
Abstract
Background
Effective pulmonary vein isolation (PVI) with cryoablation depends on adequate occlusion of pulmonary veins (PV) by the cryoballoon and is therefore likely to be affected by PV and left atrial (LA) anatomical characteristics and variants. Thus, the objective of this study was to investigate the effect of LA and PV anatomy, evaluated by computed tomography (CT), on acute and long-term outcomes of cryoablation for atrial fibrillation (AF).
Methods
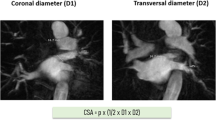
Fifty-eight patients (64.72 + 9.44 years, 60.3% male) undergoing cryoablation for paroxysmal or early persistent AF were included. Pre-procedural CT images were analyzed to evaluate LA dimensions and PV anatomical characteristics. Predictors of recurrence were identified using regression analysis.
Results
60.3% of patients had two PVs on each side with separate ostia, whereas 29.3% and 10.3% had right middle and left common PVs, respectively. The following anatomic characteristics were found to be independent predictors of recurrence: right superior PV ostial max:min diameter ratio > 1.32, left superior PV ostial max:min diameter ratio > 1.2, right superior PV antral circumference > 69.1 mm, right inferior PV antral circumference > 61.38 mm, right superior PV angle > 22.7°. Using these factors, LA diameter and right middle PV, a scoring model was created for prediction of “unfavorable” LA-PV anatomy (AUC = 0.867, p = 0.000009, score range = 0–7). Score of ≥ 4 predicted need for longer cryoenergy ablation (p = 0.039) and more frequent switch to radiofrequency energy (p = 0.066) to achieve PVI, and had a sensitivity of 83.3% and specificity of 82.5% to predict clinical recurrence.
Conclusion
CT-based scoring system is useful to identify “unfavorable” anatomy prior to cryo-PVI, which can result in procedural difficulty and poor outcomes.




Similar content being viewed by others


Abbreviations
- AF:
-
Atrial fibrillation
- AT:
-
Atrial tachycardia
- CT:
-
Computed tomography
- LA:
-
Left atrium
- PV:
-
Pulmonary vein
- RSPV:
-
Right superior pulmonary vein
- RIPV:
-
Right inferior pulmonary vein
- RMPV:
-
Right middle pulmonary vein
- LSPV:
-
Left superior pulmonary vein
- LIPV:
-
Left inferior pulmonary vein
- LCPV:
-
Left common pulmonary vein
References
Calkins H, Hindricks G, Cappato R, Kim YH, Saad EB, Aguinaga L, Akar JG, Badhwar V, Brugada J, Camm J, Chen PS, Chen SA, Chung MK, Nielsen JC, Curtis AB, Davies DW, Day JD, d’Avila A, de Groot NMS (N), di Biase L, Duytschaever M, Edgerton JR, Ellenbogen KA, Ellinor PT, Ernst S, Fenelon G, Gerstenfeld EP, Haines DE, Haissaguerre M, Helm RH, Hylek E, Jackman WM, Jalife J, Kalman JM, Kautzner J, Kottkamp H, Kuck KH, Kumagai K, Lee R, Lewalter T, Lindsay BD, Macle L, Mansour M, Marchlinski FE, Michaud GF, Nakagawa H, Natale A, Nattel S, Okumura K, Packer D, Pokushalov E, Reynolds MR, Sanders P, Scanavacca M, Schilling R, Tondo C, Tsao HM, Verma A, Wilber DJ, Yamane T 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation: Executive summary, EP Europace, 2–18; 20(1):157–208. https://doi.org/10.1093/europace/eux275.
Haissaguerre M, Jais P, Shah D, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998;339(10):659–66. https://doi.org/10.1056/NEJM199809033391003.
Pappone C, Rosanio S, Oreto G, Tocchi M, Gugliotta F, Vicedomini G, et al. Circumferential radiofrequency ablation of pulmonary vein ostia: a new anatomic approach for curing atrial fibrillation. Circulation. 2000;102(21):2619–28. https://doi.org/10.1161/01.CIR.102.21.2619.
Verma A, Jiang C, Betts TR, Chen J, Deisenhofer I, Mantovan R, et al. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med. 2015;372(19):1812–22. https://doi.org/10.1056/NEJMoa1408288.
Kuck KH, Brugada J, Fürnkranz A, Metzner A, Ouyang F, Chun KR, et al. Cryoballoon or radiofrequency ablation for paroxysmal atrial fibrillation. N Engl J Med. 2016;374:2235–45. https://doi.org/10.1056/NEJMoa1602014.
Chen J, Yang ZG, Xu HY, Shi K, Long QH, Guo YK. Assessments of pulmonary vein and left atrial anatomical variants in atrial fibrillation patients for catheter ablation with cardiac CT. Eur Radiol. 2017;27(2):660–70. https://doi.org/10.1007/s00330-016-4411-6.
Khoueiry Z, Albenque JP, Providencia R, Combes S, Combes N, Jourda F, et al. Outcomes after cryoablation vs. radiofrequency in patients with paroxysmal atrial fibrillation: impact of pulmonary veins anatomy. EP Europace. 2016;18(9):1343–51. https://doi.org/10.1093/europace/euv419.
McLellan AJ, Ling LH, Ruggiero D, et al. Pulmonary vein isolation: the impact of pulmonary venous anatomy on long-term outcome of catheter ablation for paroxysmal atrial fibrillation. Heart Rhythm. 2014;11(4):549–56. https://doi.org/10.1016/j.hrthm.2013.12.025.
