
Abstract
Peer telemental health recently became Medicaid reimbursable during the COVID-19 crisis, increasing the need for standardized training on digital peer support (DPS) services. DPS has the potential to reduce barriers to services and expand the reach of peer support specialists. The 4-h Digital Peer Support Training program was developed to train peer support specialists for rapid uptake in providing digital peer support during the COVID-19 crisis. The purpose of this study was to examine the impact of the 4-h DPS course for peer support specialists. Surveys were administered to examine pre-post changes in DPS course for participants (N = 75) related to attitudes/ beliefs towards DPS, ability to use/ engage in DPS, and organizational readiness to implement DPS. Data were analyzed by conducting paired samples t-tests. Linear mixed models were used to explore significant results further. Statistically significant (< .05) changes were observed related to readiness to use DPS, attitudes/ beliefs towards DPS, and ability to use/ engage in DPS. The 4-h DPS course may be beneficial in providing diverse groups of peer support specialists with a standardized training framework. Widespread dissemination of the DPS short course may be beneficial in rapidly equipping peer support specialists with the skills and resources needed to expand the reach of peer support services during the COVID-19 crisis and beyond.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Digital peer support can expand the reach of peer support services through the use of technology (i.e., smartphones, videoconferences, text messages) and augment clinical mental health services provided by psychiatrists and other licensed clinicians [1,2,3]. Digital peer support is defined as live or automated peer support services delivered through any technology medium [4]. The COVID-19 pandemic has facilitated the expansion of digital peer support to include not only videoconferencing, but also videogames and virtual reality peer support delivery [5]. As digital peer support continues to expand across the world, peer support specialists have increasingly reported the desire and need to use technology to deliver peer support [5]. Peer support is defined as shared knowledge, experience, emotional, social, and/or practical assistance to support others with similar lived experiences [6], and includes evidence-based peer-supported self-management services [4]. Mental health peer support provides support services to maintain recovery between clinical visits [6], and the WHO has classified peer support as an essential element of recovery [7]. Currently, digital peer support is Medicaid reimbursable due to the ongoing emergency declaration regarding the COVID-19 crisis allowing for providers (including peer support specialists) to offer telehealth services. A cross-sectional online survey of 488 peer support specialists from 42 different states found that 50% of peer support specialists reported offering digital peer support [5]. Despite the widescale use of digital peer support, a standardized training is greatly needed to guarantee quality services.
A three-month long Digital Peer Support Certification has been developed that focuses on increasing the performance of peer support specialists’ ability to use smartphones in their practice [8]. This Certification, highlighted in the Substance Abuse for Mental Health Administration’s Mental Health Peer Support Workforce Designline (2021), 16-h of in-person training and ongoing education and simulation training over a period of three-months [9]. Training includes technological literacy and skills, including how to download smartphone apps, how to send text messages, and how to watch videos [8]. This Certification also addresses organizational challenges such as access to technologies, HIPAA-compliance and confidentiality issues, work-life balance, and the importance of digital crisis intervention (e.g., how to respond to a social media message outside of work hours that states a client wants to harm themselves or others). This certification has shown to be an effective knowledge translation in that peer support specialists increased their actual capacity to use technology [8]. While the Digital Peer Support Certification is promising, the focus is service delivery through smartphone technologies–-not the broad array of technologies used by peer support specialists [5]. The use of technology beyond smartphone applications may increase access to peer support services for home-bound individuals, individuals who live in rural areas, and other individuals who have historically been difficult to reach and engage.
The purpose of this study is to examine the extent to which a 4-h Digital Peer Support training program impacts capability, knowledge, and confidence in using digital peer support, beyond smartphones applications.
Methods
An online, single arm pre/post pilot study was conducted with N = 100 peer support specialists to examine the effectiveness of the Digital Peer Support (short course) related to attitudes/ beliefs towards digital peer support, ability to use/ engage in digital peer support, and organizational readiness to implement digital peer support. This study was approved by [blinded for review] Institutional Review Board.
Participants
Eligibility for study participation included the following: (1) individuals that are 18 years and older; (2) individuals self-report as a peer support specialist; and (3) able to provide consent. Exclusion criteria are as follows: (1) individuals that are younger than 18 years old; (2) non-peer support specialists; (3) individuals deemed cognitively impaired and who are unable to provide consent as identified as not being able to register for the digital peer support training.
