
Abstract
Prior research suggests that brief interventions (BIs) for alcohol and other drug use may vary in effectiveness across patient sociodemographic factors. The objective of this individual participant data (IPD) meta-analysis was to explore for whom BIs delivered in general healthcare settings are more or less effective. We examined variability in BI effects by patient age, sex, employment, education, relationship status, and baseline severity of substance use using a two-stage IPD meta-analysis approach. All trials included in a parent aggregate data meta-analysis (k = 116) were invited to contribute IPD, and 29 trials provided patient-level data (12,074 participants). Among females, BIs led to significant reductions in binge alcohol consumption (\(\overline{g }\) = 0.09, 95% CI [0.03, 0.14]), frequency of alcohol consumption (\(\overline{g }\) = 0.10, 95% CI [0.03, 0.17]), and alcohol-related consequences (\(\overline{g }\) = 0.16, 95% CI [0.08, 0.25]), as well as greater substance use treatment utilization (\(\overline{g }\) = 0.25, 95% CI [0.21, 0.30]). BIs yielded larger reductions in frequency of alcohol consumption at 3-month follow-up for individuals with less than a high school level education (\(\overline{g }\) = 0.16, 95% CI [0.09, 0.22]). Given evidence demonstrating modest BI effects on alcohol use and mixed or null findings for BI effects on other drug use, BI research should continue to investigate potential drivers of effect magnitude and variation.
Protocol registration details:
The protocol for this review was pre-registered in PROSPERO #CRD42018086832 and the analysis plan was pre-registered in OSF: osf.io/m48g6.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Substance use disorders and related injuries are among the top five causes of death for adolescents in North America (World Health Organization, 2020) and among the top 20 causes of premature mortality for North American adults (Pan American Health Organization [PAHO], 2021). In 2019 alone, there were 85,984 deaths in North America attributed to substance use, accounting for almost 50% of substance use disorder deaths globally (PAHO 2021). The impact of substance misuse necessitates timely, effective substance use prevention and treatment. Because general healthcare settings (e.g., emergency department or primary care clinics) are more highly utilized than specialist care settings, they may allow for the broadest reach of prevention services aimed at reducing harmful substance use. Moreover, because individuals with a variety of healthcare needs (potentially unrelated to substance misuse) commonly present in general healthcare settings, there may be increased opportunity in these settings for healthcare professionals to screen for and discuss alcohol and other drug use with patients with previously undetected substance misuse.
Brief interventions (BIs) are one evidence-based and widely implemented strategy for preventing substance use problems (Solberg et al., 2008; Tanner-Smith & Grant, 2019). Here, BIs are defined as time-limited and structured interventions that aim to produce positive change in substance use behaviors or their determinants. BIs are commonly delivered within a screening, brief intervention, and referral to treatment (SBIRT) model to non-treatment-seeking individuals who may report harmful levels of alcohol use (SAMHSA, 2013). In this population, a key goal of the BI is to assist patients to develop awareness of substance use levels that are problematic and to enhance motivation to reduce substance use (SAMHSA, 2013; Tanner-Smith & Grant, 2019). BIs can be incorporated into a variety of settings given their brevity, low-cost, flexible structure, and their ability to be delivered by professionals and non-clinical interventionists alike (Kunz et al., 2004; Neighbors et al., 2010; Wutzke et al., 2001). Together these attributes make BIs an attractive prevention approach for substance use problems.
A large body of literature has examined the effectiveness of BIs for alcohol and other drug use problems. Generally consistent, modest effects have been found for BIs targeting alcohol use (Bertholet, 2005; Kaner et al., 2018; Tanner-Smith & Lipsey, 2015; Tanner-Smith et al., 2021). Less research has examined the effectiveness of BIs delivered in primary care settings for drugs other than alcohol, and here BIs often show null or inconsistent effects (Saitz, et al., 2014; Saitz, 2020; Tanner-Smith et al., 2021; Young et al., 2014). Because findings of BI trials have been inconsistent, especially for drugs other than alcohol, there have been calls to more carefully examine variability in BI effectiveness and to consider alternate ways to address unhealthy substance use (Hingson & Compton, 2014; Saitz, 2020).
Several rigorous randomized controlled trials have examined variation in the effectiveness of BIs according to patient characteristics (e.g., sociodemographic and psychosocial contextual risk factors), suggesting that some patient subgroups are more or less likely to benefit from this form of low-intensity intervention. For example, in a sample largely composed of persons with low income, high unemployment, and high rates of mental and physical health comorbidities, there was no evidence of positive BI effects on drug use, heavy episodic drinking, and drug use consequences at 6 months post-treatment regardless of the length of BI (i.e., BI lasting 15 min vs. a BI that included a 35–40-min motivational interviewing enhancement; Saitz et al., 2014). In contrast, other rigorous evidence suggests that BIs delivered in primary care settings are effective at reducing risky drug use at 3 months post-intervention in racially and ethnically diverse adult populations (Gelberg et al., 2015, 2017). In another trial conducted with women experiencing high degrees of psychosocial risk (e.g., interpersonal violence, histories of childhood sexual abuse) and mental health comorbidities (e.g., depression and post-traumatic stress disorder), a BI delivered in an emergency department setting had no effect on alcohol use outcomes (Rhodes et al., 2015). Other evidence suggests that BIs may have little or no effect for patients experiencing psychiatric comorbidities (Walton et al., 2008). Prior research has also demonstrated that BI effects on drug use are greater in treatment-seeking patients (versus screened samples), and that BIs may be less effective for persons experiencing greater severity of substance use (Patnode et al., 2020; Saitz, 2010). Evidence from prior systematic reviews and meta-analyses also suggests variability in BI effects by patient characteristics. For instance, results from a recent overview of 24 systematic reviews of alcohol-focused BIs found little evidence of benefit among adolescent and aging adult populations, women, persons experiencing unstable housing, and minoritized racial and ethnic populations (O’Donnell et al., 2014).
Although these findings suggest variability in effectiveness of BIs according to participant characteristics, to our knowledge, all systematic reviews or meta-analyses on BIs delivered in general healthcare settings have analyzed aggregate, or study-level, data (AD). AD meta-analyses are best able to examine moderators that do not vary within studies (e.g., methodological features of the study or features of the intervention in each study). Analyzing moderators that vary within studies, such as participant age or other demographic characteristics, using AD (i.e., summary values like means or proportions) can misrepresent true moderation effects (Parr et al., 2019; Tanner-Smith et al., 2022). Moreover, because any given subgroup of patients within a trial may be quite small, individual trials are often underpowered to detect meaningful subgroup differences. The field is thus limited in its ability to determine which patients benefit most from BIs, hampering efforts to deliver substance use interventions to patients for whom they are most likely to be effective.
To address these limitations, research on BIs for alcohol and other drug use has begun to use individual participant data (IPD) meta-analysis in areas including BIs for unhealthy college drinking (Huh et al., 2015; Huh et al., 2022; Mun et al., 2022). IPD meta-analysis can be used to harmonize and analyze data on a large number of individual participants, and allow for questions about patient-level variation in intervention effects to be investigated. Other advantages of IPD meta-analysis compared with AD meta-analysis can include greater precision of effect size estimates, and improved consistency and rigor of treatment-covariate (i.e., moderation) models through direct re-analysis of primary study data (Cooper & Patall, 2009). These relative advantages can yield clearer insights into variability in intervention effects and provide more actionable findings to practitioners and policymakers. The current study is an effort to consolidate and synthesize IPD from multiple BI trials to examine which patient characteristics might moderate the effectiveness of alcohol- and drug-focused BIs delivered in general healthcare settings.
Study Objective
