
Abstract
Purpose
To report a Rathke’s cleft cyst (RCC) presenting as unilateral incomplete cavernous sinus syndrome and disc edema
Method
Case report with literature review
Results
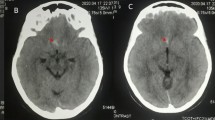
We present an 18-year-old girl who has been experiencing intermittent binocular diplopia for 1 month. Upon examination, the best corrected visual acuity was 20/20 (OU). Pronounced limitation of ocular motility with ptosis in her right eye was noted. Her pupil constricted normally. However, a relative afferent pupillary defect in the right eye was observed. Fundus examination showed disc edema in the right eye without peripapillary hemorrhage. Moreover, her thyroid function and acetylcholine receptor antibody levels were normal. Brain magnetic resonance imaging revealed a 1.6-cm mass at the suprasellar fossa and optic nerve sheath of right eye enhancement. She underwent transsphenoidal surgery, and pus-like formation was noted. Pathological findings were consistent with RCCs. After the cyst was removed, her ocular motility remarkably improved and ptosis subsided.
Conclusion
A case of RCC presenting as multiple cranial nerve palsy was reported. RCCs are benign and usually asymptomatic. Symptomatic RCCs often manifest as headache or visual problems, such as reduced visual acuity and visual field defect. Multiple cranial nerve involvement is uncommon and indicates inflammation or compression of the cavernous sinus and optic nerve. Neuropathy may resolve after surgery; therefore, surgery is indicated for symptomatic RCCs. Further, RCC should be included in the differential diagnosis of patients with disc edema.









Similar content being viewed by others


References
Teramoto A, Hirakawa K, Sanno N, Osamura Y (1994) Incidental pituitary lesions in 1,000 unselected autopsy specimens. Radiology 193(1):161–164
Trifanescu R, Ansorge O, Wass JA, Grossman AB, Karavitaki N (2012) Rathke’s cleft cysts. Clin Endocrinol 76(2):151–160
Odom JV, Bach M, Holder GE, McCulloch DL, Tormene AP (2016) ISCEV standard for clinical visual evoked potentials (2016 update). Doc Ophthalmol 133(1):1–9
Isono M, Kamida T, Kobayashi H, Shimomura T, Matsuyama J (2001) Clinical features of symptomatic Rathke’s cleft cyst. Clin Neurol Neurosurg 103(2):96–100
Kleinschmidt-DeMasters BK, Lillehei KO, Stears JC (1995) The pathologic, surgical, and MR spectrum of Rathke cleft cysts. Surg Neurol 44(1):19–26 discussion 26-7
Jung JE, Jin J, Jung MK, Kwon A, Chae HW, Kim DH, Kim HS (2017) Clinical manifestations of Rathke’s cleft cysts and their natural progression during 2 years in children and adolescents. Ann Pediatr Endocrinol Metab 22(3):164–169
Kim E (2012) Symptomatic Rathke cleft cyst: clinical features and surgical outcomes. World Neurosurg 78(5):527–534
Voelker JL, Campbell RL, Muller J (1991) Clinical, radiographic, and pathological features of symptomatic Rathke’s cleft cysts. J Neurosurg 74(4):535–544
Han SJ, Rolston JD, Jahangiri A, Aghi MK (2014) Rathke’s cleft cysts: review of natural history and surgical outcomes. J Neurooncol 117(2):197–203
Bohnstedt BN, Patel NB, Hagen MC, Fulkerson DH (2012) Acute, monocular vision loss from Rathke’s cleft cyst. J Clin Neurosci 19(6):904–906
Yum HR, Jang J, Shin SY, Park SH (2015) Rathke cleft cyst presenting as unilateral progressive oculomotor nerve palsy. Can J Ophthalmol 50(2):e31–e33
Park BH, Choi YC, Kim WJ, Han SH (2004) Transient isolated trochlear nerve palsy associated with Rathke’s cleft cyst. Yonsei Med J 45(1):166–168
Miyajima Y, Oka H, Utsuki S, Kondo K, Sato K, Fujii K (2007) Symptomatic Rathke’s cleft cyst with cavernous sinus syndrome. Neurol Med Chir (Tokyo) 47(12):576–578
Grover V, Hamrahian AH, Prayson RA, Weil RJ (2011) Rathke’s cleft cyst presenting as bilateral abducens nerve palsy. Pituitary 14(4):395–399