Measures
Study measures were administered at pre and post-time intervals and were selected to reflect key goals described in the research literature on peer support, including acceptance and use of technology, beliefs in technology, and readiness to implement change.
The Unified Theory of Acceptance and Use of Technology (UTAUT) is a valid, reliable 31 item questionnaire that assesses the likelihood of successful technology adaptation and use of technology [10]. UTAUT has 4 main determinants: performance expectancy, effort expectancy, social influence, and facilitating conditions (e.g., “Do you have the knowledge necessary to operate the system?”, “my interactions with the system would be clear and understandable” and “people who influence my behavior think that I should use the system”.) For the 4 main determinants, response options include “strongly agree”, “agree”, “somewhat agree”, “neutral”, “somewhat disagree”, “disagree”, and “strongly disagree”. UTAUT has demonstrated reliability and validity [11].
The Compatibility Beliefs in Technology is a valid, reliable 21 item questionnaire that assesses “the extent of congruence between a new technology and various aspects of the individual and the situation in which the technology will be utilized” [12]. Compatibility Beliefs in Technology has 3 domains: compatibility with existing work practices, compatibility with prior experience, and compatibility with values. Sample items include “using the system is not similar to anything that I’ve done before” and “using the system does not require significant changes in my existing work routine.” Response options range from 1 (“strongly disagree”) to 7 (“strongly agree”). Compatibility Beliefs in Technology has shown validity and reliability among users of a compatibility relationship management system [13].
Organizational Readiness for Implementing Change is a valid, reliable 12-item questionnaire that assesses the “extent to which organizational members are psychologically and behaviorally prepared to implement organizational change” [14]. Two sample items are “people who work here will do whatever it takes to implement this change” and “people who work here feel confident that the organization can get people invested in implementing this change”. Response options include “disagree”, “somewhat disagree”, “neither agree nor disagree”, “somewhat agree”, and “agree”. Organizational Readiness for Implementing Change has shown both validity and reliability in students enrolled in undergraduate, masters, and doctoral programs in health policy and management [15].
Procedures
Digital Peer Support (Short Course)
The Digital Peer Support Short Course was co-produced with scientists and peer support specialists and designed to promote rapid knowledge gain of telehealth practice during the COVID-19 crisis. This 4-h certification includes dyadic training on: digital communication skills; how to engage service users with technology; technology literacy and usage skills; bonding and connection through technology; available technologies; privacy and confidentiality; monitoring digital peer support; and how to address a digital crisis.
Recruitment
Peer support specialists were recruited via email listservs specifically for peer support specialists and peer support specialist Facebook groups (see recruitment email). Using a convenience sample, 100 peer support specialists who self-identify as peer support specialists to the PI were invited to participate. Participants were emailed a zoom registration for the Digital Peer Support Training. As part of the Zoom registration, we asked the age of participants. If the participant was younger than 18 years old or unable to complete the registration on their own, they were not included in the study.
Informed Consent
During the first 30 min of the Digital Peer Support training, the PI emailed the pre-survey, read the informed consent aloud and answered any questions. Next, [blinded for review] (PI) conducted the 4-h Digital Peer Support training using a HIPAA-compliant version of zoom with 100 peer support specialists. Finally, the PI emailed the post-survey to participants.
Statistical Analyses
Descriptive statistics were conducted to describe the demographic characteristics of the study sample. A paired-samples t-test was conducted to assess the difference between pre and post-data and for statistical significance. Linear mixed models were used to explore statistical results from paired samples t-test further. Descriptive statistics and analyses were computed using SPSS version 17. The PI did not conduct the statistical analysis.