The primary objective of this IPD meta-analysis was to explore for whom BIs delivered in general healthcare settings are more or less effective across a range of outcomes: alcohol and other drug use, tobacco use, alcohol and other drug-related consequences, mental and physical health, emergency department use, substance use treatment utilization, and readiness to change substance use behaviors. We examined variability in BI effects by patient age, sex, employment, education, relationship status, and baseline severity of substance use at three follow-up timepoints (3 months, 6 months, and 12 months post-baseline).
Methods
Protocol and Pre-registration
The protocol for this IPD meta-analysis was pre-registered in the PROSPERO registry #CRD42018086832 (Tanner-Smith et al., 2018) and the analysis plan was pre-registered on OSF (Tanner-Smith et al., 2020; osf.io/m48g6). Any deviations from the pre-registered protocol are justified and documented on OSF.
Study Eligibility Criteria and Search Strategy
This IPD meta-analyses used data from a larger parent project that also involved an AD meta-analysis (Tanner-Smith et al., 2021). Study eligibility for the parent project included the following: a randomized controlled trial (RCT) that used a no treatment, straw-person, sham intervention, or practice as usual comparison condition to evaluate the effects of an alcohol or other drug-focused BI delivered in a general healthcare setting; the study was reported in 1990 or thereafter; the study reported on at least one post-BI outcome of substance use or substance-related consequences; the BI in each study must have been delivered in four or fewer sessions to participants recruited in a general healthcare setting (e.g., primary care, general hospital, emergency department).
To identify trials meeting the inclusion criteria, we completed the following: (a) searched the following databases through March 31, 2020: PubMed; Nursing/Academic Edition (EBSCO host); ERIC, Applied Social Sciences Index and Abstracts, Dissertations & Theses Global, Social Services Abstract (ProQuest host); PsycINFO (PsycNET host); Cochrane Central Register of Controlled Trials; the WHO International Clinical Trials Registry; and the NIH RePORTER website (see Supplemental Material 1 for the full PubMed search strategy); (b) reviewed the bibliographies of all screened and eligible studies as well as all prior reviews and meta-analyses for additional studies; and (c) performed hand-searches of the 1990–2020 tables of contents in the journals Addiction, Addictive Behaviors, Campbell Systematic Reviews, and Journal of Studies on Alcohol and Drugs. See Supplemental Material 1 for the search terms used.
Study Selection
To identify eligible studies and extract aggregate level study data, a team of research assistants (RAs) were trained and supervised by senior author ETS. First, reviewers screened titles and abstracts to remove ineligible studies. Any study that was determined to be potentially eligible by at least one reviewer in this stage proceeded to the second state of screening. During the second stage of screening, two reviewers independently reviewed the full text to determine study eligibility. Finally, at the third stage, two reviewers independently extracted AD for eligible trials. When disagreements in the second and third stages of screening and data extraction arose, they were resolved by senior author ETS. Data extraction was conducted using a standardized coding protocol and RAs entered data into a FileMaker Pro database. Aggregate study data extracted and coded in this database were primarily used to describe primary study characteristics and assess risk of bias.
IPD Data Collection and Data Synthesis
Primary study investigators of all eligible trials included in the AD meta-analysis (Tanner-Smith et al., 2021) were contacted through email with an overview of the proposed IPD meta-analysis and an invitation to collaborate. Following initial contact, primary study investigators were sent a scripted email and offered their preference of either (1) a teleconference with the IPD meta-analysis principal investigator and project managers and/or (2) an email containing detailed information on the proposed IPD meta-analysis, a templated data sharing/data use agreement, information concerning the de-identification of data and protection of human subjects, and options for the secure transfer of data. In the case of no response, a series of reminder emails were sent every 2 weeks for 2 months. If no response was received, the IPD were recorded as unavailable due to investigator non-response. When available, IPD from primary studies were acquired directly from open-access data repositories.
All data cleaning and analysis were performed in the R environment (R Core Team, 2019; RStudio Team, 2019). Individual trial data were checked for consistency with published reports, including checking for missing values, comparing study sample size against published study reports and trial registries, and data distributions were checked for any missing, invalid, out of range, or inconsistent values. Baseline equivalence between primary study arms were checked using all available demographics. Data inconsistencies or missing data were discussed with relevant study investigators and corrected when necessary.Footnote 1 Data were then recoded for consistency across all studies in terms of the directionality of outcomes and the levels of each moderator of interest (see Supplemental Material 2 for notes on data harmonization and coding of all moderators and outcome domains).
Effect Sizes
Pretest-adjusted standardized mean differences for patient subgroups of interest (e.g., the marginal subgroup effect estimated from a model that included the interaction between the intervention condition and moderator of interest) were the effect sizes estimated for each individual trial during the first stage of analysis (the estimation of overall intervention effectiveness is reported in the project’s corresponding AD meta-analysis (Tanner-Smith et al., 2021)). In the second stage of analysis, these effect sizes were then synthesized into pooled pretest-adjusted standardized effects. Primary domains included alcohol consumption (frequency and quantity), binge alcohol use, other drug consumption (frequency and quantity), cannabis consumption, tobacco consumption, alcohol-related consequence, and other drug consequences. Secondary domains included physical health, mental health, substance use treatment utilization, emergency department utilization, and readiness to change.
Moderator Domains
Data were harmonized and coded for the following moderator variables when available in primary studies.Footnote 2 Age was harmonized into a three-level factor: adolescent (under 18); young adult (18–25); adult (26 or older). Housing status was a dichotomous variable with 0 representing being currently unhoused and 1 representing having stable housing. Employment status was a dichotomous variable with 0 representing being unemployed and 1 representing being currently employed half-time or greater. Education was a dichotomous variable with 0 representing have below a high school level of education and 1 representing having obtained a high school diploma/equivalent or greater. Note that adolescents below 18 years of age were not coded for education due to confounding with age, that is, that it would generally not have been possible for this subgroup to have obtained a high school education. Relationship status was coded as 0 representing a single relationship status, including being divorced, separated, or widowed; 1 was coded as being married, which could include marriage, a stable partnership, or having a current partner. Sex was coded dichotomously with 0 representing male and 1 representing female. Last, baseline severity of substance use was coded as a three-factor categorical variable, using the AUDIT or ASSIST. Low baseline severity of use was represented by an AUDIT score of 1–7 or ASSIST total score of 1–3; moderate baseline severity of use was represented by an AUDIT score of 8–15 or ASSIST total score of 4–26; last, high baseline severity of use was represented by an AUDIT score of 16 or above or an ASSIST total score of 27 or above.
Study Reporting Quality, Risk of Bias, Design Assessment
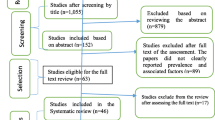
For all included IPD studies, risk of bias assessments were collected using Cochrane’s risk of bias tool for RCTs (Higgins & Altman, 2008). Studies were given ratings of high, low, or unclear risk of bias in six domains, defined as low (all domains rated low), high (any domain rated high), and unclear (any domain rated unclear and no domains rated high). Publication bias was quantitatively and graphically assessed in the corresponding AD meta-analysis (Tanner-Smith et al., 2021). In the online supplement, we present descriptive comparisons between AD studies and studies that contributed IPD. In Fig. 1, we report information on the proportion of primary studies and primary study participants obtained, and the reasons primary study data were not available. The reporting of this IPD meta-analysis was guided by the standards of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses of IPD (PRISMA IPD) Statement (Stewart et al., 2015).

