
Abstract
Purpose
To characterize alterations in pupillary light reflex responses in subjects following coronavirus disease 2019 (COVID-19), especially those with long-COVID.
Methods
Thirty-five subjects with previous COVID-19 and 30 healthy control participants were enrolled in this cross-sectional comparative study. An infrared dynamic pupillometry system (MonPack One; Metrovision, France) was used to quantify pupillary light responses. The National Institute for Health and Care Excellence (NICE) long-COVID questionnaire was used to identify persisting symptoms at least 4 weeks after acute COVID-19.
Results
The median time after the diagnosis of acute COVID-19 was 4.0 (2.0–5.0) months. There was an increase in the latency of pupil contraction (P = 0.001) and a reduction in the duration of pupil contraction (P = 0.039) in post-COVID-19 subjects compared to healthy controls. No significant differences were observed in the initial pupil diameter, amplitude and velocity of pupil contraction or latency, velocity and duration of pupil dilation. Long-COVID was present in 25/35 (71%) subjects and their duration of pupil contraction was reduced compared to subjects without long-COVID (P = 0.009). The NICE long-COVID questionnaire total score (ρ = − 0.507; P = 0.002) and neurological score (ρ = − 0.412; P = 0.014) correlated with the duration of pupil contraction and the total score correlated with the latency of dilation (ρ = − 0.352; P = 0.038).
Conclusion
Dynamic pupillometry reveals significant alterations in contractile pupillary light responses, indicative of parasympathetic dysfunction after COVID-19.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
During the acute phase of coronavirus disease 2019 (COVID-19), neurological manifestations involving the peripheral, central, and autonomic nervous systems have been reported, and in a proportion of patients, these symptoms and signs have been shown to persist following recovery [1, 2]. A guideline has been developed by the National Institute for Health and Care Excellence (NICE), Scottish Intercollegiate Guidelines Network (SIGN), and Royal College of General Practitioners (RCGP) for the diagnosis and management of long-COVID, defined as ‘signs and symptoms that develop during or following an infection consistent with COVID-19 and which continue for more than 4 weeks and are not explained by an alternative diagnosis’ [3]. It has been suggested that small fiber neuropathy may contribute to long-COVID [4], and we have recently demonstrated corneal nerve fiber loss in subjects with long-COVID [5].
Symptomatic autonomic neuropathy characterized by orthostatic hypotension, resting tachycardia, excessive sweating, erectile dysfunction and deficiency in ciliary accommodation has been reported in patients with COVID-19 [6,7,8]. Autonomic dysfunction has been confirmed with reports of impaired sudomotor function and abnormal heart rate variability in post-COVID-19 patients [9, 10].
Dynamic pupillometry can provide detailed quantification of pupillary light responses to assess dysautonomia in Alzheimer’s disease, Fabry disease, diabetes mellitus and multiple sclerosis [11,12,13,14,15]. We have utilized dynamic pupillometry to quantify pupillary light reflex responses and their association with long-COVID.
Materials and methods
Thirty-five subjects who had recovered from COVID-19 and 30 healthy control participants were included in this cross-sectional study undertaken at a university hospital. The study followed the principles of the Declaration of Helsinki and was approved by the Research Ethics Committee of the Necmettin Erbakan University. After detailed explanation of the study protocol, written informed consent was obtained from all participants. The diagnosis of COVID-19 infection was confirmed by reverse transcriptase-polymerase chain reaction (RT-PCR) assay of oropharyngeal and nasopharyngeal swabs. Exclusion criteria included diabetes mellitus or any other systemic disease that might cause autonomic neuropathy, a history of ocular surgery or trauma, and use of any topical or systemic medications that might influence pupillary responses. The long-COVID questionnaire developed by NICE, SIGN and the RCGP was used to identify ongoing symptoms more than 4 weeks after acute COVID-19 [5, 16]. This questionnaire comprises 28 items in nine domains (generalized, respiratory, neurological, cardiovascular, musculoskeletal, gastrointestinal, dermatological, psychological/psychiatric, and ear, nose and throat symptoms), with a total score ranging between 0 and 28. The neurological domain of this questionnaire consists of seven items, scoring from 0 to 7. Additionally, the Fibromyalgia Questionnaire (FM-Q) was used to identify additional symptoms including muscle pain and overlapping symptoms including headache, fatigue, depression/anxiety, irritable bowel, heartburn, bladder problems, waking up unrefreshed and cognitive issues, with a total score ranging between 0 and 26 [17].
