
Abstract
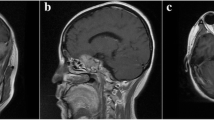
Objective and importance Thyrotroph cell adenoma accounts for only 1% of all pituitary adenomas. This tumor is tough and firm because of significant interstitial fibrosis, and is difficult to remove. Atypical adenoma has an aggressive biological character, invades the surrounding structures, and grows rapidly. Atypical thyrotroph cell adenoma is extremely rare. Clinical presentation A 32-year-old man presented with hyperthyroidism and bitemporal hemianopsia. Head magnetic resonance imaging revealed a large sellar tumor compressing the optic chiasma and invading the left cavernous sinus. Intervention Transsphenoidal surgery was performed and subtotal removal was achieved. Histological examination showed atypical thyrotroph cell adenoma. Gamma knife surgery was planned, but the tumor re-grew within 3 months, and reattached to the optic chiasma. Second transcranial surgery failed to remove residual tumor behind the pituitary stalk. Conventional irradiation followed by octreotide administration resulted in decreased tumor size and stable euthyroidism. The tumor has been controlled for 22 months since first surgery and diagnosis. Conclusion Atypical thyrotroph cell adenoma has an aggressive biological character and grows rapidly. Multimodal treatment including medication and radiotherapy is required.



Similar content being viewed by others


References
Bertholon-Greoire M, Trouillas J, Guigard MP, Loras B, Tourniaire J (1999) Mono- and plurihormonal thyrotropic pituitary adenomas: pathological, hormonal and clinical studies in 12 patients. Eur J Endocrinol 140:519–527
Delellis RA, Lloyd RV, Heitz PU, Eng C (eds) (2004) Pathology and genetics of tumors of endocrine organs. International Agency for Research on Cancer, Lyon
Kovacs K, Horvath E (eds) (1986) Tumors of the pituitary gland, 2nd series. Armed Forces Institute of Pathology, Washington
Socin HV, Chanson P, Delemer B, Tabarin A, Rohmer V, Mockel J, Stevenaert A, Beckers A (2003) The changing spectrum of TSH-secreting pituitary adenomas: diagnosis and management in 43 patients. Eur J Endocrinol 148:433–442
Sanno N, Teramoto A, Osamura Y (2001) Thyrotropin-secreting pituitary adenomas. Clinical and biological heterogeneity and current treatment. J Neurooncol 54:179–186
Lloyd RV, Kovacs K, Young WF Jr, Farrel WE, Asa SL, Trouillas J, Kontogeorgos G, Sano T, Scheithauer BW, Horvath E (2004) Pituitary tumours: introduction. In: DeLellis RA, Lloyd RV, Heitz PU, Eng C (eds) WHO classification of tumours. Pathology and genetics. Tumours of endocrine organs. IARC Press, Lyon, pp 10–13
Kontogeorgos G (2005) Classification and pathology of pituitary tumors. Endocrine 28:27–35
Kontogeorgos G (2006) Predictive markers of pituitary adenoma behavior. Neuroendocrinology 83:179–188
Saeger W, Ludecke DK, Buchfelder M, Fahlbusch R, Quabbe HJ, Petersenn S (2007) Pathohistological classification of pituitary tumors: 10 years of experience with the German pituitary tumor registry. Eur J Endocrinol 156:203–216
Thapar K, Scheithauer BW, Kovacs K, Pernicone PJ, Laws ER Jr (1996) P53 expression in pituitary adenomas and carcinomas: correlation with invasiveness and tumor growth fractions. Neurosurgery 38:765–771
Ikeda H, Ogawa Y, Yoshimoto T (1999) Ultrastructural characteristics of TSH-producing adenomas with special reference to its close similarity to BFA-treated pituitary adenoma cells. Pituitary 1:221–226
Ogawa Y, Ikeda H, Yoshimoto T (1996) Ultrastructural changes in cells of human pituitary adenoma treated by Brefeldin A. Jpn J Clin Electron Microsc 29:69–75
Ogawa Y, Tominaga T, Ikeda H (2007) Intrasellar small TSH secreting pituitary adenomas, 2 case reports. No Shinkei Geka 35:679–684
Brucker-Davis F, Oldfield EH, Skarulis MC, Doppman JL, Weintraub BD (1999) Thyrotropin-secreting pituitary tumors: diagnostic criteria, thyroid hormone sensitivity, and treatment outcome in 25 patients followed at the National Institutes of Health. J Clin Endocrinol Metab 84:476–486
Patrick AW, Atkin SL, MacKenzie J, Foy PM, White MC, MacFarlane IA (1994) Hyperthyroidism secondary to a pituitary adenoma secreting TSH, FSH alpha-subunit and GH. Clin Endocrinol (Oxf) 40:275–278
Sanno N, Teramoto A, Osamura Y (2000) Long-term surgical outcome in 16 patients with thyrotropin pituitary adenoma. J Neurosurg 93:194–200
Beck-Peccoz P, Persani L (2002) Medical management of thyrotropin-secreting pituitary adenomas. Pituitary 5:83–88
Caron P, Arlot S, Bauters C, Chanson P, Kuhn JM, Pugeat M, Marechaud R, Teutsch C, Vidal E, Sassano P (2001) Efficacy of the long-acting octreotide formulation (octreotide-LAR) in patients with thyrotropin-secreting pituitary adenomas. J Clin Endocrinol Metab 86:2849–2853
Dhillon KS, Cohan P, Kelly DF, Darwin CH, Iyer KV, Chopra IJ (2004) Treatment of hyperthyroidism associated with thyrotropin-secreting pituitary adenomas with iopanoic acid. J Clin Endocrinol Metab 89:708–711
Mixson AJ, Friedman TC, David AK (1993) Thyrotropin-secreting pituitary carcinoma. J Clin Endocrinol Metab 76:529–533
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ogawa, Y., Tominaga, T. A case of atypical thyrotroph cell adenoma, which re-grew within 3 months after surgery and required multimodal treatment. J Neurooncol 87, 91–95 (2008). https://doi.org/10.1007/s11060-007-9492-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-007-9492-2