© Reproduced with permission of the PRISMA IPD Group, which encourages sharing and reuse for non-commercial purposes
PRISMA IPD flow diagram. Note. The PRISMA flow diagram of the selection process and efforts to obtain eligible individual participant data. IPD, individual participant data.
Analytic Strategy
Analysis of IPD was carried out using a two-stage modeling approach (Burke et al., 2017; Stewart et al., 2012; see Supplemental Material 3 for the pre-registered analysis plan). The two-stage approach was selected for interpretability and because it simplified handling of missing data at the study level (Koopman et al., 2007). The two-stage approach can be used to synthesize subgroup marginal means, which allowed us to present BI treatment effects for the subgroups of interest (e.g., men and women, individuals with low, moderate, and high severity of baseline substance use) in a clinically useful way. Before the first stage of analysis, missing data were recovered using multiple imputation. Imputation was carried out at the individual study level using all available study data. Predictor and outcome variables in all studies were then standardized so that model output was in the form of standardized regression coefficients.
In the first stage of the IPD meta-analysis, pretest-adjusted intervention effects and intervention by covariate interaction effects were estimated at the primary study level, resulting in marginal subgroup effect estimates. Due to this two-stage analytic strategy, only one treatment-covariate interaction was included in each model (e.g., age × treatment). In the second stage, marginal subgroup effect estimates were pooled across studies using random-effects meta-analysis models with standard inverse-variance weighting. Mean effect sizes and 95% confidence intervals are presented for each analysis. A Benjamini–Hochberg procedure for multiple comparisons (Benjamini & Hochberg, 1995) was implemented to control false discovery rates within an outcome domain.
Pooled mean effect sizes were estimated separately for the primary and secondary outcome domains and within each follow-up time-period (i.e., 1–3 months, 6 months, 9–12 months). To maintain independence of the effect size estimates in each analysis, only one effect size per individual participant dataset for each domain (e.g., frequency alcohol consumption, other drug consumption) and at each timepoint (e.g., 3-month, 12-month) was included in each analysis. For studies that reported multiple outcome effect sizes within domains (for example, weekly and monthly frequency of alcohol use), we used decision rules to select the effect size to be included in the analysis. Specifically, preference was given to effect sizes that were (1) continuous measures versus dichotomous measures; (2) more general measures (e.g., general mental health versus depression or anxiety scores); (3) the effect size reported for the time frame that was most consistently available across all studies; (4) the effect size that had a corresponding baseline score; and (5) the effect size specific to drug or alcohol consequences (i.e., an emergency department visit related to substance use versus all hospitalizations). Regarding dependences for studies with multiple treatment contrasts (e.g., control versus screening and assessment; control versus BI), we selected the treatment contrast between the most minimally intensive control group and the most intensive intervention. A sensitivity analysis was used to assess whether the contrast between the selected control and intervention conditions (e.g., screening and assessment) substantively altered study findings (see Supplemental Material 4 for results from the sensitivity analysis; findings were robust to this modeling decision). Publication bias was assessed using Orwin’s fail safe N and funnel plots (see Supplemental Material 8).
Results
Study and Participant Characteristics
In the parent AD meta-analysis, 116 trials met eligibility criteria (Tanner-Smith et al., 2021). While all eligible trials were invited to contribute IPD, 29 clinical trials provided patient-level data (Fig. 1; see Supplemental Material 5 for references of included trials and Supplemental Material 6 for study characteristics of all included studies). In total, 12,074 participants were included in this meta-analysis; 6,577 (54.5%) received a BI for alcohol or other drug use and 5497 (45.5%) were allocated to a no treatment, straw-person, sham intervention, or practice as usual comparison condition, with the most common control being treatment as usual (45%). Trials were conducted in the USA and Canada (k = 17; 55%) and internationally (k = 13, 45%). The majority of trials were conducted with a sample at elevated risk for substance use behavior (97%); most trials used an individual, randomized controlled trial design (90%). Most trials targeted mixed alcohol and other drug use (k = 11, 38%) or alcohol only (k = 14; 48%), with only four trials targeting specific drugs (14%). Across the trials, BIs were most commonly delivered by behavioral specialists (k = 10, 34%), via in-person formats (k = 25, 86%), and at emergency department (k = 10, 34%) or community healthcare settings (k = 11, 38%). Trials commonly followed up with participants at 3 months post-treatment (72%), although some trials had longer follow-ups at 6 months (55%) or 12 months post-treatment (48%; see Table 1). Statistical comparisons between the IPD sample and the AD sample are also reported in Table 1 to assess for the representativeness of the IPD sample against the known body of studies reflected in the AD meta-analysis (see Supplemental 7 for statistical comparisons between the IPD sample and the AD sample that does not include the IPD studies).
Sociodemographic characteristics were collected at baseline for all trials but were not reported consistently across trials. Most participants were adults (26 or older; n = 5,645, 46.8%), followed by young adults (18–25 years; n = 2,175, 18%). Only a small portion of the sample were adolescents (n = 487, 4%). For those participants who reported sex, 48.9% reported being male (n = 5,903) and 38.7% (n = 4,675) reported being female. Among participants who had other sociodemographic data available, the majority of participants reported stable housing (n = 749, 6.2%), being unemployed (n = 1,461, 12.1%), a single relationship status (n = 4,509, 37.3%), and having a high school education or above (n = 4,036, 33.4%). Among participants who had available baseline severity of substance use data, the majority of participants reported low baseline severity of substance use (n = 1,377, 11.4%) followed by moderate use (n = 824, 6.8%) and then high use (n = 296, 2.5%). Due to inconsistency in reporting of race across primary studies, an adequate representation of all racial and ethnic groups was not possible. Rather, race was dichotomized as non-White and White; 3,238 participants reported being part of non-White racial and ethnic groups (26.8%) and 3,344 participants reported being White (37.7%). The sociodemographic characteristics of the pooled sample are presented in Supplement 7, Table 16; characteristics are also presented by treatment and control conditions, and the proportion of missing data for each of the variables is included. All conclusions about statistical significance below are after correcting for multiple comparisons. Model results corresponding to forest plots are presented in Supplemental Material 7.
Primary Domains
Binge Alcohol Use
For alcohol consumption at 3 months post-treatment, BIs led to significant reductions in heavy episodic (hereafter referred to as binge) alcohol consumption for females (\(\overline{g }\) = 0.09, 95% CI [0.03, 0.14]; k = 10), whereas no beneficial effect was observed for males (see Fig. 2Footnote 3). Heterogeneity across effects was minimal, suggesting that comparable effects for females could be expected in future similar trials (95% PIg [0.03, 0.14]).

