
Abstract
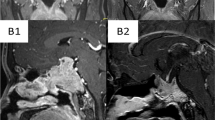
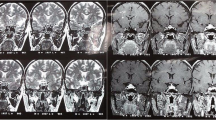
Aggressive fibromatosis (AF) is a rare, locally aggressive, proliferative fibroblastic lesion affecting musculoaponeurotic structures, most often, of the limbs and trunk. Intracranial AF is extremely rare and requires aggressive treatment to prevent recurrence. We present a case of a 34 year-old male with AF involving intracranial structures causing panhypopituitarism and diabetes insipidus. Patient was admitted to hospital because of polyuria, polydipsia, and loss of libido, impotence, hearing loss, and gait disturbance. On cranial magnetic resonance imaging, the lesion extended through the sphenoid sinus into the both pterygoid recesses, destroying the left lateral wall of the sphenoid sinus and invading the retroorbital area. There was also a distinct lesion in the hypothalamic area. The tumor was markedly isointense on both T2- and T1-weighted images relative to gray matter, and enhanced strongly after administration of gadolinium. The patient underwent partial resection of the lesion via a transcranial approach. The pathological examination of the mass was reported as AF. No other sites were found to be involved by thorax and abdominal tomography. Hormonal assessment of hypothalamic-pituitary dysfunction revealed panhypopituitarism with central diabetes insipidus. Replacement therapy was instituted. In this case, standard treatment of wide-field surgical resection was impossible. On the basis of reports that radiotherapy is an effective treatment for this kind of tumor, we administered radiation to the affected area, since chemotherapy and hormonal treatment of non-resectable tumors are not satisfactory. To our knowledge, this is the first reported case of AF presenting as panhypopituitarism with central diabetes insipidus.
Similar content being viewed by others

Abbreviations
- AF:
-
Aggressive Fibromatosis
References
Reitamo JJ, Scheinin TM, Havry P. The desmoid syndrome. New aspects in the cause, pathogenesis and treatment of the desmoid tumor. Am J Surg 1986;151:230–237.
Mehrotra AK, Sheikh S, Aaron AD, Montgomery E, Goldblum JR. Fibromatoses of the extremities: clinicopathologic study of 36 cases. J Surg Oncol 2000;74:291–296.
MacKenzie DH. The fibromatoses: a clinicopathological concept. Br Med J 1972;4:277–281.
Shields CJ, Winter DC, Kirwan WO, Redmond HP. Desmoid tumors. Eur J Surg Oncol 2001;27:701–706.
Wilkins SA Jr, Waldron CA, Mathews WH, Droulias CA. Aggressive fibromatosis of the head and neck. Am J Surg 1975;130:412–415.
Posner MC, Shiu MH, Newsome JL, Hajdu SI, Gaynor JJ, Brennan MF. The desmoid tumor. Not a benign disease. Arch Surg 1989;124:191–196.
Duggal A, Dickinson IC, Sommerville S, Gallie P. The management of extra-abdominal desmoid tumours. Int Orthop 2004;28:252–256.
Reitamo JJ, Scheinin TM, Hayry P. The desmoid syndrome. New aspects in the cause, pathogenesis and treatment of the desmoid tumor. Am J Surg 1986;151:230–237.
Phillips SR, A'Hern R, Thomas JM. Aggressive fibromatosis of the abdominal wall, limbs and limb girdles. Br J Surg 2004;91:1624–1629.
Ballo MT, Zagars GK, Pollack A. Radiation therapy in the management of desmoid tumors. Int J Radiat Oncol Biol Phys 1998;42:1007–1014.
Mavrakis AN, Tritos NA. Diagnostic and therapeutic approach to pituitary incidentalomas. Endocr Pract 2004;10:438–444.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gursoy, A., Cesur, M., Aktaş, B. et al. Intracranial aggressive fibromatosis presenting as panhypopituitarism and diabetes insipidus. Pituitary 8, 123–126 (2005). https://doi.org/10.1007/s11102-005-3758-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11102-005-3758-5