
Abstract
Background
Lynch syndrome is the most common cause of hereditary colorectal cancer (CRC) and confers increased risk of other cancers. Identification of patients improves morbidity and mortality. Screening tumors for absent mismatch repair (MMR) protein expression by immunohistochemistry (IHC) is a recommended approach. Despite guidelines advocating universal screening, significant variation in clinical practice exists.
Aims/Methods
A retrospective study of two different IHC-based Lynch syndrome screening protocols at an urban, university hospital was performed. Outcomes from a “selective” screening strategy utilized from August 2007–July 2010 on CRC tumors from patients with high-risk features were compared with a “universal” strategy of screening all CRC tumors from July 2010–August 2013. Positively screened patients were referred for genetic counseling and offered germline testing.
Results
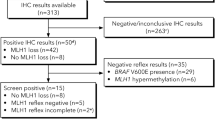
A total of 392 patients with CRC were screened: 107 selectively and 285 universally. The prevalence of Lynch syndrome was 3.1 %, with no difference by strategy. There was a trend (p = 0.06) toward fewer universally screened patients agreeing to genetic counseling compared with those selectively screened. Selective criteria failed to identify one of eight cases of Lynch syndrome from the universal group, though the universal strategy screened 166 additional tumors to find this additional patient.
Conclusions
Selective screening for Lynch syndrome has similar outcomes as universal screening in terms of identifying Lynch syndrome, despite screening far fewer patients. In addition, fewer eligible patients in our study agreed to undergo genetic counseling and germline testing than in prior studies. These lower rates may better reflect uptake of these services in clinical practice.
Similar content being viewed by others


References
Umar A, Boland CR, Terdiman JP, et al. Revised bethesda guidelines for hereditary nonpolyposis colorectal cancer (lynch syndrome) and microsatellite instability. J Natl Cancer Inst. 2004;96:261–268.
Vasen HF, Watson P, Mecklin JP, et al. New clinical criteria for hereditary nonpolyposis colorectal cancer (hnpcc, lynch syndrome) proposed by the international collaborative group on hnpcc. Gastroenterology. 1999;116:1453–1456.
Lynch HT, de la Chapelle A. Hereditary colorectal cancer. N Engl J Med. 2003;348:919–932.
Bonadona V, Bonaiti B, Olschwang S, et al. Cancer risks associated with germline mutations in mlh1, msh2, and msh6 genes in lynch syndrome. JAMA. 2011;305:2304–2310.
Hampel H, Frankel WL, Martin E, et al. Screening for the lynch syndrome (hereditary nonpolyposis colorectal cancer). N Engl J Med. 2005;352:1851–1860.
Aaltonen LA, Salovaara R, Kristo P, et al. Incidence of hereditary nonpolyposis colorectal cancer and the feasibility of molecular screening for the disease. N Engl J Med. 1998;338:1481–1487.
Barnetson RA, Tenesa A, Farrington SM, et al. Identification and survival of carriers of mutations in DNA mismatch-repair genes in colon cancer. N Engl J Med. 2006;354:2751–2763.
Salovaara R, Loukola A, Kristo P, et al. Population-based molecular detection of hereditary nonpolyposis colorectal cancer. J Clin Oncol. 2000;18:2193–2200.
Ward RL, Hicks S, Hawkins NJ. Population-based molecular screening for lynch syndrome: implications for personalized medicine. J Clin Oncol. 2013;31:2554–2562.
Moreira L, Balaguer F, Lindor N, et al. Identification of lynch syndrome among patients with colorectal cancer. JAMA. 2012;308:1555–1565.
Jarvinen HJ, Aarnio M, Mustonen H, et al. Controlled 15-year trial on screening for colorectal cancer in families with hereditary nonpolyposis colorectal cancer. Gastroenterology. 2000;118:829–834.
Schmeler KM, Lynch HT, Chen LM, et al. Prophylactic surgery to reduce the risk of gynecologic cancers in the lynch syndrome. N Engl J Med. 2006;354:261–269.
Lindor NM, Petersen GM, Hadley DW, et al. Recommendations for the care of individuals with an inherited predisposition to lynch syndrome: a systematic review. JAMA. 2006;296:1507–1517.
Gibson J, Lacy J, Matloff E, et al. Microsatellite instability testing in colorectal carcinoma: a practical guide. Clin Gastroenterol Hepatol. 2014;12:e171.
