
Abstract
The vast majority of individuals with Rett syndrome do not utilize natural speech and therefore require alternative and augmentative communication (AAC). The purpose of the current study was to investigate the use of high- and low-tech AAC modalities by three individuals with Rett syndrome given similar instruction for using both modalities. For all participants, the number of sessions to criterion and cumulative number of trials with independent requests during simultaneous or alternating instruction in the use of a high- and low-tech AAC modality were investigated. Parents conducted all sessions with remote coaching from a research assistant via telecommunication. Each participant exhibited idiosyncratic response patterns in terms of use of their high- and low-tech AAC modalities during instruction but ultimately demonstrated the ability to use both modalities to make requests. Implications for future research and practice pertaining to AAC of individuals with complex communication needs are discussed. This paper is a companion to Girtler et al. (2023).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Rett syndrome is a rare neurodevelopmental disorder associated with a mutation in the X chromosome that primarily affects females. Rett syndrome is characterized by a regression period in early childhood, typically resulting in severe impairments in communication and motor skills (Amir & Zoghbi, 2000; Ellaway & Christodoulou, 2001; Hagberg, 1985; Hagberg & Zoghbi, 2002; NINDS, 2023). The prevalence of Rett syndrome is about one in every 10,000–15,000 girls (Amir & Zoghbi, 2000; Ellaway & Christodoulou, 2001). Although some individuals with Rett syndrome do retain some speech (Bartolotta et al., 2011; Zappella et al., 2001), most typically lose almost all abilities to use natural speech (Bartolotta et al., 2011; Byiers et al., 2014; Sigafoos et al., 2009); thus, individuals with Rett syndrome would benefit from acquiring the ability to use augmentative and alternative communication (AAC) (Sigafoos et al., 1996, 2009; Simacek et al., 2016) to communicate with communication partners, such as family members, teachers or caretakers, and other community members.
AAC involves various levels of support to individuals who need either a supplement to or replacement for natural speech. Aided AAC includes using materials or devices as a tool for producing functional communication (Ganz et al., 2013, 2014; Reichle et al., 2019). Previous studies on communication interventions have incorporated a variety of AAC modalities for individual participants with Rett syndrome (e.g., Byiers et al., 2014; Sigafoos et al., 1996; Simacek et al., 2016; Stasolla et al., 2014; see Amoako & Hare, 2020 and Sigafoos et al., 2009 for a review). AAC materials vary in their level of technological advancement (i.e., low-, mid-, and high-tech; Reichle et al., 2019; Simacek et al., 2016). High-tech AAC includes speech-output technologies, such as Tobii devices activated by eye-gaze as well as iPads or tablets activated manually on touch screens. High-tech devices allow for computer interface and involve digitized or synthesized speech. Mid-tech AAC (e.g., microswitches) includes some speech-output technologies but lack certain features found in high-tech devices, such as text-to-speech and sentence construction. Low-tech AAC does not include any electronics. Examples include communication books and choice boards (Ganz et al., 2013, 2014; Reichle et al., 2019; Simacek et al., 2016).
The extent of motor impairment is heterogeneous in the Rett syndrome population. To illustrate, across six studies that included a total of 16 girls with Rett syndrome who acquired the use of AAC, four of the girls were able to walk independently, four could walk with assistance, five used vocal approximations, and eight could use their hands to some extent (Byiers et al., 2014; Hetzroni et al., 2002; Sigafoos et al., 1996; Simacek et al., 2016, 2017; Stasolla et al., 2014). There is a range of motor deficits that individuals with Rett syndrome can experience, including disturbances in motor movement and planning and abnormalities in muscle tone. Other obstacles to communication can include the presence of irregular breathing, seizures, sleep difficulties, fatigue, Scoliosis, gastro-intestinal issues, and stereotypic behavior (Mackay et al., 2017; Neul et al., 2010; Stasolla et al., 2014; Townend et al., 2020). These patterns, which can all interfere with the ability to use ACC requiring activation using hands, tend to also be idiosyncratic (Erlandson & Hagberg, 2005). Advancements in AAC technology as well as demonstrations from previous literature (e.g., Bartolotta et al., 2011; Simacek et al., 2016; Urbanowicz et al., 2016) has shown eye-gaze to be an appropriate and more commonly used modality of communication for some individuals. Variations in how individuals can use an AAC device that would typically be activated using hands is also a possible approach (e.g., Kolb et al., 2023). Given the heterogeneity in expression of Rett syndrome, speech and motor abilities are critical characteristics to be considered when selecting an appropriate AAC modality (Amoako & Hare, 2020; Sigafoos et al., 1996, 2009; Simacek et al., 2016; Stasolla et al., 2014).
In a study by Simacek et al. (2016), the parents of two child participants with Rett syndrome used systematic, evidence-based instruction to teach participants to use AAC devices to request three different preferred items. One participant used a speech-generating device that required her to press symbols on a touch screen to make requests. The second participant used a Tobii that required her to eye-gaze toward symbols to make requests. The authors selected the devices based on the individual participants’ specific motor skills. More specifically, the participant who was taught to use the touch screen device was able to grasp, hold, press, pick up, and put down objects. In contrast, the participant who was taught to use the eye-gaze device could not use her hands to manipulate objects. Consideration of an individual’s motor abilities allows them to use a form of AAC they are physically capable of and that is the least restrictive for the individual.
In choosing appropriate AAC modalities for an individual, it is also worth considering how effectively they might be able to use various AAC modalities in a variety of settings and situations (Reichle et al., 2019). More specifically, different communication modalities may be easier to use for each individual and their communication partners in different situations. For example, due to portability, low-tech AAC (such as a communication book with symbols) may be more appropriate for an individual to use when out in the community. In contrast, a high-tech AAC device (such as a Tobii) may be more suitable to use at home, as it is less mobile and requires calibration with the user’s eye position for it to be functional. Such circumstances warrant the consideration of having multiple communication modalities available to utilize.
