
Abstract
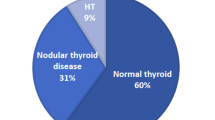
Several studies have associated acromegaly with an increased risk of benign and malignant tumors. While simple and multinodular goiters are common findings in acromegaly, the prevalence of thyroid cancer is uncertain. The objective of this study was to estimate the prevalence of thyroid cancer in a series of acromegalic patients from three hospitals in northeast of Brazil. The methodology used included morphological, cytological and histological thyroid analysis of acromegalic patients and volunteers over 18 years, matched for age and sex and with nodule (s) ≥1 cm. The subjects of this study were 124 acromegalic patients, including 76 females (61.3%) and 48 men (38.7%), with a mean age 45.1 years. Results of the study showed that thyroid ultrasonography was normal in 31 cases (25%), 25 had diffuse goiter (20.1%), 67 had nodules (54%) and one agenesis of the right lobe (0.8%). Thirty-six patients underwent fine needle aspiration biopsy (FNAB) of their nodules and 9 cases of papillary cancer were found (7.2%). The control group consisted of 263 subjects, 156 females (59.3%) and 107 males (40.7%), mean age 44.7 years. In ultrasound assessment, 96 had nodules (36.5%). Of these, 13 were punctured and 2 cases of papillary carcinoma were found (0.7%). These results gave an odds ratio of 10.21 (p = 0.0011, 95% CI 2.17 to 48.01). These findings demonstrate an increased prevalence of thyroid cancer, statistically significant when compared to our control group. Thus, it is suggested that acromegalic patients should be routinely submitted to thyroid ultrasound evaluation, followed by FNAB of nodules when indicated.


Similar content being viewed by others


References
Clayton PE, Banerjee I, Murray PG, Renehan AG (2011) Growth hormone, the insulin-like growth factor axis, insulin and cancer risk. Nat Rev Endocrinol 7:11–24
Melmed S (2006) Medical progress: acromegaly. N Engl J Med 355:2558–2573
Colao A, Ferone D, Marzullo P, Lombardi G (2004) Systemic complications of acromegaly: epidemiology, pathogenesis, and management. Endocr Rev 25:102–152
Melmed S, Colao A, Barkan A et al (2009) Guidelines for acromegaly management: an update. J Clin Endocrinol Metab 94:1509–1517
Cohen P, Clemmons DR, Rosenfeld RG et al (2000) Does the GH-IGF-1 axis play a role in cancer pathogenesis? Growth Horm IGF Res 10: 297–305
Renehan AG, Brennan BM (2008) Acromegaly, growth hormone and cancer risk. Best Pract Res Clin Endocrinol Metab 22:639–657
Melmed S (2001) Acromegaly and cancer: not a problem? J Clin Endocrinol Metab 86:2929–2934
Orme SM, McNally RJ, Cartwright RA, Belchetz PE (1998) Mortality and cancer incidence in acromegaly: a retrospective cohort study. United Kingdom acromegaly study group. J Clin Endocrinol Metab 83:2730–2734
Terzolo M, Reimondo G, Gasperi M et al (2005) Colonoscopic screening and follow-up inpatients with acromegaly: a multicenter study in Italy. J Clin Endocrinol Metab 90:84–90
Rokkas T et al (2008) Risk of colorectal neoplasm in patients with acromegaly: a meta-analysis. World J Gastroenterol 14:3484–3489
Cats A et al (1996) Increased epithelial cell proliferation in the colon of patients with acromegaly. Cancer Res 56:523–526
Bogazzi F et al (2003) Changes in the expression of the peroxisome proliferator-activated receptor gamma gene in the colonic polyps and colonic mucosa of acromegalic patients. J Clin Endocrinol Metab 88:3938–3942