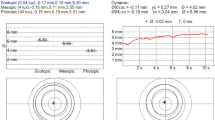
Quantitative pupillary light reflex measurements were undertaken using an infrared dynamic pupillometry system (MonPack One; Metrovision, France). Dynamic pupillary responses were elicited with white light flashes (light intensity 100 cd/m2, on/off time 200/3300 ms) and recorded with an infrared camera under near-infrared illumination (880 nm), which allows pupil parameters to be measured in complete darkness. Automated real-time image processing was performed, and pupil contours were outlined by the proprietary software of the device, with a measurement sensitivity of 0.01 mm. At least ten measurements were performed binocularly and the average values of the following eight parameters were automatically quantified: initial pupil diameter (mm), amplitude of pupil contraction (mm), duration of pupil contraction (ms), latency of pupil contraction (ms), velocity of pupil contraction (mm/s), latency of pupil dilation (ms), velocity of pupil dilation (mm/s), and duration of pupil dilation (ms) (Fig. 1). For all participants, the data obtained from the right eyes were included in the analyses.

Pupillary light reflex responses measured with dynamic pupillometry in a control participant (left), and a post-COVID-19 subject (right)
Statistical analyses were performed with SPSS 21.0 (SPSS for Windows, USA) software. Basic descriptive statistics were reported as the mean ± SD or median (interquartile range [IQR]), as appropriate. Normal distribution of continuous variables was confirmed with the Shapiro–Wilk test. Categorical parameters were compared using the Pearson χ2 test. Independent samples t test or Mann Whitney U test was used to compare parameters between post-COVID-19 patients and control participants. Kruskal–Wallis test followed by Dunn’s test with adjusted P values using Benjamini–Hochberg procedure or one-way ANOVA test followed by Tukey multiple comparison test were used to compare the parameters among the created subgroups. The associations between study variables were measured using Pearson’s correlation coefficient for parametric data and Spearman’s correlation coefficient for non-parametric data. For all evaluations, a two-sided P value of less than 0.05 was considered statistically significant.
Results
The mean age of post-COVID-19 subjects was 43.7 ± 11.5 years compared to 41.2 ± 9.6 years in the control group. No significant differences were observed between the two groups for age (P = 0.353) and gender (P = 0.565). The median (IQR) time from the diagnosis of acute COVID-19 was 4.0 (2.0–5.0) months. The median (IQR) values of the NICE questionnaire total and neurological scores, and FM-Q score beyond 4 weeks after acute infection were 3.0 (0–6.0), 0 (0–2.0), and 5.0 (2.0–10.0), respectively. During the acute phase of COVID-19, 21 subjects (60%) had no clinical signs of pneumonia, 10 (29%) had clinical signs of pneumonia not requiring oxygen support, 3 (9%) were hospitalized and received oxygen therapy, and 1 (3%) patient was admitted to the intensive care unit for the need of respiratory support.
Compared to controls, post-COVID-19 subjects had a longer latency (P = 0.001) and shorter duration (P = 0.039) of pupil contraction, with no significant difference in the initial pupil diameter, velocity and amplitude of pupil contraction, and latency, velocity and duration of pupil dilation (Table 1). At least one persisting symptom was present in 25/35 (71%) subjects, beyond 4 weeks after acute COVID-19 (defined as long-COVID). Subjects with and without long-COVID had longer latency of pupil contraction when compared to healthy controls (P = 0.012 and P = 0.010, respectively), but did not differ between subjects with and without long-COVID. However, the duration of pupil contraction was lower in subjects with compared to without long-COVID (P = 0.009) and healthy controls (P = 0.005). The latency of pupil dilation was also reduced in subjects with long-COVID compared to those without long-COVID (P = 0.014) (Table 2).
Sixteen of 35 subjects (46%) had at least one persisting neurological symptom beyond 4 weeks after acute COVID-19. The latency of pupil contraction was longer in subjects with and without persisting neurological symptoms compared to healthy controls (P = 0.016 and P = 0.010, respectively), but did not differ between subjects with and without neurological symptoms. The duration of pupil contraction was lower in subjects with neurological symptoms compared to controls (P = 0.008) (Table 3).
The total score on the NICE questionnaire correlated with the duration of contraction (ρ = − 0.507; P = 0.002) and latency of pupillary dilation (ρ = − 0.352; P = 0.038). The neurological score on the NICE questionnaire and FM-Q correlated with the duration of contraction (ρ = − 0.412; P = 0.014 and ρ = − 0.488; P = 0.003, respectively).