There are a variety of everyday scenarios that warrant the use of different communication modalities. For example, when in a crowded, noisy restaurant, gestures, rather than natural speech, may be more effective for gaining attention from others and communicating messages such as ordering food or asking for the bill. For individuals who use AAC, rather than using a device with speech output in a noisy restaurant, another option may be to use a communication book where they can point to or exchange symbols indicating their wants and needs. Having multiple communication modalities to use may also be beneficial when a device is inoperable or unavailable, such as if a high-tech AAC device is out for repair. In summary, just as those who use natural speech utilize a variety of modalities to communicate, such as gestures and written language, individuals who use limited or no natural speech can also benefit from having multiple communication modalities available to them. For individuals with Rett syndrome, teaching them to use more than one form of AAC, such as both a high-tech and a low-tech communication modality, may provide them the flexibility to use the modality that is easier to use, more accessible, or preferable in certain settings or situations. Furthermore, recent guidelines for how to manage communication needs of individuals with Rett syndrome developed by international groups of multidisciplinary stakeholders highly recommend providing access to multiple communication modalities, both high- and low-tech (Townend et al., 2020). Thus, we expect the utilization of multiple communication modalities in communication intervention for individuals with Rett syndrome to become more standard practice.
In one study by Stasolla et al. (2014), three participants with Rett syndrome were provided with instruction in the use of both the picture exchange communication system (PECS) (Frost & Bondy, 2002) and a speech generating device to request preferred items. All participants were provided with instruction for using PECS prior to instruction for using the speech generating device. After the participants learned to use both AAC modalities, researchers investigated levels of performance in using both modalities. All three participants exhibited comparable performance levels in using both their high- and low-tech AAC modalities. During the subsequent phase, investigators asked the participants to choose which modality they wanted to use prior to instruction. Two of the three participants demonstrated a preference and exclusively chose to use the speech generating device. In summary, all three participants acquired use of two forms of AAC to express communication, and two of the three participants exhibited preference for a particular AAC modality.
Previous literature has provided similar demonstrations with individuals with autism spectrum disorder (ASD) (e.g., Ganz et al., 2013; Son et al., 2006). In a study by Ganz et al. (2013), three children diagnosed with ASD, between the ages of 3 and 4 were taught PECS using an iPad with the PECS Phase III application following demonstration of mastery of PECS Phase III or IV using a communication book. During instruction, each participant was taught to request preferred foods or toys by touching symbols on the iPad. Symbols on the iPad were identical to those used in the communication book. After each child mastered utilizing the iPad to make requests, researchers assessed each child’s preference for the AAC modalities by presenting both modalities in front of the child to use to request preferred foods or toys. Researchers recorded occurrences of use of the modalities. Two of three participants chose to use the iPad more frequently than the communication book, whereas the third participant chose to use the communication book more frequently. The results demonstrated that two participants changed preference for AAC modalities from the communication book to the iPad after they learned to use both modalities; thus, at the conclusion of the study, all participants demonstrated the ability to acquire use of two different communication modalities and each participant demonstrated a modality preference.
Across studies investigating the use of AAC modalities with individuals with Rett syndrome, various low-, mid-, and high-tech modalities have been incorporated, such as speech generating technologies, including touch screen devices and Tobii with eye-gaze software, communication boards, microswitches, and picture exchange (e.g., Byiers et al., 2014; Sigafoos et al., 1996; Simacek et al., 2016, 2017; Stasolla et al., 2014; see Amoako & Hare, 2020; Sigafoos et al., 2009 for a review). Research findings have demonstrated that a range of AAC modalities can be appropriate for individuals with Rett syndrome; however, fewer studies exist that demonstrate the use of multiple AAC modalities by similar individuals.
The purpose of the current study was to investigate the use of high- and low-tech AAC modalities by three individuals with Rett syndrome who were given similar instruction. The following research question was addressed: For three individuals with Rett syndrome who received similar instruction in the use of two AAC modalities, one high-tech and one low-tech, what response patterns were observed in their use of each modality?
Method
This study is a companion to Girtler et al. (2023), which investigated the effects of systematic individualized instruction on page-linking skills of three individuals with Rett syndrome. Both studies shared the same participants, consent and recruitment procedures, and researchers. Both studies were conducted within the same time frame.
Participants and Setting
Three individuals, two girls and one woman diagnosed with Rett syndrome, and their parents, who were the interventionists, participated in the study. They were provided with intervention toward acquiring use of a high- and low-tech AAC modality. They resided in various locations in the United States and Canada. The parents were coached remotely by researchers from a telehealth lab associated with an R1 land-grant at the university. Participants were accepted into the study if they met the following criteria: (a) had a clinical diagnosis of Rett syndrome, (b) did not use vocal communication as a primary modality of communication, and (c) did not independently use high- and low-tech AAC modalities. Written informed consent to participate was obtained from the parents prior to the start of the study. None of the participants with Rett syndrome were able to provide written consent but did provide assent in the form of agreement to engage with the procedures. See Tables 1 and 2, respectively, for demographic information for the child participants and their parents.
Alice
Alice was a 3-year-old white girl with atypical Rett syndrome. Alice could walk independently, reach for and grasp both small and large items, and climb onto furniture. She also had an isolated point response with her index finger. She could eat by herself and play with toys requiring fine motor skills, such as Legos. Some of Alice’s highly preferred items and activities included milk, Play-Doh, and watching YouTube videos on her parent's cell phone. Alice exhibited several forms of idiosyncratic and unaided communication, such as three spoken words (i.e., all, no, book); word approximations (including mands); gestures; an approximated sign for MORE; shaking head to indicate yes/no responses; pointing; and looking at parents. Alice used a Wego as her high-tech AAC modality with TouchChat or Proloquo2Go software. For her low-tech AAC modality, she used a 3-ring binder with laminated symbols attached. Prior to the start of the study, Alice had experience with PECS for about 6 months but did not use it reliably. She received the Wego device at the beginning of the study. During instruction in use of high- and low-tech AAC communication modalities, Alice’s target communication involved symbol discrimination from an array and page-linking to make requests (Girtler et al., 2023). Alice's mother was the interventionist during the study. She did not have formal training in using the TouchChat and Proloquo2Go software prior to the start of the study.