Sohn C, Sohns JM, Bergau L, et al. Pulmonary vein anatomy predicts freedom from atrial fibrillation using remote magnetic navigation for circumferential pulmonary vein ablation. EP Europace. 2013;15(8):1136–42. https://doi.org/10.1093/europace/eut059.
den Uijl DW, Tops LF, Delgado V, Schuijf JD, Kroft LJM, de Roos A, et al. Effect of pulmonary vein anatomy and left atrial dimensions on outcome of circumferential radiofrequency catheter ablation for atrial fibrillation. Am J Cardiol. 2011;107(2):243–9. https://doi.org/10.1016/j.amjcard.2010.08.069.
Takarada K, Ströker E, Abugattas JP, de Regibus V, Coutiño HE, Lusoc I, et al. Impact of an additional right pulmonary vein on second-generation cryoballoon ablation for atrial fibrillation: a propensity matched score study. J Interv Card Electrophysiol. 2018;54(1):1–8. https://doi.org/10.1007/s10840-018-0373-8.
Huang SW, Jin Q, Zhang N, Ling TY, Pan WQ, Lin CJ, et al. Impact of pulmonary vein anatomy on long-term outcome of cryoballoon ablation for atrial fibrillation. Curr Med Sci. 2018;38:259–67. https://doi.org/10.1007/s11596-018-1874-5.
Shigeta T, Okishige K, Yamauchi Y, Aoyagi H, Nakamura T, Yamashita M, et al. Clinical assessment of cryoballoon ablation in cases with atrial fibrillation and a left common pulmonary vein. J Cardiovasc Electrophysiol. 2017;28:1021–7. https://doi.org/10.1111/jce.13267.
Ströker E, Takarada K, de Asmundis C, Abugattas JP, Mugnai G, Velagić V, et al. Second-generation cryoballoon ablation in the setting of left common pulmonary veins: procedural findings and clinical outcome. Heart Rhythm. 2017;14(9):1311–8. https://doi.org/10.1016/j.hrthm.2017.06.019.
Heeger CH, Tscholl V, Wissner E, et al. Acute efficacy, safety, and long-term clinical outcomes using the second-generation cryoballoon for pulmonary vein isolation in patients with a left common pulmonary vein: a multicenter study. Heart Rhythm. 2017;14:111–1118. https://doi.org/10.1002/clc.23163.
Guler E, Guler GB, Demir GG, et al. Effect of pulmonary vein anatomy and pulmonary vein diameters on outcome of cryoballoon catheter ablation for atrial fibrillation. Pacing Clin Electrophysiol. 2015;38:989–96. https://doi.org/10.1111/pace.12660.
Tsyganov A, Petru J, Skoda J, Sediva L, Hala P, Weichet J, et al. Anatomical predictors for successful pulmonary vein isolation using balloon-based technologies in atrial fibrillation. J Interv Card Electrophysiol. 2015;44:265–71. https://doi.org/10.1007/s10840-015-0068-3.
Knecht S, Kuhne M, Altmann D, et al. Anatomical predictors for acute and mid-term success of cryoballoon ablation of atrial fibrillation using the 28 mm balloon. J Cardiovasc Electrophysiol. 2013;24:132–8. https://doi.org/10.1111/jce.12003.
Kubala M, Hermida J, Nadji G, Quenum S, Traulle S, Jarry G. Normal pulmonary veins anatomy is associated with better AF-free survival after cryoablation as compared to atypical anatomy with common left pulmonary vein. Pacing Clin Electrophysiol. 2011;34:837–43. https://doi.org/10.1111/j.1540-8159.2011.03070.x.
Evranos B, Kocyigit D, Gurses KM, Yalcin MU, Sahiner ML, Kaya EB, et al. Increased left atrial pressure predicts recurrence following successful cryoablation for atrial fibrillation with second-generation cryoballoon. J Interv Card Electrophysiol. 2016;46:145–51. https://doi.org/10.1007/s10840-016-0107-8.
Aryana A, Mugnai G, Singh SM, et al. Procedural and biophysical indicators of durable pulmonary vein isolation during cryoballoon ablation of atrial fibrillation. Heart Rhythm. 2016;13(2):424–32. https://doi.org/10.1016/j.hrthm.2015.10.033.
Greiss H, Berkowitsch A, Wojcik M, et al. The impact of left atrial surface area and the second generation cryoballoon on clinical outcome of atrial fibrillation cryoablation. Pacing Clin Electrophysiol. 2015;38:815–24. https://doi.org/10.1111/pace.12637.
Thorning C, Hamadi M, Liaw JV, et al. CT evaluation of pulmonary venous anatomy variation in patients undergoing catheter ablation for atrial fibrillation. Clin Imaging. 2011;35(1):1–9. https://doi.org/10.1016/j.clinimag.2009.11.005.
Ströker E, de Asmundis C, Saitoh Y, Velagić V, Mugnai G, Irfan G, et al. Anatomic predictors of phrenic nerve injury in the setting of pulmonary vein isolation using the 28-mm second-generation cryoballoon. Heart Rhythm. 2016;13(2):342–51. https://doi.org/10.1016/j.hrthm.2015.10.017.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
The study was approved by the Institutional Review Board of our institution.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Vaishnav, A.S., Alderwish, E., Coleman, K.M. et al. Anatomic predictors of recurrence after cryoablation for atrial fibrillation: a computed tomography based composite score. J Interv Card Electrophysiol 61, 293–302 (2021). https://doi.org/10.1007/s10840-020-00799-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-020-00799-7