Results
Demographic Characteristics of the Study Sample
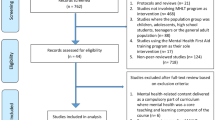
Table 1 presents the sociodemographic characteristics of the sample (n = 75) at baseline. These sociodemographic charactersitics also serve as covariates. The sample had a mean age of 46.9 years (SD = 11.5) and was predominantly female (n = 56, 74.7%) and White (n = 49, 65.3%). The majority of participants completed college or held an advanced degree (n = 47, 62.7%). Participants reported their mental health diagnoses only if they felt comfortable with sharing, diagnosis breakdown can be seen in Table 1. Participants were located throughout the United States, as well as in Canada and the United Kingdom. The majority of participants were located in Illinois (n = 28, 37.3%), Virginia (n = 14, 18.7%), and West Virginia (n = 8, 10.7%).
There were 21 participants who did not complete the post-test, and these participants were not included in the subsequent analysis. Paired samples t-tests were conducted to explore differences in pre-and post-test scores on readiness to use digital peer support, attitudes/beliefs toward digital peer support, organizational readiness for implementing digital peer support, and ability to use/engage in digital peer support. All paired samples t-tests were significant except organizational readiness for implementing digital peer support. Results can be seen in Table 2.
Significant results were further explored using linear mixed models. Linear mixed models were conducted to examine the effects of gender, age, education, psychiatric diagnosis, and location on scores over time. Gender, age, education, psychiatric diagnosis, and location were not significantly associated with scores on readiness to use digital peer support, attitudes/beliefs toward digital peer support, or ability to use/engage in digital peer support.
Discussion
Participants’ confidence in offering digital peer support increased after providing them training. Confidence increased overtime through a better ability to use/egage in digital peer support, a more positive attitude/belief toward digital peer support, and a greater readiness to use digital peer support. This is a particularly encouraging finding since numerous studies have shown a positive correlation between confidence and successfully learning new skills. For example, a 2014 study by Clanton et al. reported an association between confidence and competence in surgical skills after giving medical students a workshop [16]. In “The role of self-confidence in learning to teach in higher education,” author Ian Sadler found relationships between confidence and content knowledge and between confidence and approach to teaching among new teachers [17].
Digital peer support training not only increased confidence but also increased knowledge. This result shouldn't be overemphasized; however, since knowledge differs from actual performance. Just because someone has the knowledge required to complete a certain task, it doesn’t mean they can complete that task; oftentimes, knowledge is only the first step in learning. The brain has two completely different mechanisms for learning new skills and for learning facts or information, and amnesia patients can even successfully learn new skills even while having very poor insight into the knowledge required to learn these skills [18]. This evidence suggests a profound dissociation between knowledge and performance.
Participants’ organizational readiness for implementing digital peer support decreased after training. This decrease may result from an overload of information in a short amount of time. A future study should be conducted in which the information is taught over a more extended period. More time would allow the participants to digest the information better.
Limitations
This study is not without limitations and results should be interpreted with caution. 21 participants did not complete the post-test. This moderate attrition rate may be due to the functionallity, newness, or length of the program. Also, this study is only generalizable to the Digital Peer Support (short course) delivered in an online environment. Of note, we did not request the mental health diagnoses of peer support specialists as they are a protected workforce under the American with Disabilities Act. Rather, individuals were presented with the opportunity to self-report their primary diagnoses on a voluntary basis. Future research should also examine the real-world implications of these results on peer support specialists’ work to see if the results are indicative of implementation of digital peer support and clinical effectiveness among peer support specialists’ clients they serve.
Implications for Behavioral Health
The Digital Peer Support (short course) may be beneficial in rapidly providing diverse groups of peer support specialists with a standardized training framework for delivering peer support over technology mediums. Promising evidence shows that the Digital Peer Support (short course) increases peer support specialists’ attitudes and beliefs towards digital peer support, as well as their ability to use and engage in digital peer support. Widespread dissemination of the Digital Peer Support (short course) may be beneficial in equipping peer support specialists with the skills and resources that are needed to expand the reach of peer support services during the COVID-19 crisis and beyond by increasing access to peer support services for home-bound individuals, individuals who live in rural areas, and other individuals who have historically been difficult to reach and engage.
Contributor Contribution
All authors co-lead the study design, analysis, and write-up of the results. All authors contributed equally.
References
Druss BG, Bradford DW, Rosenheck RA, et al. Mental disorders and use of cardiovascular procedures after myocardial infarction. JAMA. 2000;283(4):506–611 (PMID: 10659877).