Discussion
This study shows evidence of increased latency and reduced duration of pupil contraction, indicative of parasympathetic dysfunction in subjects who have recovered from mild COVID-19. Furthermore, the severity of pupillary dysfunction was related to the number of persisting symptoms assessed by the NICE long-COVID questionnaire and FM-Q. These abnormalities are consistent with a growing body of literature suggesting that COVID-19 may be associated with autonomic dysfunction. Ghosh et al. [6] reported postural hypotension, constipation, intermittent profuse sweating and erectile dysfunction, preceding an acute motor axonal neuropathy in a patient with acute COVID-19. Umapathi et al. [7] described patients with acute COVID-19 who developed hyperhidrosis, orthostatic tachycardia and impaired pupillary accommodation. Abnormalities in quantitative sudomotor axon reflex testing, thermoregulatory sweat test, electrochemical skin conductance, and cardiovascular autonomic testing have been described in post-COVID-19 patients [9, 10, 18,19,20,21]. In a recent study by Shouman et al. [18], abnormalities in autonomic function tests were detected in 63% of patients during or after COVID-19, with the most common finding being orthostatic intolerance. The Composite Autonomic Symptom Scale 31 (COMPASS-31) questionnaire identified orthostatic intolerance, gastrointestinal, secretomotor and pupillomotor dysfunction in a cohort of 180 subjects with previous COVID-19 [22].
Quantitative evaluation of the pupillary light reflex enables relatively rapid evaluation of sympathetic and parasympathetic dysfunction. We have previously demonstrated a reduction in the amplitude and duration of pupillary contraction and latency of pupillary dilation in relation to the severity of autonomic symptoms based on the COMPASS 31 questionnaire in patients with Fabry disease [15]. Karahan et al. [23] reported an increase in resting pupil diameter as well as alterations in static and dynamic pupil parameters in subjects 1 month after COVID-19; but did not relate them to ongoing symptoms or presence of long-COVID. Abnormalities in accommodation, tonic pupil and the Holmes-Adie syndrome have also been described in people with COVID-19 [7, 24,25,26]. Vrettou et al. [27] hypothesized that the increase in pupil size and reduced pupillary light response in patients with COVID-19 may be an acute phenomenon with cytokine activation of the locus coeruleus and inhibitory signaling to the Edinger–Westphal nucleus. However, we now show altered pupillary responses, 4.0 months after acute COVID-19 characterized by a prolonged latency and a shorter duration of pupil contraction indicative of continuing parasympathetic dysfunction. Our findings could be attributed to the development of small fiber neuropathy associated with COVID-19 [4, 28,29,30]. Of note a possible ocular neurotropism has been hypothesized for SARS-CoV-2 [31,32,33]. We have recently shown a loss of corneal sub-basal nerve fibers, which are predominantly sensory but also contain autonomic nerves, and related it to the severity of long-COVID [5]. Long-COVID is defined as the persistence of symptoms at least 4 weeks after acute COVID-19 and post-COVID-19 syndrome when symptoms persist more than 12 weeks after acute infection [16]. Charfeddine et al. [34] suggested that long-COVID symptoms may be associated with an abnormal microcirculation and endothelial dysfunction and of course microvascular alterations may play a role in the pathogenesis of nerve damage [35]. Further investigation is needed to assess the role of microcirculatory dysfunction in the pathophysiology of altered pupillary responses in long-COVID.
A limitation of our study was the lack of a specific autonomic symptom questionnaire to assess the severity of dysautonomia. However, we used the NICE questionnaire and FM-Q to evaluate symptoms which evaluate some aspects of autonomic dysfunction. This study also assessed a relatively small sample size, and the cross-sectional study design precludes causal inferences.
In conclusion, we have utilized dynamic pupillometry to demonstrate predominantly parasympathetic pupillary dysfunction in post-COVID-19 patients. Dynamic pupillometry is relatively easy to perform and could be used to rapidly screen for autonomic dysfunction in patients with long-COVID.
Data availability
All anonymized data that support the findings of this study are available to any qualified researcher upon reasonable request to the corresponding author (ORCID: 0000–0002-0509–5649).