Gasperi M, Martino E, Manetti L, Arosio M, Porretti S, Faglia G et al (2002) Prevalence of thyroid diseases in patients with acromegaly: results of an Italian multicenter study. J Endocrinol Invest 25:240–245
Ruchala M, Skiba A, Gurgul E et al (2009) The occurrence of thyroid focal lesions and a need for fine needle aspiration biopsy in patients with acromegaly due to an increased risk of thyroid cancer. Neuro Endocrinol Lett 30:382–386
Cheung NW, Boyages SC (1997) The thyroid gland in acromegaly: an ultrasonographic study. Clin Endocrinol (Oxf) 46:545–549
Jenkins PJ, Besser M (2001) Clinical perspective: acromegaly and cancer: a problem. J Clin Endocrinol Metab 86:2935–2941
Pollak M (2008) Insulin, insulin-like growth factors and neoplasia. Best Pract Res Clin Endocrinol Metab 22:625–638
Giovannucci E, Harlan DM, Archer MC, Bergenstal RM, Gapstur SM, Habel LA, Pollak M, Regensteiner JG, Yee D (2010) Diabetes and cancer: a consensus report. CA Cancer J Clin 60:207–221
Loeper S, Ezzat S (2008) Acromegaly: re-thinking the cancer risk. Rev Endocr Metab Disord 9:41–58
Kasagi K et al (1999) Goiter associated with acromegaly: sonographic and scintigraphic findings of the thyroid gland. Thyroid 9:791–796
Tita P et al (2005) High prevalence of differentiated thyroid carcinoma in acromegaly. Clin Endocrinol (Oxf) 63:161–167
Baris D et al (2002) Acromegaly and cancer risk: a cohort study in Sweden and Denmark. Cancer Causes Control 13:395–400
Kurimoto M et al (2008) The prevalence of benign and malignant tumors in patient with acromegaly at a single institute. Endocr J 55:67–71
Gullu BE et al (2010) Thyroid cancer is the most common cancer associated with acromegaly. Pituitary 13:242–248
Vannelli GB et al (1990) Insulin-like growth factor-I receptors in nonfunctioning thyroid nodules. J Clin Endocrinol Metab 71:1175–1182
Manousos O et al (1999) IGF-I and IGF-II in relation to colorectal cancer. Int J Cancer 83:15–17
Jenkins PJ et al (2000) Insulin-like growth factor I and the development of colorectal neoplasia in acromegaly. J Clin Endocrinol Metab 85:3218–3221
Suikkari AM et al (1988) Insulin regulates the serum levels of low molecular weight insulin-like growth factor-binding protein. J Clin Endocrinol Metab 66:266–272
Böni-Schnetzler M (1990) Insulin regulates the expression of the insulin-like growth factor binding protein 2 mRNA in rat hepatocytes. Mol Endocrinol 4:1320–1326
Giovannucci E (1995) Insulin and colon cancer. Cancer Causes Control 6:164–179
Brada M et al (1992) Risk of second brain tumour after conservative surgery and radiotherapy for pituitary adenoma. BMJ 304:1343–1346
Tsang RW et al (1993) Glioma arising after radiation therapy for pituitary adenoma. A report of four patients and estimation of risk. Cancer 72:2227
Minniti G et al (2005) Risk of second brain tumour after conservative surgery and radiotherapy for pituitary adenoma: update after an additional 10 years. J Clin Endocrinol Metab 90:800–804
Ayuk J, Stewart PM (2009) Mortality following pituitary radiotherapy. Pituitary 12:35–39
Coeli CM et al (2005) Incidência e mortalidade por câncer de tireóide no Brasil. Arq Bras Endocrinol Metab 49:503–509
Wexler TL et al (2010) Growth hormone status predicts left ventricular mass in patients after cure of acromegaly. Growth Hormon IGF Res 20:333–337
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
dos Santos, M.C.C., Nascimento, G.C., Nascimento, A.G.C. et al. Thyroid cancer in patients with acromegaly: a case–control study. Pituitary 16, 109–114 (2013). https://doi.org/10.1007/s11102-012-0383-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11102-012-0383-y