Aaltonen LA, Peltomaki P, Mecklin JP, et al. Replication errors in benign and malignant tumors from hereditary nonpolyposis colorectal cancer patients. Cancer Res. 1994;54:1645–1648.
Terdiman JP, Gum JR Jr, Conrad PG, et al. Efficient detection of hereditary nonpolyposis colorectal cancer gene carriers by screening for tumor microsatellite instability before germline genetic testing. Gastroenterology. 2001;120:21–30.
Hampel H, Frankel WL, Martin E, et al. Feasibility of screening for lynch syndrome among patients with colorectal cancer. J Clin Oncol. 2008;26:5783–5788.
Terdiman JP. It is time to get serious about diagnosing lynch syndrome (hereditary nonpolyposis colorectal cancer with defective DNA mismatch repair) in the general population. Gastroenterology. 2005;129:741–744.
Mvundura M, Grosse SD, Hampel H, et al. The cost-effectiveness of genetic testing strategies for lynch syndrome among newly diagnosed patients with colorectal cancer. Genet Med. 2010;12:93–104.
Pinol V, Castells A, Andreu M, et al. Accuracy of revised bethesda guidelines, microsatellite instability, and immunohistochemistry for the identification of patients with hereditary nonpolyposis colorectal cancer. JAMA. 2005;293:1986–1994.
Schofield L, Watson N, Grieu F, et al. Population-based detection of lynch syndrome in young colorectal cancer patients using microsatellite instability as the initial test. Int J Cancer. 2009;124:1097–1102.
Ladabaum U, Wang G, Terdiman J, et al. Strategies to identify the lynch syndrome among patients with colorectal cancer: a cost-effectiveness analysis. Ann Int Med. 2011;155:69–79.
Evaluation of Genomic Applications in P, Prevention Working G. Recommendations from the egapp working group: genetic testing strategies in newly diagnosed individuals with colorectal cancer aimed at reducing morbidity and mortality from lynch syndrome in relatives. Genet Med. 2009;11:35–41.
Burt RW, Cannon JA, David DS, et al. Colorectal cancer screening. J Natl Compr Cancer Netw JNCCN.. 2013;11:1538–1575.
Beamer LC, Grant ML, Espenschied CR, et al. Reflex immunohistochemistry and microsatellite instability testing of colorectal tumors for lynch syndrome among us cancer programs and follow-up of abnormal results. J Clin Oncol. 2012;30:1058–1063.
Cohen SA. Current lynch syndrome tumor screening practices: a survey of genetic counselors. J Genet Couns. 2014;23:38–47.
Bessa X, Balleste B, Andreu M, et al. A prospective, multicenter, population-based study of braf mutational analysis for lynch syndrome screening. Clin Gastroenterol Hepatol. 2008;6:206–214.
Heald B, Plesec T, Liu X, Pai R, et al. Implementation of universal microsatellite instability and immunohistochemistry screening for diagnosing lynch syndrome in a large academic medical center. J Clin Oncol. 2013;31:1336–1340.
Gritz ER, Peterson SK, Vernon SW, et al. Psychological impact of genetic testing for hereditary nonpolyposis colorectal cancer. J Clin Oncol. 2005;23:1902–1910.
Sharaf RN, Myer P, Stave CD, et al. Uptake of genetic testing by relatives of lynch syndrome probands: a systematic review. Clin Gastroenterol Hepatol. 2013;11:1093–1100.
Cross DS, Rahm AK, Kauffman TL, et al. Underutilization of lynch syndrome screening in a multisite study of patients with colorectal cancer. Genet Med. 2013;15:933–940.
Chubak B, Heald B, Sharp RR. Informed consent to microsatellite instability and immunohistochemistry screening for lynch syndrome. Genet Med. 2011;13:356–360.
Williams JL, Williams MS. Informed consent and immunohistochemistry screening for lynch syndrome. Genet Med. 2011;13:848–849.
Ladabaum U, Ford JM. Lynch syndrome in patients with colorectal cancer: finding the needle in the haystack. JAMA.. 2012;308:1581–1583.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kidambi, T.D., Blanco, A., Myers, M. et al. Selective Versus Universal Screening for Lynch Syndrome: A Six-Year Clinical Experience. Dig Dis Sci 60, 2463–2469 (2015). https://doi.org/10.1007/s10620-014-3234-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-014-3234-z