Nina
Nina was a 19-year-old Asian woman. She was able to feed herself using her hands, use a cup for drinking, grasp small and large items, use an isolated point, and walk independently, with an occasional unsteady gait. She required assistance with self-care tasks. Her preferred food items were cookies, jellybeans, milk, and water. Her preferred activity was watching TV shows and movies. Nina communicated primarily through reaching and leading her parents to items or activities to gain assistance or access. She also engaged in vocalizations to gain attention and as a form of protest. Prior to the start of the study, Nina had experience with PECS on and off for 10 years, and inconsistently used Proloquo2Go on an iPad for 7 years. Her parents reported that she was exposed to these modalities but had not been taught how to use them reliably. She did not use either modality functionally to request preferred items. During the study, Nina used an iPad with the Proloquo2Go app as her high-tech AAC modality and a 3-ring binder with laminated symbols attached as her low-tech AAC modality. During instruction with her high- and low-tech AAC modalities, Nina’s target communication involved symbol discrimination from an array and page-linking to make requests (Girtler et al., 2023). Nina's parents were both present for sessions, with her father being the primary interventionist. Neither of Nina’s parents had formal training in using the Proloquo2Go app prior to the start of the study.
Courtney
Courtney was a 5-year-old white girl who could walk independently, grasp some items, and reliably reach for preferred items. She needed assistance drinking, eating, operating toys, and opening containers with preferred items inside, such as food or Play-Doh. Playing with toys and playing games with her sisters were identified as Courtney’s preferred activities. Cereal, blueberries, goldfish, cheese sticks, and water were identified as being some of her preferred foods. Courtney exhibited a variety of potentially communicative responses, such as using one word approximation, mama, reaching for items near her, and touching one of her mother's palms to indicate “yes” or “no”. Before starting the study, Courtney was able to request specific preferred food items in a field size of five using her Tobii i13 series with Snap Core First software. Courtney used the Tobii with Snap Core First software as her high-tech AAC modality and a 3-ring binder with laminated symbols attached as her low-tech AAC modality during the study. Prior to the start of the study, Courtney could not use either the Tobii or the communication book to page-link (i.e., choose a category symbol and subsequently a target symbol to request access to specific preferred items, activities, or actions). During instruction with her high- and low-tech AAC modalities, Courtney’s target communication involved page-linking to make requests (Girtler et al., 2023). Courtney's mother was the interventionist during the study. Prior to the start of the study, she had previous experience in operating a Tobii.
Setting
Approximately two to three, 30 min appointments were scheduled with each participant each week. During each appointment, researchers coached parents remotely via telehealth in running instructional sessions. Parents implemented instructional sessions within their homes. Researchers took data live while parents implemented instructional sessions.
Materials
Each participant used a high- and a low-tech AAC modality throughout the study. Prior to the study, each participant’s parent had already coordinated with their child’s local speech therapist to acquire the high-tech AAC device. Parents had the high-tech devices prior to the study; they were not asked to obtain these devices. Researchers provided the low-tech AAC materials (i.e., the communication books). For Nina and Courtney, the same symbols used for the high-tech AAC devices were also included for the low-tech AAC books. Nina used symbols generated from Proloquo2Go and Courtney used symbols generated from Snap Core First. Alice used symbols generated from TouchChat or Proloquo2Go on her high-tech AAC modality and from Boardmaker on her low-tech AAC modality.
Researchers and participants communicated via a HIPAA (Health Insurance Portability and Accountability Act)-approved video conferencing platform, either Google Meet or Zoom. Each family was provided with a unique Gmail account to communicate with researchers and login to the videoconferencing platform. A dedicated Dell OptiPlex 3010 Desktop computer with a Dell 24″ monitor was used by the researchers on campus. A Logitech HD Pro Webcam C920, a Polaroid 8″ Heavy Duty Mini Tripod, and a Logitech ClearChat Comfort/USB Headset H390 was used so that researchers could use video and sound when communicating with participants via videoconferencing. Sessions were videotaped using Debut Video Capture or Zoom software. All data and videos were stored on the university’s encrypted, secure server. In certain cases, such as during the COVID-19 pandemic, researchers conducted sessions off-campus. Researchers used a personal computer with built-in video camera and audio, connected through a university-based virtual private network (VPN) as a security measure, and used Google Meet or Zoom to communicate with participants. All data and videos were saved on the same secure university-based server. All videos were deleted from personal computers after they were uploaded to the secure server.
Most participants used personal communication technologies with cameras and microphones of their choice to communicate with researchers (e.g., laptops, iPads, desktops, and cell phones). For one participant, researchers mailed equipment to the family to borrow during the study.
Measures
For all participants, communicative requests involved completing a chain of responses that included selecting a category of preferred items or activities and then a specific preferred item or activity. For Alice and Nina, communicative requests were defined as using their pointer finger to select a symbol on the iPad or Wego (high-tech) and handing a picture exchange card to their parent (low-tech). For Courtney, requests were defined as activation of speech-output by the Snap Core First software using eye-gaze at symbols displayed on the Tobii for 0.8 s (high-tech) and eye-pointing toward symbols displayed on the communication book for 2 s (low-tech). During instructional sessions for all participants, researchers recorded requests as being accurate and independent, prompted, or incorrect. For all three participants, instructional sessions included five opportunities (trials) to make an independent and accurate request, except for a small number of Courtney and Nina’s sessions that included four or six trials. Participants met the performance criterion when they exhibited 80–100% accurate and independent requests across three consecutive sessions. Researchers calculated the number of sessions to criterion and cumulative number of trials with independent requests and used that data to provide descriptive information on each participant’s use of their high- and low-tech AAC modalities in the current paper.
Research Design
The current study is a descriptive study, aimed at investigating patterns of use of a high- and low-tech AAC modality during systematic instruction. Specifically, researchers investigated how long each participant took to learn use of each modality to make a request, as well as the relative growth in using each during instructional sessions. For more information on the research design used with each participant to demonstrate acquisition of each modality, see Girtler et al. (2023).