Walker ER, McGee RE, Druss BG. Mortality in mental disorders and global disease burden implications: a systematic review and meta-analysis. JAMA Psychiat. 2015;72(4):334–41 (PMID: 25671328).
Druss BG, Zhao L, Von Esenwein S, et al. Understanding excess mortality in persons with mental illness: 17-year follow up of a nationally representative US survey. Med Care. 2011;49(6):599–604 (PMID: 21577183).
Fortuna KL, Naslund JA, LaCroix JM, Bianco CL, Brooks JM, Zisman-Ilani Y, Muralidharan A, Deegan P. Systematic review of digital peer support interventions for people with a lived experience of a serious mental illness. JMIR Mental Health. 2020;7(4):e16460.
Ferron J, Fortuna KL. Landscape of digital peer support. (under review).
Solomon P. Peer support/peer provided services underlying processes, benefits, and critical ingredients. Psychiatr Rehabil J. 2004;27(4):392–401.
World, health, and organization, about social determinants of health. 2017. Available at https://www.who.int/health-topics/social-determinants-of-health.
Fortuna KL, Walker R, Brooks J. Strategies to impact peer support specialists’ capacity to use digital peer support technology. JMIR Mental Health. 2020;7(7):e20429.
Substance Use and Mental Health Services. Mental Health Peer Support Workforce Designline. 2021. Available at: https://www.hca.wa.gov/assets/program/mental-health-peer-support-workforce-designline.pdf.
Venkatesh V, Morris M, Davis G, et al. User acceptance of information technology: Toward a unified view. MIS Q. 2003;27(3):425–78. https://doi.org/10.2307/30036540.
Alshahrani H, Walker D. Validity, reliability, predictors, moderation: The UTAUT model revisited. Gen Linear Model J. 2017;43(2):23–34. https://doi.org/10.31523/glmj.043002.003.
Karahanna E, Agarwal R, Angst C. Reconceptualizing compatibility beliefs in technology acceptance research. MIS Q. 2006;30(4):781–804. https://doi.org/10.2307/25148754.
Pan X. Technology acceptance, technological self-efficacy, and attitude toward technology-based self-directed learning: learning motivation as a mediator. Front Psychol. 2020. https://doi.org/10.3389/fpsyg.2020.564294.
Weiner BJ, Amick H, Lee SY. Conceptualization and measurement of organizational readiness for change: a review of the literature in health services research and other fields. Med Care Res Rev. 2008;65(4):379–436. https://doi.org/10.1177/1077558708317802.
Shea CM, Jacobs SR, Esserman DA, et al. Organizational readiness for implementing change: a psychometric assessment of a new measure. Implementation science : IS. 2014;9:7. https://doi.org/10.1186/1748-5908-9-7.
Clanton J, Gardner A, Cheung M, et al. The relationship between confidence and competence in the development of surgical skills. J Surg Educ. 2014;71(3):405–12. https://doi.org/10.1016/j.jsurg.2013.08.009.
Sadler I. The role of self-confidence in learning to teach in higher education. Innov Educ Teach Int. 2013;50(2):157–66. https://doi.org/10.1080/14703297.2012.760777.
Cohen NJ, Eichenbaum H, Deacedo BS, et al. Different memory systems underlying acquisition of procedural and declarative knowledge. Ann N Y Acad Sci. 1985;444:54–71. https://doi.org/10.1111/j.1749-6632.1985.tb37579.
Acknowledgements
We do not have any acknowledgments.
Funding
The authors received no financial support for the research, authorship, or publication of this article.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
This study was approved by Dartmouth College IRB.
Guarantor
Karen L. Fortuna.
Conflict of Interest
All authors declare that he/she has no conflict of interest. The authors received no financial support for the research, authorship, or publication of this article. Dr. Fortuna offers consulting services through Social Wellness.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Dr. Fortuna provided consulting through Social Wellness
Rights and permissions
About this article

Cite this article
Fortuna, K.L., Brooks, J.M., Myers, A. et al. Effectiveness of a Digital Peer Support Training Program Designed for Rapid Uptake Among Peer Support Specialists Pilot Study. Psychiatr Q 93, 783–790 (2022). https://doi.org/10.1007/s11126-022-09984-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11126-022-09984-5