
Abstract
Background
Introduction of biologic agents in inflammatory bowel disease (IBD) has increased the likelihood of disease remission. Despite resolution of active inflammation, a subset of IBD patients report persistent defecatory symptoms.
Aim
To evaluate a group of patients with inflammatory bowel disease with suspected functional defecatory disorders, by use of anorectal manometric testing and subsequent biofeedback therapy.
Methods
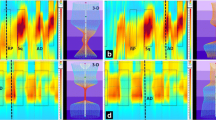
A group of IBD patients with persistent defecatory problems despite clinical improvement were included in this study. These patients had no evidence of left-sided disease. Endoscopic and radiographic study findings and timing in relation to the manometry study were recorded. Anorectal manometry was performed by the standard protocol and included rectal sensory assessment, ability to expel a balloon, and pressure dynamics with simulated defecation.
Results
Thirty IBD patients (Crohn’s 23 patients; ulcerative colitis six patients) presented with defecatory disorders including constipation (67 %) increased stooling (10 %), and rectal urgency and/or incontinence and rectal pain (6 %). All but one patient had anorectal manometric criteria of dyssynergia (presence of anismus motor pattern and inability to expel the balloon). Of the patients who completed biofeedback therapy, 30 % had a clinically significant (≥7-point) improvement in SIBDQ score, with a reduction in health-care utilization after a six-month period (p = 0.02).
Conclusions
Despite remission, some inflammatory bowel disease patients have persistent defecatory symptoms. Defecatory symptoms may not be predictive of an underlying inflammatory disorder. Lack of inflammatory activity and absence of left-sided disease should prompt investigation of functional disorders. Anorectal manometric testing and biofeedback therapy for patients with a diagnosis of dyssynergia may be a useful therapy.


Similar content being viewed by others

References
Farthing MJ, Lennard-jones JE. Sensibility of the rectum to distension and the anorectal distension reflex in ulcerative colitis. Gut. 1978;19:64–69.
Denis P, Colin R, Galmiche JP, et al. Elastic properties of the rectal wall in normal adults and in patients with ulcerative colitis. Gastroenterology. 1979;77:45–48.
Buchmann P, Mogg GA, Alexander-Williams J, Allan RN, Keighley MR. Relationship of proctitis and rectal capacity in Crohn’s disease. Gut. 1980;21:137–140.
Chrysos E, Athanasakis E, Tsiaoussis J, Zoras O, et al. Rectoanal motility in Crohn’s disease patients. Dis Colon Rectum. 2001;44:1509–1513.
Annese V, Bassotti G, Napolitano G, Usai P, Andriulli A, Vantrappen G. Gastrointestinal motility disorders in patients with inactive Crohn’s disease. Scand J Gastroenterol. 1997;32:1107–1117.
Andersson P, Olaison G, Hallböök O, Boeryd B, Sjödahl R. Increased anal resting pressure and rectal sensitivity in Crohn’s disease. Dis Colon Rectum. 2003;46:1685–1689.
Mueller MH, Kreis ME, Gross ML, Becker HD, Zittel TT, Jehle EC. Anorectal functional disorders in the absence of anorectal inflammation in patients with Crohn’s disease. Br J Surg. 2002;89:1027–1031.
Rao SS, Welcher KD, Happel J. Can biofeedback therapy improve anorectal function in fecal incontinence? Am J Gastroenterol. 1996;91:2360–2366.
Rao SS, Welcher KD, Leistikow JS. Obstructive defecation: a failure of rectoanal coordination. Am J Gastroenterol. 1998;93:1042–1050.
Harvey RF, Bradshaw JM. A simple index of Crohn’s-disease activity. Lancet. 1980;1:514.
Walmsley RS, Ayres RC, Pounder RE, Allan RN. A simple clinical colitis activity index. Gut. 1998;1:29–33.
Rao SS, Hatfield R, Soffer E, Rao S, Beaty J, Conklin JL. Manometric tests of anorectal function in healthy adults. Am J Gastroenterol. 1999;94:773–783.
Bharucha AE, Wald A, Enck P, Rao S. Functional anorectal disorders. Gastroenterology. 2006;130:1510.
Irvine EJ, Zhou Q, Thompson AK. The Short Inflammatory Bowel Disease Questionnaire: a quality of life instrument for community physicians managing inflammatory bowel disease. CCRPT Investigators. Canadian Crohn’s Relapse Prevention Trial. Am J Gastroenterol. 1996;91:1571–1578.
Simren M, Axelsson J, Gillberg R, Abrahamsson H, Svedlund J, Björnsson ES. Quality of life in inflammatory bowel disease in remission: the impact of IBS-like symptoms and associated psychological factors. Am J Gastroentrol. 2002;97:389–396.
Minderhoud IM, Oldenburg B, Wismeijer JA, van Berge Henegouwen GP, Smout AJ. IBS-like symptoms in patients with inflammatory bowel disease in remission; relationships with quality of life and coping behavior. Dig Dis Sci. 2004;49:469–474.
Farrokhyar F, Marshall JK, Easterbrook B, Irvine EJ. Functional gastrointestinal disorders and mood disorders in patients with inactive inflammatory bowel disease: prevalence and impact on health. Inflamm Bowel Dis. 2006;12:38–46.
Chiarioni G, Whitehead WE, Pezza V, Morelli A, Bassotti G. Biofeedback is superior to laxatives for normal transit constipation due to pelvic floor dyssynergia. Gastroenterology. 2006;130:657–664.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Perera, L.P., Ananthakrishnan, A.N., Guilday, C. et al. Dyssynergic Defecation: A Treatable Cause of Persistent Symptoms When Inflammatory Bowel Disease Is in Remission. Dig Dis Sci 58, 3600–3605 (2013). https://doi.org/10.1007/s10620-013-2850-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-013-2850-3