Procedures
Parents implemented all sessions in their home while researchers coached them remotely via telehealth. Prior to starting the first session, researchers provided parents with written instructions on how to implement the procedures. During sessions, researchers provided instructions and prompts as needed as well as performance feedback while parents implemented the procedures. Each session involved participants requesting one preferred item, activity, or action using either their high- or low-tech AAC modality. During sessions, researchers collected data via direct observation on the participants' use of the communication modalities. The current paper provides a broader description of the systematic instructional procedures for teaching use of high- and low-tech modalities to make requests across various target categories. For information on pre-intervention assessment and baseline procedures as well as detailed information on instructional procedures used with the participants to teach specific target requests, refer to Girtler et al. (2023).
Alice
Instruction with both the high- and low-tech AAC modalities occurred simultaneously, or within the same time frame/appointments. Independent and accurate requests for Alice using her high-tech AAC device consisted of using her finger on the Wego touch screen to: (a) choose a symbol that depicted a category of preferred items and activities (i.e., PLAY, FOOD, DRINK, PEOPLE), and (b) choose a symbol that indicated a specific preferred item or activity. Requests on her low-tech modality consisted of using her finger to touch cards to: (a) choose a symbol with the words I-WANT, and (b) choose a symbol indicating a preferred item or activity; thus, her parents taught her to discriminate among symbols and navigate to the page where the specific item or activity appeared.
Backward chaining and differential reinforcement with a 10 s prompt delay procedure were used to teach Alice to communicate requests using her high- and low-tech AAC modalities. During instructional trials, Alice was presented with a choice of a preferred activity or food, depending on naturally scheduled activities, such as breakfast time and play time. The preferred activity or food was present and out of reach. Either her high- or low-tech AAC modality was presented in front of Alice with the corresponding icon in the array. Following independent and accurate requests, Alice was provided 30 s access to the chosen item or activity. If Alice did not make a request within 10 s, her parent used a prompt to guide her to make a request. Prompting continued until Alice correctly made a request. She was then presented with the chosen item or activity and allowed 15 s of access.
Nina
Instruction with both the high- and low-tech AAC modalities occurred simultaneously, or within the same time frame/appointments. Independent and accurate requests for Nina using her high-tech AAC device consisted of using her finger on the ipad touch screen to: (a) choose a symbol that displayed the words “I want” with a vocal output, (b) choose a category symbol (i.e., FOOD, DRINK, TV SHOW), and (c) choose a symbol indicating a specific preferred item or activity within one of the categories. Requests on her low-tech modality consisted of using her hands to: (a) open her book, (b) flip to a category page (i.e., FOOD, DRINK, TV SHOW), and (c) select a symbol indicating a specific preferred item or activity; thus, her parents taught her to discriminate among symbols and navigate to the page where the specific item or activity appeared.
Forward chaining, total-task chaining, and discrimination training were used to teach Nina to communicate requests using her high- and low-tech AAC modalities. During instructional trials, Nina was presented with a drink choice, a food choice, or a TV remote (signaling choice of a TV show). Either Nina’s high- or low-tech AAC modality was presented in front of her displaying an array of icons corresponding to the chosen category. After presenting the items, Nina’s father asked “What do you want to eat/drink/watch?” Following independent and accurate requests, Nina was provided one bite of a chosen food item, one sip of a chosen drink, or 20 to 30 s access to a chosen activity. If Nina did not make a request within 5 s, or if she made an error, Nina’s father prompted her to make an accurate request. Prompting continued until Nina correctly made a request and was then presented with the chosen item or activity.
Courtney
Instruction began with the high-tech modality (Tobii). Independent and accurate requests for Courtney using her high-tech AAC device consisted of three steps: (a) eye-gaze toward a tab representing a general category of preferred items, activities, or actions (i.e., FOOD/DRINK, ATTENTION, HELP, TOYS, and GAMES/ACTIVITIES) for 0.8 s, (b) eye-gaze toward a second symbol within the category indicating whether she wanted food or drink (within the food/drink category) or indicating a desire to engage with an item, activity, or another person within the other four categories (i.e., ATTENTION!, “Help me open”, “I want to play a game”) for 0.8 s, and (c) eye-gaze toward a third symbol representing the specific item, activity, or action (i.e., “goldfish”, “Give me tickles”, “rockin' octopus”, “My turn”) for 0.8 s.
In the midst of instruction in the three-step process for requesting with the Tobii, it had to be sent for maintenance. While the Tobii was not available, the low-tech modality (communication book) with a two-step page-linking procedure to request preferred items, activities, and actions was taught. The two-step procedure required Courtney to: (a) eye-point for at least 2 consecutive seconds to a symbol representing a general category of preferred items, activities, or actions (i.e., FOOD/DRINK, ATTENTION, HELP, TOYS, and GAMES/ACTIVITIES), and (b) eye-point for at least 2 consecutive seconds to another symbol representing a specific item activity, or action (i.e., GOLDFISH, TICKLES, HELP-OPEN, ROCKIN’-OCTOPUS, MY-TURN). After observing Courtney make independent and accurate requests across categories using the communication book, the researchers and Courtney’s parent agreed that the two-step process of page-linking was a more efficient and streamlined process for Courtney to communicate wants and needs; thus, it was decided to target the same two steps on the Tobii upon its return.
A forward-chaining plus a prompt delay procedure was used to teach Courtney to communicate requests using her high- and low-tech AAC modalities. During instructional trials, Courtney was presented with either her high- or low-tech AAC modality displaying an icon representing the target category and, when applicable, having the target preferred item or activity present and out of reach. The target preferred item or activity was decided after presenting a choice between either two items, activities, and actions within a category or after a choice between two different categories followed by a choice between two specific items, activities, or actions. Courtney's parent would then say, “If you want __, you can ask for it on your device”, and wait for 0, 4, or 7 s (depending on the preset time delay) for her to make a request. Following independent and accurate requests, Courtney was provided one bite of a chosen food item, one sip of a chosen drink, or 20 to 30 s access to a chosen activity or action. If Courtney did not respond within 10 s, or if she made an error, Courtney’s parent prompted her to make an accurate request. Prompting continued until Courtney correctly made a request and was then presented with the chosen item, activity, or action.