Marginal mean subgroup difference in binge alcohol use shown with 95% confidence intervals
Frequency of Alcohol Use
BIs lead to significant reductions in frequency of alcohol consumption among females (\(\overline{g }\) = 0.10, 95% CI [0.03, 0.17]; k = 11) (see Fig. 3); heterogeneity across effects was minimal suggesting that comparable beneficial effects for females could be expected in future similar trials (95% PIg [0.03, 0.17]). Similarly, results showed that BIs led to significant reductions in frequency of alcohol consumption at 3 months follow-up for individuals with below high school levels of education (\(\overline{g }\) = 0.16, 95% CI [0.09, 0.22]; k = 6). Heterogeneity in effects was minimal suggesting that similar beneficial effects for individuals with education levels below high school could be expected in future comparable trials (95% PIg [0.09, 0.22]).

Marginal mean subgroup difference in frequency alcohol use shown with 95% confidence intervals
Quantity of Alcohol Use
There was no evidence that BIs led to statistically significant reductions in the quantity of alcohol use for any subgroup moderator of interest at any follow-up assessment period (see Fig. 4).

Marginal mean subgroup difference in quantity alcohol use shown with 95% confidence intervals
Cannabis, Tobacco, and Other Drug Use
There was no evidence of BIs resulting in beneficial effects for any subgroup of interest for the frequency of cannabis consumption (Fig. 5), and quantity of cannabis consumption outcomes at any 3-, 6-, or 12-month timepoint (Fig. 6), although results should be interpreted with caution given that there were few trials that contributed data (k ranged from 2 to 5). No evidence of significant marginal mean subgroup effects at 3 months, 6 months, or 12 months post-treatment for any tobacco use consumption outcome was identified (Fig. 7). Again, these results should be interpreted with caution given the small number of studies contributing effect sizes for these analyses (k ranged from 2 to 6). Last, there was no evidence of significant marginal mean subgroup effects found at 3 months, 6 months, or 12 months post-treatment for other drug use consumption (Fig. 8).

Marginal mean subgroup difference in frequency cannabis use shown with 95% confidence intervals

Marginal mean subgroup difference in quantity cannabis use shown with 95% confidence intervals

Marginal mean subgroup difference in tobacco use shown with 95% confidence intervals

Marginal mean subgroup difference in other drug use shown with 95% confidence intervals
Alcohol and Other Drug Consequences
At 3 months post-treatment, BIs led to significant reductions in alcohol-related consequences for females (\(\overline{g }\) = 0.16, 95% CI [0.08, 0.25]; k = 7), but not for males (see Fig. 9). Heterogeneity across effects was minimal suggesting that similar beneficial effects for females could be expected in future similar trials (95% PIg [0.08, 0.25]). No evidence of statistically significant marginal mean subgroup effects was found at 3 months, 6 months, or 12 months post-treatment for other drug-related consequences (Fig. 10).

Marginal mean subgroup difference in alcohol-related consequences shown with 95% confidence intervals

Marginal mean subgroup difference in drug-related consequences shown with 95% confidence intervals
Secondary Domains
Mental and Physical Health
There was no evidence that BIs were associated with statistically significant reductions in mental health symptoms (see Fig. 11) or physical health symptoms (Fig. 12), though these results should be interpreted with caution given the small number of studies contributing data to these analyses (k ranged from 2 to 4).

Marginal mean subgroup difference in mental health symptoms shown with 95% confidence intervals

Marginal mean subgroup difference in physical health symptoms shown with 95% confidence intervals
Service Utilization
BIs led to greater substance use treatment utilization at 3 months post-treatment for females (\(\overline{g }\) = 0.25, 95% CI [0.21, 0.30]; k = 3; see Fig. 13) but not males. Heterogeneity across effects was minimal suggesting that similar beneficial effects for females could be expected in future similar trials (95% PIg [0.11, 0.39]). There was no evidence that BIs were associated with statistically significant reductions in emergency department use (see Fig. 14).

Marginal mean subgroup difference in substance use service utilization shown with 95% confidence intervals

Marginal mean subgroup difference in emergency department utilization shown with 95% confidence intervals
Readiness to Change
No evidence of significant marginal mean subgroup effects was found at 3 months, 6 months, or 12 months post-treatment for readiness to change (Fig. 15). These results should be interpreted with caution given the small number of studies contributing effect sizes for these analyses (k ranged from 2 to 6).