Pawar SJ, Sharma RR, Lad SD, Dev E, Devadas RV (2002) Rathke’s cleft cyst presenting as pituitary apoplexy. J Clin Neurosci 9(1):76–79
Kobayashi N, Oshitari T, Kobayashi K, Onoda T, Ikeda H, Adachi-Usami E (2014) Optic neuritis caused by Rathke’s cleft cyst in young adult. Case Rep Ophthalmol Med 2014:204762
Roncaroli F, Bacci A, Frank G, Calbucci F (1998) Granulomatous hypophysitis caused by a ruptured intrasellar Rathke’s cleft cyst: report of a case and review of the literature. Neurosurgery 43(1):146–149
Nishikawa T, Takahashi JA, Shimatsu A, Hashimoto N (2007) Hypophysitis caused by Rathke’s cleft cyst. Case report. Neurol Med Chir (Tokyo) 47(3):136–139
Komatsu F, Tsugu H, Komatsu M, Sakamoto S, Oshiro S, Fukushima T, Nabeshima K, Inoue T (2010) Clinicopathological characteristics in patients presenting with acute onset of symptoms caused by Rathke’s cleft cysts. Acta Neurochir (Wien) 152(10):1673–1678
Go JL, Rajamohan AG (2017) Imaging of the sella and parasellar region. Radiol Clin North Am 55(1):83–101
Shin JL, Asa SL, Woodhouse LJ, Smyth HS, Ezzat S (1999) Cystic lesions of the pituitary: clinicopathological features distinguishing craniopharyngioma, Rathke’s cleft cyst, and arachnoid cyst. J Clin Endocrinol Metab 84(11):3972–3982
Midha R, Jay V, Smyth HS (1991) Transsphenoidal management of Rathke’s cleft cysts A clinicopathological review of 10 cases. Surg Neurol 35(6):446–454
Nishioka H, Haraoka J, Izawa H, Ikeda Y (2006) Magnetic resonance imaging, clinical manifestations, and management of Rathke’s cleft cyst. Clin Endocrinol (Oxf) 64(2):184–188
Chotai S, Liu Y, Pan J, Qi S (2015) Characteristics of Rathke’s cleft cyst based on cyst location with a primary focus on recurrence after resection. J Neurosurg 122(6):1380–1389
Karavitaki N, Scheithauer BW, Watt J, Ansorge O, Moschopoulos M, Llaguno AV, Wass JA (2008) Collision lesions of the sella: co-existence of craniopharyngioma with gonadotroph adenoma and of Rathke’s cleft cyst with corticotroph adenoma. Pituitary 11(3):317–323
Hofmann BM, Kreutzer J, Saeger W, Buchfelder M, Blumcke I, Fahlbusch R, Buslei R (2006) Nuclear beta-catenin accumulation as reliable marker for the differentiation between cystic craniopharyngiomas and rathke cleft cysts: a clinico-pathologic approach. Am J Surg Pathol 30(12):1595–1603
Trifanescu R, Stavrinides V, Plaha P, Cudlip S, Byrne JV, Ansorge O, Wass JA, Karavitaki N (2011) Outcome in surgically treated Rathke’s cleft cysts: long-term monitoring needed. Eur J Endocrinol 165(1):33–37
Megdiche-Bazarbacha H, Ben Hammouda K, Aicha AB, Sebai R, Belghith L, Khaldi M, Touibi S (2006) Intrasphenoidal rathke cleft cyst. AJNR Am J Neuroradiol 27(5):1098–1100
Zada G (2011) Rathke cleft cysts: a review of clinical and surgical management. Neurosurg Focus 31(1):E1
Aho CJ, Liu C, Zelman V, Couldwell WT, Weiss MH (2005) Surgical outcomes in 118 patients with Rathke cleft cysts. J Neurosurg 102(2):189–193
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Informed consent
Written informed consent was obtained from the patient for publication of this case report, including accompanying images.
Statement of human rights and ethical approval
All procedures involving human participants were conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Statement on the welfare of animals
All applicable international, national, and/or institutional guidelines for the care and use of animals were followed.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Chang, C.F., Chen, Y.M. Rathke’s cleft cyst presenting as incomplete cavernous sinus syndrome and disc edema: a case report with literature review. Doc Ophthalmol 140, 55–65 (2020). https://doi.org/10.1007/s10633-019-09713-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10633-019-09713-7