Data Collection and Analysis
The primary focus of the current study was to investigate the use of high- and low-tech AAC modalities when exposed to similar instruction with both modalities. For the purposes of this investigation, researchers focused on the same category across both modalities: play for Alice, and food for Nina and Courtney. During instructional sessions, researchers recorded the percentage of independent and accurate requests exhibited by each participant. The number of sessions it took to reach performance criterion to make a specific request within a target category of preferred items/activities was calculated. This measure demonstrated how long it took to acquire the target skill using each modality. Additionally, using cumulative graphs for each participant, cumulative number of trials with independent requests within the same target category across instructional sessions using high- and low-tech AAC modalities were plotted. This measure demonstrated each participant’s relative growth in using each modality during instruction; thus, both number of sessions to criterion and cumulative number of trials with independent requests were used as descriptive data for investigating each participant’s use of their high- and low-tech AAC modality. Both measures revealed each participant’s idiosyncratic use of each modality during instruction.
Interobserver Agreement and Procedural Fidelity
Interobserver agreement (IOA) was measured for at least 33% of all instructional sessions for each participant using a trial-by-trial agreement method as described by Ledford and Gast (2018). Across all instructional sessions, the average percentage of IOA was 97%, r = 80%-100% for Alice; 96%, r = 60%-100% for Nina; and 93.29%, r = 75%-100% for Courtney.
Procedural fidelity measures were recorded for at least 33% of all sessions for each participant. Researchers recorded parent fidelity in implementing procedures through video recordings of the sessions. Measures included a task analysis of steps the parent needed to implement during sessions, which generally included pre-session exposure to a preferred item, activity, or action, and reinforcing or providing an additional prompt following a participant response. Across all sessions, the percentage of procedural fidelity accuracy averaged 99%, r = 95% -100% for Alice's mother; 96%, r = 66% -100% for Nina's father; and 96%, r = 80% -100% for Courtney's mother.
Results
Table 3 depicts the number of instructional sessions required to meet criterion using the high- and low-tech AAC modalities. Specifically, the current paper provides a report on the acquisition of one target communication request using a high- and low-tech AAC modality for each participant (play for Alice and food for Nina and Courtney).
Alice
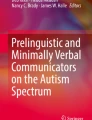
In acquiring use of her high- and low-tech AAC modalities, Alice required 20 sessions to reach criterion with the high-tech modality and 21 sessions to reach criterion with the low-tech modality; thus, Alice required one fewer session to acquire the request using the high-tech modality than the low-tech modality. Figure 1 depicts the cumulative number of trials with independent requests for play across instructional sessions until meeting criterion using the high- and low-tech AAC modalities for Alice. Altogether, the data depicted reflect instruction over a span of 10 weeks. During instruction with the high-tech AAC modality, Alice had 31 trials with independent requests across 20 instructional sessions, with an average gain of 1.55 independent requests per session. During instruction with the low-tech AAC modality, Alice had 65 trials with independent requests across 21 instructional sessions, with an average gain of 3.1 independent requests per session. Overall, Alice exhibited growth in making independent requests across instructional sessions using both modalities, with a higher average gain per session when using the low-tech modality during instruction.

High- and Low-tech Cumulative Number of Trials with Independent Requests for Alice
Nina
In acquiring use of her high- and low-tech AAC modalities, Nina required 54 sessions to reach criterion with the high-tech modality and 52 sessions to reach criterion with the low-tech modality; thus, Nina required two fewer sessions to acquire the request using the low-tech than the high-tech modality.
Figure 2 depicts the cumulative number of trials with independent requests for various food choices across instructional sessions until meeting criterion using the high- and low-tech AAC modalities for Nina. Altogether, the data depicted reflect instruction over a span of 27 weeks. During instruction with the high-tech AAC modality, Nina had 170 trials with independent requests across 56 instructional sessions, with an average gain of 3.04 independent requests per session. During instruction with the low-tech AAC modality, Nina had 180 trials with independent requests across 54 instructional sessions, with an average gain of 3.33 independent requests per session. Overall, Nina exhibited growth in making independent requests across instructional sessions using both modalities, with nearly identical average gains per session across the two modalities.

High- and Low-tech Cumulative Number of Trials with Independent Requests for Nina
Courtney
Unlike Alice and Nina, high- and low-tech modalities were taught sequentially for Courtney. The number of sessions to criterion for three-step page-linking on the high-tech modality was 28. Subsequently, the number of sessions to criterion for two-step page-linking on the low-tech modality was 16. Lastly, the number of sessions to criterion for two-step page-linking on the high-tech modality was six; thus, Courtney required fewer sessions to meet criterion for two-step page-linking on the low-tech modality following instruction for three-step page-linking on the high-tech modality. Subsequently, it took even fewer sessions to meet criterion upon the introduction of two-step page-linking on the high-tech modality.
Figure 3 depicts the cumulative number of trials with independent requests for food choices across instructional sessions until meeting criterion using the high- and low-tech AAC modalities for Courtney. Altogether, the data depicted reflect instruction over a span of 25 weeks. During instruction for the three-step process using the high-tech AAC modality, Courtney had 76 trials with independent requests across 28 instructional sessions, with an average gain of 2.71 independent requests per session. During instruction for the two-step process using the low-tech AAC modality, Courtney had 55 trials with independent requests across 16 instructional sessions, with an average gain of 3.44 independent requests per session. During instruction for the two-step process using the high-tech AAC modality, Courtney had 20 trials with independent requests across six instructional sessions, with an average gain of 3.33 independent requests per session; thus, following instruction for the three-step process using the high-tech AAC modality, Courtney exhibited a higher average gain during instruction for the two-step process on the low-tech AAC modality. Subsequently, she exhibited a comparable average gain during instruction for the two-step process on the high-tech AAC modality.

High- and Low-tech Cumulative Number of Trials with Independent Requests for Courtney
Discussion
General Discussion
The purpose of the current study was to investigate the use of high- and low-tech AAC modalities by three individuals with Rett syndrome given similar instruction for teaching both modalities. For Nina and Alice, the use of high- and low-tech AAC modalities during simultaneous instruction for both modalities was examined. For Courtney, the use of high- and low-tech AAC modalities during alternating instruction for both modalities was examined. Each participant demonstrated idiosyncratic responding across high- and low-tech AAC modalities during instruction, but ultimately demonstrated the ability to use both modalities to communicate requests for preferred items or activities.