Marginal mean subgroup difference in readiness to change shown with 95% confidence intervals
Discussion
This IPD meta-analysis synthesized findings from 29 trials and 12,074 individual participants, drawn from a larger AD meta-analysis (Tanner-Smith et al., 2021), with the aim of examining key participant characteristics as moderators of the effects of BIs delivered in general healthcare settings on alcohol and other drug use and healthcare utilization, readiness to change, and physical and mental health. Among primary outcomes, there was evidence that BIs led to reductions in alcohol consumption and alcohol-related consequences and increases in substance use treatment utilization, with larger effects occurring for females and individuals with below high school levels of education at 3 months post-intervention. Despite these differences, the absolute effect magnitudes were small. We also found limited beneficial effects of BIs on other drug outcomes or consequences, which is consistent with prior primary research that found few studies (with inconsistent findings) on the efficacy of drug BIs. Overall, there was limited data available on the effects of BIs on tobacco use and substance use treatment utilization, emergency department utilization, physical and mental health outcomes, and readiness to change.
In this synthesis, findings showed that females have larger intervention-driven reductions in alcohol consumption outcomes in the first 3 months following a BI, including greater reductions in binge alcohol consumption and greater reductions in the frequency of use (e.g., number of drinks in the past week or month) relative to control. Further, there was evidence documenting that females also experienced fewer alcohol-related consequences and greater utilization of substance use treatment following receipt of BIs. These findings contrast with a prior AD meta-analysis that found men have larger BI-driven reductions in alcohol consumption relative to females (Kaner et al., 2018). It is possible that the disparity in sex-moderation findings is due to aggregation bias (i.e., examining the proportion of female participants in primary studies as a moderator of BI effects versus examining interactions between sex and treatment condition at the individual level, as was done in this IPD study). Findings also diverge from an AD meta-analysis documenting that BIs do not increase receipt of alcohol-related services (Glass et al., 2015), whereas the current study suggests females may show increased utilization of substance-related (i.e., both alcohol and other drug) treatment services following BI. These differing findings are less surprising when considering that prior reviews also suggest there are a limited number of studies that have data disaggregated by sex and a larger number of primary studies that focus on BI effects for men only (Kaner et al., 2018; Moyer et al., 2002; O’Donnell et al., 2014). Future research should clarify whether there are additional factors that may drive the sex-specific effects documented in this study. For example, Blow and colleagues (2006) document that younger women, in particular, show reduced heavy episodic drinking following receipt of BI. Further, a prior systematic review suggests that pregnant women who endorse abstinence from alcohol use as a goal when enrolling in BI or women who enroll in BI with heavier drinking profiles may show greater BI-driven abstinence from alcohol consumption (Gilinsky et al., 2011). Future studies might consider these interactions between sex, age, and other goals for abstinence or substance use consumption (e.g., reproductive status) to further the field’s understanding of the profiles of and conditions under which women are most likely to benefit from BI receipt.
Our findings also provide evidence that adults with below high school levels of education may particularly benefit from short-term BI-driven reductions in alcohol consumption. Although there is considerable research documenting the association between greater educational attainment and lowered risk substance use or alcohol or other drug dependence (Bloomfield et al., 2006; Daniel et al., 2009; Paljärvi et al., 2013), this relationship is undoubtedly complex and bidirectional, as illustrated by longitudinal studies on the topic (e.g., Fergusson et al., 2008). Further, there are few studies that directly examine the moderating role of educational attainment on BI or other substance-related program effectiveness (in contrast to research on the effects of educational attainment on relapse, substance use treatment enrollment, or program completion, for which there is some evidence). It should be noted that in the current study, adolescents were not included in the education moderator analyses due to potential confounding with age and because, in general, it would not have been possible for adolescents to have yet obtained a high school diploma. Further, in the current study, only 50% of participants across trials had educational attainment data available; therefore, these results should be interpreted with caution.
The findings from this IPD meta-analysis should be interpreted with several limitations in mind. For several patient characteristics (i.e., effect size moderators), data were not available at the primary study level or were otherwise collapsed or dichotomized into categories that were not able to be harmonized across the 29 primary studies. For example, contextual factors known to exacerbate risk for substance use, including housing status, were only reported in two primary studies. Further, baseline severity of substance use was also inconsistently measured and reported and therefore, nearly 80% of individual participants were missing data on this characteristic. Due to the challenges of data availability and harmonizing variables consistently across primary studies, we made the decision to collapse many participant-level moderator categories to facilitate the inclusion of the greatest number of studies in each analysis. We recognize that this approach does not reflect the true range of individuals’ identities or experiences (e.g., relationship status as “Single” or “Married”). Further, in this study, only one treatment-covariate interaction was included in each model, limiting our ability to further disentangle three-way interactions (e.g., age × employment status × treatment status).