References
Roy D, Ghosh R, Dubey S, Dubey MJ, Benito-León J, Kanti Ray B (2021) Neurological and neuropsychiatric impacts of COVID-19 pandemic. Can J Neurol Sci 48:9–24. https://doi.org/10.1017/cjn.2020.173
Dani M, Dirksen A, Taraborrelli P et al (2021) Autonomic dysfunction in “long COVID”: rationale, physiology and management strategies. Clin Med (Lond) 21:e63–e67. https://doi.org/10.7861/clinmed.2020-0896
NICE Covid-19 rapid guideline: managing the long-term effects of COVID-19. https://www.nice.org.uk/guidance/ng188/chapter/4-Planning-care. Accessed 18 Dec 2020
Shiers S, Ray PR, Wangzhou A et al (2020) ACE2 and SCARF expression in human dorsal root ganglion nociceptors: implications for SARS-CoV-2 virus neurological effects. Pain 161:2494–2501. https://doi.org/10.1097/j.pain.0000000000002051
Bitirgen G, Korkmaz C, Zamani A et al (2021) Corneal confocal microscopy identifies corneal nerve fibre loss and increased dendritic cells in patients with long COVID. Br J Ophthalmol. https://doi.org/10.1136/bjophthalmol-2021-319450
Ghosh R, Roy D, Sengupta S, Benito-León J (2020) Autonomic dysfunction heralding acute motor axonal neuropathy in COVID-19. J Neurovirol 26:964–966. https://doi.org/10.1007/s13365-020-00908-2
Umapathi T, Poh MQW, Fan BE, Li KFC, George J, Tan JYL (2020) Acute hyperhidrosis and postural tachycardia in a COVID-19 patient. Clin Auton Res 30:571–573. https://doi.org/10.1007/s10286-020-00733-x
Moreno-Escobar MC, Kataria S, Khan E et al (2021) Acute transverse myelitis with dysautonomia following SARS-CoV-2 infection: a case report and review of literature. J Neuroimmunol 353:577523. https://doi.org/10.1016/j.jneuroim.2021.577523
Hinduja A, Moutairou A, Calvet JH (2021) Sudomotor dysfunction in patients recovered from COVID-19. Neurophysiol Clin 51:193–196. https://doi.org/10.1016/j.neucli.2021.01.003
Buchhorn R, Baumann C, Willaschek C (2020) Heart rate variability in a patient with coronavirus disease 2019. Int Cardiovasc Forum J 20:34–36. https://doi.org/10.17987/icfj.v20i0.685
Chougule PS, Najjar RP, Finkelstein MT, Kandiah N, Milea D (2019) Light-induced pupillary responses in Alzheimer’s disease. Front Neurol 10:360. https://doi.org/10.3389/fneur.2019.00360
de Seze J, Arndt C, Stojkovic T et al (2001) Pupillary disturbances in multiple sclerosis: correlation with MRI findings. J Neurol Sci 188:37–41. https://doi.org/10.1016/s0022-510x(01)00540-8
Bitirgen G, Akpinar Z, Turk HB, Malik RA (2021) Abnormal dynamic pupillometry relates to neurologic disability and retinal axonal loss in patients with multiple sclerosis. Transl Vis Sci Technol 10:30. https://doi.org/10.1167/tvst.10.4.30
Ferrari GL, Marques JL, Gandhi RA et al (2010) Using dynamic pupillometry as a simple screening tool to detect autonomic neuropathy in patients with diabetes: a pilot study. Biomed Eng Online 9:26. https://doi.org/10.1186/1475-925X-9-26
Bitirgen G, Turkmen K, Zengin N, Malik RA (2021) Altered pupillary light responses are associated with the severity of autonomic symptoms in patients with Fabry disease. Sci Rep 11:8146. https://doi.org/10.1038/s41598-021-87589-x
NICE ‘Long COVID’ guideline. https://www.guidelines.co.uk/infection/nice-long-covid-guideline/455728.article. Accessed 18 Dec 2020
At-Home Fibromyalgia Questionnaire. https://www.doctoroz.com/article/home-fibromyalgia-questionnaire. Accessed 22 Sept 2021
Shouman K, Vanichkachorn G, Cheshire WP et al (2021) Autonomic dysfunction following COVID-19 infection: an early experience. Clin Auton Res 31:385–394. https://doi.org/10.1007/s10286-021-00803-8
Barizien N, Le Guen M, Russel S, Touche P, Huang F, Vallée A (2021) Clinical characterization of dysautonomia in long COVID-19 patients. Sci Rep 11:14042. https://doi.org/10.1038/s41598-021-93546-5
Stute NL, Stickford JL, Province VM, Augenreich MA, Ratchford SM, Stickford ASL (2021) COVID-19 is getting on our nerves: sympathetic neural activity and haemodynamics in young adults recovering from SARS-CoV-2. J Physiol 599:4269–4285. https://doi.org/10.1113/JP281888
Kaliyaperumal D, Rk K, Alagesan M, Ramalingam S (2021) Characterization of cardiac autonomic function in COVID-19 using heart rate variability: a hospital based preliminary observational study. J Basic Clin Physiol Pharmacol 32:247–253. https://doi.org/10.1515/jbcpp-2020-0378