Alice
During simultaneous instruction with her high- and low-tech AAC modalities, Alice exhibited idiosyncratic response patterns when acquiring the use of both modalities to communicate. Overall, Alice required relatively the same number of sessions to meet criterion on both modalities, requiring just one additional session to meet criterion on her low-tech AAC modality. Overall, she did exhibit a higher average gain of independent requests per session using her low-tech AAC modality; however, she still met the criterion for making independent requests on both her high- and low-tech modalities.
Nina
Like Alice, Nina exhibited idiosyncratic response patterns. She required relatively the same number of sessions to meet criterion on both AAC modalities, requiring just two additional sessions to meet criterion on her high-tech modality. She exhibited a comparable average gain of independent requests per session using both her low- and high-tech AAC modalities. Overall, Nina met criterion for making independent requests on both her high- and low-tech modalities, and merely needed more instructional sessions to meet criterion on her high-tech AAC modality. Of interest is that although Alice and Nina acquired the use of two communication modalities to make requests simultaneously, they exhibited idiosyncratic differences in how long it took them to acquire use of each modality and in their relative growth in acquiring each modality.
Courtney
Finally, Courtney also exhibited idiosyncratic response patterns when using her high- and low-tech AAC modalities during alternating instruction on each modality. Following instruction on her high-tech modality, she required fewer sessions to meet criterion on her low-tech AAC modality. Subsequently, following reintroduction of instruction on her high-tech modality, even fewer sessions were required to meet criterion. Additionally, she exhibited a higher average gain of independent requests per session during instruction for the two-step process using her low-tech and high-tech AAC modalities following instruction for the three-step process using her high-tech AAC modality. The following inferences can be drawn from these data: First, exposure to instruction on the high-tech AAC modality may have allowed Courtney to acquire the two-step process on her low-tech AAC modality within fewer instructional sessions. Subsequently, similar exposure may have allowed her to acquire the two-step process on her high-tech modality when reintroduced in even fewer sessions. Ultimately, as with Alice and Nina, Courtney acquired the use of both a high- and low-tech AAC modality to communicate requests.
The current study results provide important information regarding children with Rett syndrome and their potential communicative abilities and needs. First, it demonstrates the potential for individuals with Rett syndrome and complex communication needs to acquire the use of more than one AAC modality. Using systematic instruction that included prompts, reinforcement, and behavior chaining, Alice and Nina simultaneously learned to exchange symbols using a communication book and touch symbols displayed on a screen to make requests. Similarly, Courtney learned to use eye-gaze with symbols on a Tobii and subsequently eye-pointing with symbols on a communication book to make requests. Although all participants exhibited variations in how they acquired use of each modality, all three participants acquired the skills to use both AAC modalities to communicate. Because all three participants acquired use of two communication modalities, they now have the option of using either, depending on which is more suitable for a particular environment or their preference. Furthermore, as demonstrated in Courtney’s scenario, proficiency with more than one AAC modality can permit continued communication when one device needs to be repaired; thus, for individuals with Rett syndrome, it is worth considering teaching the use of more than one AAC modality (Townend et al., 2020), preferably modalities that are different in terms of their level of functionality in different environments or scenarios.
In comparing the results of the current study to those found in Stasolla et al. (2014), similar patterns were found regarding acquisition of two different communication modalities of different tech levels. In Stasolla et al. (2014), three participants were exposed to intervention to acquire the use of both PECS and a speech generating device to make requests. Next, researchers compared levels of requests exhibited by the participants when using PECS compared to the speech generating device. Although performance patterns in using the high- and low-tech AAC modalities varied for each participant, they all acquired the use of both AAC modalities and demonstrated similar performance levels using both. Overall, results found in both Stasolla et al. (2014) and the current study demonstrate the ability of individuals with Rett syndrome to acquire use of more than one communication modality as well as idiosyncrasies in terms of use of each modality during instruction.
Following the study, researchers had a discussion with each parent and asked them questions related to the level of ease their children had in using each of their AAC modalities, the modality they found their child was most successful in using to communicate, and the modality they envisioned their child using in the long-term. In terms of ease of use, two of three parents expressed that their child's high-tech AAC modality was moderately easy to use, and one parent expressed that their child's high-tech AAC modality was slightly easy to use. In contrast, two of three parents expressed that their child's low-tech AAC modality was slightly easy to use, and one parent expressed that their child's low-tech AAC modality was moderately easy to use. In terms of effective use, two of three parents reported that their child used their high-tech AAC modality more effectively when communicating with both the parent and other members of the community whereas one parent reported that their child used both her high- and low-tech AAC modality equally effectively when communicating. For the environment in which each AAC modality was most useful, all three parents reported that their child’s high-tech AAC modality was most useful at home and one parent reported that their child's high-tech AAC modality was most useful in school as well. In contrast, each parent reported different locations in which their child’s low-tech AAC modality was most useful, with one parent reporting that their child's low-tech modality was not any more useful to use in any setting, such as home, school, or out in the community. Finally, two of three parents reported that, in the long-term, they envisioned their child using their high-tech AAC modality alone whereas one parent reported that they envisioned their child using both her high- and low-tech AAC modalities in the long-term.
Although each individual’s preference toward certain communication modalities is arguably most important, parents or guardians of children with Rett syndrome may be one of the primary communication partners within their household and community, and therefore need to be able to be respond to communication produced by their child using AAC. Furthermore, parents or guardians may be responsible for setting up, adjusting, programming, transporting, and making minor repairs to their child’s AAC device(s). Therefore, parents or guardians may develop a perspective as to AAC modalities that their child is more successful in using generally or in certain situations; thus, teaching an individual with Rett syndrome more than one communication modality can provide them with a choice of modalities to use, and their parents can use their experiences to assist in helping their child develop an individualized system that allows for ease of communication with primary stakeholders in a variety of situations.