The aim of traditional systematic reviews (employing AD) is typically to identify all available studies relevant to its topic, which in turn yields conclusions based on the complete or near-complete body of evidence. Although it would be optimal for IPD meta-analyses to achieve the same end, many systemic barriers to data sharing exist (Tan et al., 2021), and these exacerbate other issues like the sufficient recruitment, enrollment, and reporting of members of important subgroups. Such barriers are among several commonly faced by researchers conducting IPD meta-analysis that impact the availability of IPD; in our case, these obstacles resulted in an analytic sample comprising one quarter of the studies in the parent AD meta-analysis described above.Footnote 4 We recommend that institutions and funders allocate resources for initiatives that promote the practice of data sharing. These systems-level movements have the potential to facilitate data transparency and promote a more complete, nuanced, and clinically meaningful understanding of how BI and other intervention effects may vary according to participant characteristics. Short of conclusions resting on the “full” body of evidence, however, findings of IPD meta-analyses are based on a larger amount of data than any one study. Consequently, we argue that findings from IPD meta-analyses should not be gauged by the extent to which they represent all available studies on a topic, but instead by whether the studies that are included provide accurate and meaningful estimates of the moderation effects of interest.
Alcohol and other drug use continues to be a public health crisis with profound effects on individuals, families, and communities. The breadth of research on BIs directed at interrupting substance use problems and the negative sequalae that follow demonstrates the field’s commitment to supporting individuals affected by substance use challenges. The current study contributes to a more nuanced understanding of the impact of BIs delivered in general healthcare settings by identifying specific patient groups that may benefit more (or less) from this type of intervention. In light of evidence demonstrating modest BI effects on alcohol use and mixed or null findings for BI effects on other drug use, BI research should continue to investigate potential drivers of effect magnitude and variation. Although the significant BI effects on alcohol use were modest, it is possible that these small effects may be clinically meaningful when evaluated at the population level; therefore, along with others (e.g., Heather, 2012), we suggest researchers consider efforts to examine the population-level effects of BIs in settings where BIs are already widely implemented to determine if BIs result in reductions in population level harms (e.g., rates of alcohol-related illness, injury, or death). Further, even though results show that BIs may lead to modest reductions in alcohol use, it could be that even those small effects are important in interrupting a trajectory of substance use that could be unhealthy, thereby shifting an individual’s substance use from an unhealthier threshold to one that places them at lower risk for negative substance use harms. Researchers should also continue to test novel interventions and program adaptations that could more effectively address substance use for populations for whom BIs demonstrate some evidence of benefit.
Data Availability
Data were obtained through a restricted data use agreement with primary study authors. Data are not publicly available.
Notes
Data inquiries were made with three primary study investigators. Reasons for data queries were: (1) requesting a clustering variable relevant to the study design; (2) clarifying translation and variable accuracy for data provided in a language that was not English; (3) requesting the randomization variable and subsequently verifying original sample size and group baseline characteristics.
We planned to examine participant race/ethnicity as a potential moderator (see pre-registered analysis protocol). However, reporting of race was inconsistent across studies and would have necessitated dichotomizing participants into white or non-white subgroups. We judged this approach to be incompatible with our aims of providing finer-grained understanding of BI effects, and ultimately decided against including such a crude race variable among the final set of candidate moderators.
For Figs. 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, and 15 referenced throughout the results section, caution should be used when visually comparing effect size estimates across figures and study domains as x-axis are not consistent across figures. See the online supplement for the complete presentation of all numerical results presented in the following paragraphs.
Though this is the case, the descriptive comparison between the AD and IPD samples presented in Table 1 show that characteristics of primary studies providing IPD are generally comparable to the full sample of studies in the AD parent meta-analysis (See online supplement; Tanner-Smith et al., 2021).
References
Benjamini, Y., & Hochberg, Y. (1995). Controlling the false discovery rate: A practical and powerful approach to multiple testing. Journal of the Royal Statistical Society, 57(1), 289–300. https://doi.org/10.1111/j.2517-6161.1995.tb02031.x
Bertholet, N. (2005). Reduction of alcohol consumption by brief alcohol intervention in primary care: Systematic review and meta-analysis. Archives of Internal Medicine, 165(9), 986. https://doi.org/10.1001/archinte.165.9.986
Bloomfield, K., Grittner, U., Kramer, S., & Gmel, G. (2006). Social inequalities in alcohol consumption and alcohol-related problems in the study countries of the EU concerted action 'Gender, Culture, and Alcohol Problems: A Multi-National Study' Alcohol and Alcoholism, 41(suppl_1), i26–i36. https://doi.org/10.1093/alcalc/agl073
Blow, F. C., Barry, K. L., Walton, M. A., Maio, R. F., Chermack, S. T., Bingham, C. R., Ignacio, R. V., & Strecher, V. J. (2006). The efficacy of two brief intervention strategies among injured, at-risk drinkers in the emergency department: Impact of tailored messaging and brief advice. Journal of Studies on Alcohol, 67(4), 568–578. https://doi.org/10.15288/jsa.2006.67.568
Burke, D. L., Ensor, J., & Riley, R. D. (2017). Meta-analysis using individual participant data: One-stage and two-stage approaches, and why they may differ. Statistics in Medicine, 36(5), 855–875. https://doi.org/10.1002/sim.7141
Cooper, H., & Patall, E. A. (2009). The relative benefits of meta-analysis conducted with individual participant data versus aggregated data. Psychological Methods, 14(2), 165–176. https://doi.org/10.1037/a0015565
Daniel, J. Z., Hickman, M., Macleod, J., Wiles, N., Lingford-Hughes, A., Farrell, M., Araya, R., Skapinakis, P., Haynes, J., & Lewis, G. (2009). Is socioeconomic status in early life associated with drug use? A systematic review of the evidence: Socioeconomic status and drug use. Drug and Alcohol Review, 28(2), 142–153. https://doi.org/10.1111/j.1465-3362.2008.00042.x
Fergusson, D. M., Boden, J. M., & Horwood, L. J. (2008). The developmental antecedents of illicit drug use: Evidence from a 25-year longitudinal study. Drug and Alcohol Dependence, 96(1–2), 165–177. https://doi.org/10.1016/j.drugalcdep.2008.03.003
Gelberg, L., Andersen, R. M., Afifi, A. A., Leake, B. D., Arangua, L., Vahidi, M., Singleton, K., Yacenda-Murphy, J., Shoptaw, S., Fleming, M. F., & Baumeister, S. E. (2015). Project QUIT (Quit Using Drugs Intervention Trial): A randomized controlled trial of a primary care-based multi-component brief intervention to reduce risky drug use: Project QUIT. Addiction, 110(11), 1777–1790. https://doi.org/10.1111/add.12993
