multicenter cohort study. Quality of Life Research, 22(1), 1–11.
Rapkin, B. D., Garcia, I., Michael, W., Zhang, J., & Schwartz, C. E. (2017). Distinguishing appraisal and personality influences on quality of life in chronic illness: Introducing the quality-of-life appraisal profile version 2. Quality of Life Research, 26(10), 2815–2829.
Jansen, S. J., Stiggelbout, A. M., Nooij, M. A., Noordijk, E. M., & Kievit, J. (2000). Response shift in quality of life measurement in early-stage breast cancer patients undergoing radiotherapy. Quality of Life Research, 9(6), 603–615.
Abolhassani, N., Santos-Eggimann, B., Bula, C., Goy, R., Guessous, I., & Henchoz, Y. (2019). Temporal changes in importance of quality of life domains: A longitudinal study in community-dwelling Swiss older people. Quality of Life Research, 28(2), 421–428.
Hinz, A., Karoff, J., Kittel, J., Brähler, E., Zenger, M., Schmalbach, B., & Kocalevent, R.-D. (2020). Associations between self-rated health and the assessments of anchoring vignettes in cardiovascular patients. International Journal of Clinical and Health Psychology, 20(2), 100–107.
Preiss, M., Friedrich, M., Stolzenburg, J. U., Zenger, M., & Hinz, A. (2019). Response shift effects in the assessment of urologic cancer patients’ quality of life. European Journal of Cancer Care (England), 28(4), E13027.
Anota, A., Bascoul-Mollevi, C., Conroy, T., Guillemin, F., Velten, M., Jolly, D., Mercier, M., Causeret, S., Cuisenier, J., Graesslin, O., Hamidou, Z., & Bonnetain, F. (2014). Item response theory and factor analysis as a mean to characterize occurrence of response shift in a longitudinal quality of life study in breast cancer patients. Health and Quality of Life Outcomes, 12, 32.
Schwartz, C. E., Feinberg, R. G., Jilinskaia, E., & Applegate, J. C. (1999). An evaluation of a psychosocial intervention for survivors of childhood cancer: Paradoxical effects of response shift over time. Psycho-Oncology, 8(4), 344–354.
Schwartz, C., Sprangers, M. A., Carey, A., & Reed, G. (2004). Exploring response shift in longitudinal data. Psychology & Health, 19(1), 51–69.
Chen, P. Y., & Yang, C. M. (2020). Consequences of ignoring the response-shift and measure non-invariant items in sleep studies: An empirical data based simulation of the treatment effect of Cbt-I on dysfunctional sleep beliefs. Sleep Medicine, 74, 99–108.
Chen, P. Y., Jan, Y. W., & Yang, C. M. (2017). Are the insomnia severity index and Pittsburgh sleep quality index valid outcome measures for cognitive behavioral therapy for insomnia? Inquiry from the perspective of response shifts and longitudinal measurement invariance in their Chinese versions. Sleep Medicine, 35, 35–40.
De Beurs, D. P., Fokkema, M., De Groot, M. H., De Keijser, J., & Kerkhof, A. J. (2015). Longitudinal measurement invariance of the beck scale for suicide ideation. Psychiatry Research, 225(3), 368–373.
Mayo, N. E., Scott, S. C., & Ahmed, S. (2009). Case management poststroke did not induce response shift: The value of residuals. Journal of Clinical Epidemiology, 62(11), 1148–1156.
Murray, A. L., Mckenzie, K., Murray, K., & Richelieu, M. (2020). Examining response shifts in the clinical outcomes in routine evaluation-outcome measure (Core-Om). British Journal of Guidance & Counselling, 48(2), 276–288.
Smith, D., Woodman, R., Harvey, P., & Battersby, M. (2016). Self-perceived distress and impairment in problem gamblers: A study of pre- to post-treatment measurement invariance. Journal of Gambling Studies, 32(4), 1065–1078.
Rapkin, B. D. (2000). Personal goals and response shifts: understanding the impact of illness and events on the quality of life of people living with aids. In Adaptation to changing health: Response shift in quality-of-life research (pp. 53–71). American Psychological Association.
Schwartz, C. E., Stucky, B. D., Michael, W., & Rapkin, B. D. (2020). Does Response shift impact interpretation of change even among scales developed using item response theory? Journal of Patient-Reported Outcomes, 4(1), 8.
Zhang, X.-H., Li, S.-C., Xie, F., Lo, N.-N., Yang, K.-Y., Yeo, S.-J., Fong, K.-Y., & Thumboo, J. (2012). An exploratory study of response shift in health-related quality of life and utility assessment among patients with osteoarthritis undergoing total knee replacement surgery in a tertiary hospital in Singapore. Value in Health, 15(1), S72–S78.
Bastianelli, A., Gius, E., & Cipolletta, S. (2016). Changes over time in the quality of life, prolonged grief and family strain of family caregivers of patients in vegetative state: A pilot study. Journal of Health Psychology, 21(5), 844–852.
Funding
Open access funding provided by University of Gothenburg. This research was undertaking, in part, thanks to funding from the Canada Research Chairs (CRC) program supporting Dr. Sawatzky’s CRC in Person-Centered Outcomes. Canada Research Chairs, CRC-2017-00268, Richard Sawatzky
Author information
Authors and Affiliations
Consortia
Contributions
TS led preliminary conception and analyses with OAA and OL, with the support of OL, AB, and AA, which were used to inform the development of the protocol. RS led the current project, including data extraction, conducted the analyses, and wrote the first outlines and all drafts of the paper together with MS. RS, LR, MGEV, VS, and MS screened the articles and RS, LR, and MGEV conducted data extraction. Outstanding issues were discussed and resolved with VS and MAGS. VS, MGEV, MAGS, TS, OOA, MGEV, LR, VS, MAGS, LL, and JB contributed to the data interpretation and commented to and edited the first iterations of the paper. All co-authors and the remaining members of the Response Shift – in Sync Working Group commented to and edited the semi-final draft. They all approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest that are relevant to the content of this article. JRB is Co-Editor in Chief of Quality of Life Research.
Research involving human participants and/or animals
Not applicable.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Consent to participate
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sawatzky, R., Sajobi, T.T., Russell, L. et al. Response shift results of quantitative research using patient-reported outcome measures: a descriptive systematic review. Qual Life Res 33, 293–315 (2024). https://doi.org/10.1007/s11136-023-03495-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-023-03495-x