Clinical Implications
The idiosyncrasies demonstrated in terms of each participant’s use of their high- and low-tech AAC modalities provides potential implications for professionals who incorporate AAC modalities into their teaching or practice, such as clinicians or teachers. In the current study, all participants met criterion for using their high- and low-tech AAC modalities within a varied number of instructional sessions. Taking note of these results, it is worth considering that, when teaching individuals to use more than one AAC modality, they may not learn to use each modality at the same rate and performance may not look the same for both modalities at any given time during the instructional process. In summary, one can expect individual differences in how different AAC modality use is acquired. This is consistent with the guidelines published by Townend et al. (2020), suggesting individuals with Rett syndrome do not need to demonstrate a minimum level of performance with low-tech AAC before being introduced to high-tech AAC. Lastly, following mastery of different AAC modalities, practitioners may consider assessing the communicator’s preference for each modality, which may provide further insight as to the modality individuals prefer to use generally or in certain situations (Ringdahl et al., 2016; Stasolla et al., 2014; Son et al., 2006). Ideally, individuals should not only be able to use the AAC modality with which they are most proficient; they should have the freedom to use an AAC modality with which they are most comfortable and prefer to use under various conditions (e.g., at home, in the community).
Limitations and Future Directions
There are some limitations in the current study worth nothing. First, the current study is descriptive and does not demonstrate experimental control between instruction and acquisition of the high- and low-tech AAC modalities. The aim of the current paper was to evaluate the use of high- and low-tech AAC modalities, for the purpose of demonstrating potential considerations regarding teaching individuals with Rett syndrome multiple AAC modalities.
Second, one variable that may have influenced Alice and Nina’s acquisition of their low-tech AAC modality was their prior exposure to PECS before this investigation. Although Alice and Nina had previous exposure to PECS, they were not fluent with using the system prior to the current study. Lastly, another variable that may have influenced Alice's acquisition of her high-tech AAC modality was frequent changes in device software. As the family borrowed software to identify the most appropriate for her, two different and novel software packages were used during the study. The need to learn a new program with new symbols may have influenced the number of sessions required to meet performance criterion with the iPad.
Future research in the area of Rett syndrome and communication can help in understanding best practices in teaching individuals and to provide pathways for future practice. One possible pathway for future research may be to replicate similar methods conducted in the current study to determine whether similar patterns are observed with other individuals with Rett syndrome and whether there are other variables that should be considered when teaching and choosing AAC modalities. Like previous studies (e.g., Ganz et al., 2013; Stasolla et al., 2014; Son et al., 2006), future research should also use experimental methods to measure preference for specific AAC modalities. Using systematic methods to determine AAC modalities that an individual uses fluently, as well as to determine AAC modalities an individual prefers to use, can provide pertinent information and guidance in developing a complete AAC system for individuals.
Finally, unknown is the effect of a multi-component approach to communication in which caregivers target a variety of expressive communication functions beyond requests, such as commenting, asking questions, and expressing feelings, as well as receptive language through the use of systematic modeling of AAC for receptive language development.
Conclusion
The current study contributes to the small database that indicates individuals with Rett syndrome have the potential to acquire the use of more than one AAC modality. Taking into consideration mobility issues, functionality of different AAC modalities based on the environment, and the ease of use of different AAC modalities with caregivers and familiar communication partners can influence decisions on which modalities to teach. Acquiring multiple communication modalities that are highly preferred and used with minimal effort can give individuals with Rett syndrome or other developmental and intellectual disabilities the independence to communicate needs and preferences to others, the ability to express oneself, and decrease the likelihood of abandoning the use of AAC.
Data Availability
Data are available upon request from the first author.
References
Amir, R. E., & Zoghbi, H. Y. (2000). Retts syndrome: Methyl-CpG-binding protein 2 mutations and phenotype-genotype correlations. American Journal of Medical Genetics, 97, 147–152.
Amoako, A. N., & Hare, D. J. (2020). Non-medical interventions for individuals with Rett syndrome: A systematic review. Journal of Applied Research in Intellectual Disabilities, 33, 808–827. https://doi.org/10.1111/jar.12694
Bartolotta, T. E., Zipp, G. P., Simpkins, S. D., & Glazewski, B. (2011). Communication skills in girls with Rett Syndrome. Focus on Autism and Other Developmental Disabilities, 26, 15–24. https://doi.org/10.1177/1088357610380042
Byiers, B. J., Dimian, A., & Symons, F. J. (2014). Functional communication training in Rett syndrome: A preliminary study. American Journal on Intellectual and Developmental Disabilities, 119, 340–350. https://doi.org/10.1352/1944-7558-119.4.340
Ellaway, J., & Christodoulou, C. (2001). Rett syndrome: Clinical characteristics and recent genetic advances. Disability and Rehabilitation, 23. https://doi.org/10.1080/09638280150504171
Erlandson, A., & Hagberg, B. (2005). MECP2 abnormality phenotypes: Clinicopathologic area with broad variability. Journal of Child Neurology, 20, 727–732. https://doi.org/10.1177/08830738050200090501
Frost, L. A., & Bondy, A. S. (2002). The Picture exchange communication system training manual (2nd ed.). Pyramid Educational Products, Inc.
Ganz, J. B., Hong, E. R., & Goodwyn, F. D. (2013). Effectiveness of the PECS Phase III app and choice between the app and traditional PECS among preschoolers with ASD. Research in Autism Spectrum Disorders, 7, 973–983. https://doi.org/10.1016/j.rasd.2013.04.003
Ganz, J. B., Rispoli, M. J., Mason, R. A., & Hong, E. R. (2014). Moderation of effects of AAC based on setting and types of aided AAC on outcome variables: An aggregate study of single-case research with individuals with ASD. Developmental Neurorehabilitation, 17, 184–192. https://doi.org/10.3109/17518423.2012.748097
Girtler, S. N., Unholz-Bowden, E. K., Shipchandler, A., Kolb, R. L., & McComas, J. J. (2023). Use of augmentative and alternative communication by individuals with Rett syndrome part 1: Page-linking. Journal of Developmental and Physical Disabilities. https://doi.org/10.1007/s10882-023-09903-x
Hagberg, B. (1985). Rett’s syndrome: Prevalence and impact on progressive severe mental retardation in girls. Acta Paediatrica Scandinavica, 74, 405–408. https://doi.org/10.1111/j.16512227.1985.tb10993.x
Hagberg, B., & Zoghbi, H. Y. (2002). Clinical manifestations and stages of Rett syndrome. Mental Retardation and Developmental Disabilities Research Reviews, 8, 61–65. https://doi.org/10.1002/mrdd.10020
Hetzroni, O., Rubin, C., & Konkol, O. (2002). The use of assistive technology for symbol identification by children with Rett syndrome. Journal of Intellectual and Developmental Disability, 27, 57–71. https://doi.org/10.1080/13668250120119626-1
Kolb, R. L., McComas, J. J., Girtler S. N., Simacek, J., & Dimian, A. F., Unholz-Bowden, E. K., & Shipchandler, A. H. (2023). Teaching requesting to individuals with Rett syndrome using alternative augmentative communication (AAC) through caregiver coaching via telehealth. Journal of Developmental and Physical Disabilities. https://doi.org/10.1007/s10882-023-09894-9
Ledford, J. R., & Gast, D. L. (2018). Single case research methodology: Applications in special education and behavioral sciences. Routledge.