Gelberg, L., Andersen, R. M., Rico, M. W., Vahidi, M., Natera Rey, G., Shoptaw, S., Leake, B. D., Serota, M., Singleton, K., & Baumeister, S. E. (2017). A pilot replication of QUIT, a randomized controlled trial of a brief intervention for reducing risky drug use, among Latino primary care patients. Drug and Alcohol Dependence, 179, 433–440. https://doi.org/10.1016/j.drugalcdep.2017.04.022
Gilinsky, A., Swanson, V., & Power, K. (2011). Interventions delivered during antenatal care to reduce alcohol consumption during pregnancy: A systematic review. Addiction Research & Theory, 19(3), 235–250. https://doi.org/10.3109/16066359.2010.507894
Glass, J. E., Hamilton, A. M., Powell, B. J., Perron, B. E., Brown, R. T., & Ilgen, M. A. (2015). Specialty substance use disorder services following brief alcohol intervention: A meta-analysis of randomized controlled trials. Addiction, 110(9), 1404–1415. https://doi.org/10.1111/add.12950
Heather, N. (2012). Can screening and brief intervention lead to population-level reductions in alcohol-related harm? Addiction Science & Clinical Practice, 7, 15. https://doi.org/10.1186/1940-0640-7-15
Higgins, J. P., & Altman, D. G. (2008). Assessing risk of bias in included studies. In J. P. Higgins & S. Green (Eds.), Cochrane handbook for systematic reviews of interventions (pp. 187–241). John Wiley & Sons, Ltd. https://doi.org/10.1002/9780470712184.ch8
Hingson, R., & Compton, W. M. (2014). Screening and brief intervention and referral to treatment for drug use in primary care. JAMA: Journal of the American Medical Association, 312(5), 488–489.
Huh, D., Li, X., Zhou, Z., Walters, S. T., Baldwin, S. A., Tan, Z., Larimer, M. E., & Mun, E.-Y. (2022). A structural equation modeling approach to meta-analytic mediation analysis using individual participant data: Testing protective behavioral strategies as a mediator of brief motivational intervention effects on alcohol-related problems. Prevention Science, 23(3), 390–402. https://doi.org/10.1007/s11121-021-01318-4
Huh, D., Mun, E.-Y., Larimer, M. E., White, H. R., Ray, A. E., Rhew, I. C., Kim, S.-Y., Jiao, Y., & Atkins, D. C. (2015). Brief motivational interventions for college student drinking may not be as powerful as we think: An individual participant-level data meta-analysis. Alcoholism, Clinical and Experimental Research, 39(5), 919–931. https://doi.org/10.1111/acer.12714
Kaner, E. F., Beyer, F. R., Muirhead, C., Campbell, F., Pienaar, E. D., Bertholet, N., Daeppen, J. B., Saunders, J. B., & Burnand, B. (2018). Effectiveness of brief alcohol interventions in primary care populations. Cochrane Database of Systematic Reviews. https://doi.org/10.1002/14651858.CD004148.pub4
Koopman, L., van der Heijden, G. J. M. G., Grobbee, D. E., & Rovers, M. M. (2007). Comparison of methods of handling missing data in individual patient data meta-analyses: An empirical example on antibiotics in children with acute otitis media. American Journal of Epidemiology, 167(5), 540–545. https://doi.org/10.1093/aje/kwm341
Kunz, F. M., French, M. T., & Bazargan-Hejazi, S. (2004). Cost-effectiveness analysis of a brief intervention delivered to problem drinkers presenting at an inner-city hospital emergency department. Journal of Studies on Alcohol, 65(3), 363–370. https://doi.org/10.15288/jsa.2004.65.363
Moyer, A., Finney, J., Searingen, C., & Vergun, P. (2002). Brief interventions for alcohol problems: A meta-analytic review of controlled investigations in treatment-seeking and non-treatment-seeking populations. Addiction, 97, 279–292. https://doi.org/10.1046/j.1360-0443.2002.00018.x
Mun, E.-Y., Li, X., Lineberry, S., Tan, Z., Huh, D., Walters, S. T., Zhou, Z., Larimer, M. E., & in Collaboration with Project INTEGRATE Team. (2022). Do brief alcohol interventions reduce driving after drinking among college students? A two-step meta-analysis of individual participant data. Alcohol and Alcoholism, 57(1), 125–135. https://doi.org/10.1093/alcalc/agaa146
Neighbors, C. J., Barnett, N. P., Rohsenow, D. J., Colby, S. M., & Monti, P. M. (2010). Cost-effectiveness of a motivational intervention for alcohol-involved youth in a hospital emergency department. Journal of Studies on Alcohol and Drugs, 71(3), 384–394. https://doi.org/10.15288/jsad.2010.71.384
O’Donnell, A., Anderson, P., Newbury-Birch, D., Schulte, B., Schmidt, C., Reimer, J., & Kaner, E. (2014). The impact of brief alcohol interventions in primary healthcare: A systematic review of reviews. Alcohol and Alcoholism, 49(1), 66–78. https://doi.org/10.1093/alcalc/agt170
Paljärvi, T., Suominen, S., Car, J., & Koskenvuo, M. (2013). Socioeconomic disadvantage and indicators of risky alcohol-drinking patterns. Alcohol and Alcoholism, 48(2), 207–214. https://doi.org/10.1093/alcalc/ags129
Pan American Health Organization. (2021). Leading causes of mortality and health loss at regional, subregional, and country levels in the Region of the Americas, 2000-2019. ENLACE data portal.
Parr, N. J., Schweer-Collins, M. L., Darlington, T. M., & Tanner-Smith, E. E. (2019). Meta-analytic approaches for examining complexity and heterogeneity in studies of adolescent development. Journal of Adolescence, 77(1), 168–178. https://doi.org/10.1016/j.adolescence.2019.10.009
Patnode, C. D., Perdue, L. A., Rushkin, M., Dana, T., Blazina, I., Bougatsos, C., Grusing, S., O’Connor, E. A., Fu, R., & Chou, R. (2020). Screening for unhealthy drug use: Updated evidence report and systematic review for the US Preventive Services Task Force. JAMA, 323(22), 2310. https://doi.org/10.1001/jama.2019.21381
R Core Team. (2019). R: A language and environment for statistical computing (3.6.0) [Computer software]. R Foundation for Statistical Computing. https://www.R-project.org/
Rhodes, K. V., Rodgers, M., Sommers, M., Hanlon, A., Chittams, J., Doyle, A., Datner, E., & Crits-Christoph, P. (2015). Brief motivational intervention for intimate partner violence and heavy drinking in the emergency department: A randomized clinical trial.JAMA, 314(5), 466. https://doi.org/10.1001/jama.2015.8369
RStudio Team. (2019). RStudio: Integrated development environment for R (1.2.1335) [Computer software]. RStudio, Inc. http://www.rstudio.com/
Saitz, R. (2010). Alcohol screening and brief intervention in primary care: Absence of evidence for efficacy in people with dependence or very heavy drinking: Alcohol SBI for dependence: No evidence. Drug and Alcohol Review, 29(6), 631–640. https://doi.org/10.1111/j.1465-3362.2010.00217.x
Saitz, R. (2020). Screening for unhealthy drug use: Neither an unreasonable idea nor an evidence-based practice. JAMA, 323(22), 2263–2265. https://doi.org/10.1001/jama.2019.20152
Saitz, R., Palfai, T. P. A., Cheng, D. M., Alford, D. P., Bernstein, J. A., Lloyd-Travaglini, C. A., Meli, S. M., Chaisson, C. E., & Samet, J. H. (2014). Screening and brief intervention for drug use in primary care: The ASPIRE randomized clinical trial. JAMA, 312(5), 502. https://doi.org/10.1001/jama.2014.7862
Solberg, L. I., Maciosek, M. V., & Edwards, N. M. (2008). Primary care intervention to reduce alcohol misuse. American Journal of Preventive Medicine, 34(2), 143–152.e3. https://doi.org/10.1016/j.amepre.2007.09.035
Stewart, G. B., Altman, D. G., Askie, L. M., Duley, L., Simmonds, M. C., & Stewart, L. A. (2012). Statistical analysis of individual participant data meta-analyses: A comparison of methods and recommendations for practice. PLOS ONE, 7(10), e46042. https://doi.org/10.1371/journal.pone.0046042