Buoite Stella A, Furlanis G, Frezza NA, Valentinotti R, Ajcevic M, Manganotti P (2021) Autonomic dysfunction in post-COVID patients with and without neurological symptoms: a prospective multidomain observational study. J Neurol. https://doi.org/10.1007/s00415-021-10735-y
Karahan M, Demirtaş AA, Hazar L et al (2021) Autonomic dysfunction detection by an automatic pupillometer as a non-invasive test in patients recovered from COVID-19. Graefes Arch Clin Exp Ophthalmol 259:2821–2826. https://doi.org/10.1007/s00417-021-05209-w
Ordás CM, Villacieros-Álvarez J, Pastor-Vivas AI, Corrales-Benítez Á (2020) Concurrent tonic pupil and trochlear nerve palsy in COVID-19. J Neurovirol 26:970–972. https://doi.org/10.1007/s13365-020-00909-1
Gopal M, Ambika S, Padmalakshmi K (2021) Tonic pupil following COVID 19. J Neuroophthalmol. https://doi.org/10.1097/WNO.0000000000001221
Kaya Tutar N, Kale N, Tugcu B (2021) Adie-Holmes syndrome associated with COVID-19 infection: a case report. Indian J Ophthalmol 69:773–774. https://doi.org/10.4103/ijo.IJO_3589_20
Vrettou CS, Korompoki E, Sarri K et al (2020) Pupillometry in critically ill patients with COVID-19: a prospective study. Clin Auton Res 30:563–565. https://doi.org/10.1007/s10286-020-00737-7
Oaklander AL (2020) Clinical significance of angiotensin-converting enzyme 2 receptors for severe acute respiratory syndrome coronavirus 2 (COVID-19) on peripheral small-fiber sensory neurons is unknown today. Pain 161:2431–2433. https://doi.org/10.1097/j.pain.0000000000002050
Odriozola A, Ortega L, Martinez L et al (2021) Widespread sensory neuropathy in diabetic patients hospitalized with severe COVID-19 infection. Diabetes Res Clin Pract 172:108631. https://doi.org/10.1016/j.diabres.2020.108631
Novak P (2020) Post COVID-19 syndrome associated with orthostatic cerebral hypoperfusion syndrome, small fiber neuropathy and benefit of immunotherapy: a case report. eNeurologicalSci 21:100276. https://doi.org/10.1016/j.ensci.2020.100276
Neri P, Pichi F (2020) COVID-19 and the eye immunity: lesson learned from the past and possible new therapeutic insights. Int Ophthalmol 40:1057–1060. https://doi.org/10.1007/s10792-020-01389-2
Neri P, Lamperti M, Pichi F (2020) SARS-COV-2 and eye immunity: the lesson was learned but we are not done yet. Brainstorming on possible pathophysiology inspired by ocular models. Int Ophthalmol 40:1879–1883. https://doi.org/10.1007/s10792-020-01495-1
Neri P, Pichi F (2021) SARS-CoV-2 and the eye: The Pandora’s box of ocular immunology. J Ocul Pharmacol Ther 37:502–509. https://doi.org/10.1089/jop.2021.0058
Charfeddine S, Ibn Hadj Amor H, Jdidi J et al (2021) Long COVID 19 syndrome: is it related to microcirculation and endothelial dysfunction? Insights from TUN-EndCOV study. Front Cardiovasc Med 8:745758. https://doi.org/10.3389/fcvm.2021.745758
Erdener ŞE, Dalkara T (2019) Small vessels are a big problem in neurodegeneration and neuroprotection. Front Neurol 10:889. https://doi.org/10.3389/fneur.2019.00889
Funding
The authors did not receive support from any organization for the submitted work.
Author information
Authors and Affiliations
Contributions
GB, CK, and RAM contributed to the conception and design of the study; GB, CK, AZ, HK and RAM contributed to acquisition and analysis of data; MSI performed statistical analyses; GB and CK contributed to drafting the text and preparing the figures; AZ, MSI, HK and RAM reviewed the draft, provided suggestions and improvements.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no financial or proprietary interests in any material discussed in this article.
Ethics approval
Approval was obtained from the ethics committee of Necmettin Erbakan University. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The preliminary findings of this study were presented as a poster at the Association for Research in Vision and Ophthalmology (ARVO) 2021 Imaging in the Eye Conference (May 13–14, 2021).
Rights and permissions
About this article

Cite this article
Bitirgen, G., Korkmaz, C., Zamani, A. et al. Abnormal quantitative pupillary light responses following COVID-19. Int Ophthalmol 42, 2847–2854 (2022). https://doi.org/10.1007/s10792-022-02275-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10792-022-02275-9