Mackay, J., Downs, J., Wong, K., Heyworth, J., Epstein, A., & Leonard, H. (2017). Autonomic breathing abnormalities in Rett syndrome: Caregiver perspectives in an international database study. Journal of Neurodevelopmental Disorders, 9, 15. https://doi.org/10.1186/s11689-017-9196-7
National Institute of Neurological Disorders and Stroke. (2023, January 20). Rett Syndrome. https://www.ninds.nih.gov/health-information/disorders/rett-syndrome?search-term=Rett
Neul, J. L., Kaufmann, W. E., Glaze, D. G., Christodoulou, J., Clarke, A. J., Bahi-Buisson, N., & Percy, A. K. (2010). Rett syndrome: Revised diagnostic criteria and nomenclature. Annals of Neurology, 68, 944–950. https://doi.org/10.1002/ana.22124
Reichle, J., Simacek, J., Wattanawongwan, S., & Ganz, J. (2019). Implementing aided augmentative communication systems with persons having complex communicative needs. Behavior Modification, 43, 841–878. https://doi.org/10.1177/0145445519858272
Ringdahl, J. E., Berg, W. K., Wacker, D. P., Ryan, S., Ryan, A., Crook, K., & Molony, M. (2016). Further demonstrations of individual preference among mand modalities during functional communication training. Journal of Developmental and Physical Disabilities, 28, 905–917. https://doi.org/10.1007/s10882-016-9518-9
Sigafoos, J., Green, V. A., Schlosser, R., O’Reilly, M. F., Lancioni, G. E., Rispoli, M., & Lang, R. (2009). Communication intervention in Rett syndrome: A systematic review. Research in Autism Spectrum Disorders, 3, 304–318. https://doi.org/10.1016/j.rasd.2008.09.006
Sigafoos, J., Laurie, S., & Pennell, D. (1996). Teaching children with Rett syndrome to request preferred objects using aided communication: Two preliminary studies. Augmentative and Alternative Communication, 12, 88–96. https://doi.org/10.1080/07434619612331277538
Simacek, J., Dimian, A., & McComas, J. (2017). Communication intervention for young children with severe neurodevelopmental disabilities via telehealth. Journal of Autism and Developmental Disorders, 47, 744–767. https://doi.org/10.1007/s10803-016-3006-z
Simacek, J., Reichle, J., & McComas, J. J. (2016). Communication intervention to teach requesting through aided AAC for two learners with Rett syndrome. Journal of Developmental and Physical Disabilities, 28, 59–81. https://doi.org/10.1007/s10882-015-9423-7
Son, S.-H., Sigafoos, J., O’Reilly, M., & Lancioni, G. E. (2006). Comparing two types of augmentative and alternative communication systems for children with autism. Pediatric Rehabilitation, 9(389), 395. https://doi.org/10.1080/13638490500519984
Stasolla, F., De Pace, C., Damiani, R., Di Leone, A., Albano, V., & Perilli, V. (2014). Comparing PECS and VOCA to promote communication opportunities and to reduce stereotyped behaviors by three girls with Rett syndrome. Research in Autism Spectrum Disorders, 8, 1269–1278. https://doi.org/10.1016/j.rasd.2014.06.009
Townend, G., Bartolotta, T., Urbanowicz, A., Wandin, H., & Curfs, L. (2020). Development of consensus-based guidelines for managing communication of individuals with Rett syndrome. Augmentative and Alternative Communication, 36, 71–81. https://doi.org/10.1080/07434618.2020.1785009
Urbanowicz, A., Downs, J., Girdler, S., Ciccone, N., & Leonard, H. (2016). An exploration of the use of eye gaze and gestures in females with Rett syndrome. Journal of Speech, Language, and Hearing Research, 59, 1373–1383. https://doi.org/10.1044/2015_jslhr-l-14-0185
Zappella, M., Meloni, I., Longo, I., Hayek, G., & Renieri, A. (2001). Preserved speech variants of the Rett syndrome: Molecular and clinical analysis. American Journal of Medical Genetics, 104, 14–22.
Funding
This study was funded by grant #1R21DC015021.
Author information
Authors and Affiliations
Contributions
All authors contributed toward research conceptualization, study design, and data analysis. Data collection was performed by Emily Unholz-Bowden, Shawn N. Girtler, Alefyah Shipchandler, and Rebecca L. Kolb. Emily Unholz-Bowden, Shawn N. Girtler, and Alefyah Shipchandler contributed toward writing. Editing was performed by Rebecca L. Kolb and Jennifer J. McComas.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethics Approval
This study was approved by the University of Minnesota’s Institutional Review Board. All ethics procedures and codes based on the Declaration of Helsinki, the Institutional Review Board, and the Behavior Analyst Certification Board Professional and Ethical Compliance Code for Behavior Analysts were followed during the study.
Consent to Participate
Written informed consent was obtained from a parent/legal guardian of each child participant.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Unholz-Bowden, E.K., Girtler, S.N., Shipchandler, A. et al. Use of Augmentative and Alternative Communication by Individuals with Rett Syndrome Part 2: High-Tech and Low-Tech Modalities. J Dev Phys Disabil 36, 147–167 (2024). https://doi.org/10.1007/s10882-023-09902-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10882-023-09902-y