Stewart, L. A., Clarke, M., Rovers, M., Riley, R. D., Simmonds, M., Stewart, G., & Tierney, J. F. (2015). Preferred reporting items for a systematic review and meta-analysis of individual participant data: The PRISMA-IPD statement. JAMA, 313(16), 1657. https://doi.org/10.1001/jama.2015.3656
Substance Abuse and Mental Health Services Administration. (2013) Systems-Level Implementation of Screening, Brief Intervention, and Referral to Treatment. Technical Assistance Publication (TAP) Series 33. HHS Publication No. (SMA) 13-4741. Rockville, MD.
Tan, A. C., Askie, L. M., Hunter, K. E., Barba, A., Simes, R. J., & Seidler, A. L. (2021). Data sharing—trialists’ plans at registration, attitudes, barriers and facilitators: A cohort study and cross‐sectional survey. Research Synthesis Methods, 12(5), 641–657. https://doi.org/10.1002/jrsm.1500
Tanner-Smith, E., Darlington, T., Gelberg, L., & Saitz, R. (2018). Brief substance use counseling interventions to reduce consumption and consequences among patients in general healthcare settings: Understanding variability in effects. https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42018086832
Tanner-Smith, E. E., Grant, S., & Mayo-Wilson, E. (2022). Modern meta-analytic methods in prevention science: Introduction to the special issue. Prevention Science, 23(3), 341–345. https://doi.org/10.1007/s11121-022-01354-8
Tanner-Smith, E. E., & Grant, S. P. (2019). Brief interventions as evidence-based prevention strategies. In Z. Sloboda, H. Petras, E. Robertson, & R. Hingson (Eds.), Prevention of substance use (pp. 181–192). Springer International Publishing. https://doi.org/10.1007/978-3-030-00627-3_11
Tanner-Smith, E. E., & Lipsey, M. W. (2015). Brief alcohol interventions for adolescents and young adults: A systematic review and meta-analysis. Journal of Substance Abuse Treatment, 51, 1–18. https://doi.org/10.1016/j.jsat.2014.09.001
Tanner-Smith, E., Parr, N. J., Schweer-Collins, M. L., & Saitz, R. (2021). Effects of brief substance use interventions delivered in general medical settings: A systematic review and meta-analysis. Addiction, 1–13. https://doi.org/10.1111/add.15674
Tanner-Smith, E., Saitz, R., Gelberg, L., Darlington, T., Parr, N., Schweer-Collins, M., & Frankel, L. (2020). Brief substance use interventions in general healthcare settings meta-analysis. OSF. osf.io/m48g6
Walton, M. A., Goldstein, A. L., Chermack, S. T., Mccammon, R. J., Cunningham, R. M., Barry, K. L., & Blow, F. C. (2008). Brief alcohol interventions in the emergency department: Moderators of effectiveness. Journal of Studies on Alcohol and Drugs, 69(4), 550–560. https://doi.org/10.15288/jsad.2008.69.550
World Health Organization. (2020). Global Health Estimates 2020: Deaths by Cause, Age, Sex, by Country and by Region, 2000-2019. Geneva.
Wutzke, S. E., Shiell, A., Gomel, M. K., & Conigrave, K. M. (2001). Cost effectiveness of brief interventions for reducing alcohol consumption. Social Science & Medicine, 52(6), 863–870. https://doi.org/10.1016/S0277-9536(00)00189-1
Young, M. M., Stevens, A., Galipeau, J., Pirie, T., Garritty, C., Singh, K., Yazdi, F., Golfam, M., Pratt, M., Turner, L., Porath-Waller, A., Arratoon, C., Haley, N., Leslie, K., Reardon, R., Sproule, B., Grimshaw, J., & Moher, D. (2014). Effectiveness of brief interventions as part of the Screening, Brief Intervention and Referral to Treatment (SBIRT) model for reducing the nonmedical use of psychoactive substances: A systematic review. Systematic Reviews, 3(1), 50. https://doi.org/10.1186/2046-4053-3-50
Acknowledgements
We would like to acknowledge the following researchers and staff who collaborated with us by preparing and sharing their original participant-level data and documentation, some of whom shared multiple datasets: Nicolas Arnaud, Sawitri Assanagkornchai, Nicholas Barticevic, Michael Bogenshutz, Gallus Bischof, Pol Bruguera, Cheryl Cherpitel, Elizabeth J D’Amico, Jean-Bernard Daeppen, Jacques Guame, Lillian Gelberg, Jan Gryczynski, Sion Harris, Nick Heather, Kypros Kypri, Catherine Laporte, Michael Mason, Talita Ponce, Karin Rhodes, Gail Rose, Richard Saitz, Katherine Sorsdahl, Anthony Spirito, and Anne Zahradnik. We would also like to acknowledge the research assistants and research associates at the University of Oregon who assisted with data collection. Any opinions, findings, and conclusions expressed in this manuscript are those of the authors and do not necessarily reflect the views of these colleagues.
Funding
The work was supported by the National Institute on Drug Abuse [R01DA043589]. The content is solely the responsibility of the authors and does not necessarily represent the official position or policy of the National Institute on Drug Abuse, National Institutes of Health, or Department of Veterans Affairs.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics Approval
The University of Oregon Institutional Review Board (IRB) review the protocol for this review and determined that the study activities did not meet the definition of research with human subjects according to Titel 45 CFR 46.102 (d-f) and thus did not require IRB approval.
Consent to Participate
Primary study investigators have record of informed consent; all included primary studies had informed consent procedures that allowed for sharing of de-identified data.
Conflict of Interest
ETS, NP, and MSC have no conflicts of interest to declare. RS reports personal fees from University of Oregon to support this work. RS also reports non-financial support from Alkermes, personal fees from American Society of Addiction Medicine, American Medical Association, National Council on Behavioral Healthcare, Kaiser Permanente, UpToDate/Wolters Kluwer, Yale University, National Committee on Quality Assurance, Oregon Health Sciences University, RAND Corporation, Leed Management Consulting/Harvard Medical School, Partners, Beth Israel/Deaconess Hospital, American Academy of Addiction Psychiatry, Group Health Cooperative, Checkup and Choices, International Network on Brief Interventions for Alcohol and Other Drugs (INEBRIA) supported via funds from Systembolaget, Smart Recovery, Karolinska Institute, Institute for Research and Training in the Addictions, Medical Malpractice Expert Witness, Charles University, Brandeis University, and Massachusetts Medical Society outside the submitted work; he also reports research consulting to ABT Corporation (not remunerated). RS is an author of primary studies included in this review but was not involved in the data extraction or data analysis of those studies for this review.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Richard Saitz is a co-author given his significant contributions to this work. He died on January 15, 2022.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Schweer-Collins, M.L., Parr, N.J., Saitz, R. et al. Investigating for Whom Brief Substance Use Interventions Are Most Effective: An Individual Participant Data Meta-analysis. Prev Sci 24, 1459–1482 (2023). https://doi.org/10.1007/s11121-023-01525-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11121-023-01525-1