
Abstract
Background
Little is known about the factors that predict clinical relapse in Crohn’s disease patients receiving thiopurine therapy to maintain remission. The objective of this study was, therefore, to investigate these factors.
Methods
A total of 82 Crohn’s disease patients who received their first course of azathioprine or 6-mercaptopurine treatment at Severance Hospital between June 1996 and July 2007 were recruited to the study. During the follow-up period (25.5 ± 16.6 months) 19 patients (23.2%) discontinued the medication because of significant adverse effects. Forty-five patients who continued to receive thiopurines to maintain medically or surgically induced remission were enrolled in the study. After adjusting the maintenance dose, patients in remission were followed at 2–3 month intervals. Relapse was defined as a Crohn’s disease activity index ≥150.
Results
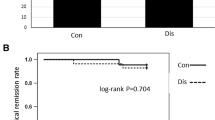
The male-to-female ratio was 1.5:1 and the mean age was 26.3 ± 7.1 years. Cumulative relapse was 18.0% after one year and 49.2% after three years. According to multivariate Cox regression analysis, younger age (<30 years) at thiopurine therapy and increased C-reactive protein level (≥0.5 mg/dL) at remission were independent predictors of relapse (hazard ratio 19.751, 95%-confidence interval (CI) 1.996–195.402, P = 0.011 and hazard ratio 9.001, 95% CI 1.583–51.181, P = 0.013, respectively).
Conclusions
Younger age (<30 years) and increased C-reactive protein level at remission were independent predictors of relapse in Crohn’s disease patients receiving thiopurines to maintain remission. These high-risk groups warrant closer observation and possibly early introduction of biological agents.




Similar content being viewed by others


References
Munkholm P, Langholz E, Davidsen M, et al. Disease activity courses in a regional cohort of Crohn’s disease patients. Scand J Gastroenterol. 1995;30:699–706.
Loftus EV Jr, Sandborn WJ. Epidemiology of inflammatory bowel disease. Gastroenterol Clin North Am. 2002;31:1–20.
Munkholm P, Langholz E, Nielsen OH, et al. Incidence and prevalence of Crohn’s disease in the county of Copenhagen, 1962–1987: a sixfold increase in incidence. Scand J Gastroenterol. 1992;27:609–614.
Yang SK, Yun S, Kim JH, et al. Epidemiology of inflammatory bowel disease in the Songpa-Kangdong district, Seoul, Korea, 1986–2005: a KASID study. Inflamm Bowel Dis. 2008;14:542–549.
Kim ES, Kim WH. Inflammatory bowel disease in Korea: epidemiological, genomic, clinical, and therapeutic characteristics. Gut Liver. 2010;4:1–14.
Cosnes J, Cattan S, Blain A, et al. Long-term evolution of disease behavior of Crohn’s disease. Inflamm Bowel Dis. 2002;8:244–250.
Pearson DC, May GR, Fick G, et al. Azathioprine for maintaining remission of Crohn’s disease. Cochrane Database Syst Rev. 2000;2:CD000067.
Peyrin-Biroulet L, Deltenre P, Ardizzone S, et al. Azathioprine and 6-mercaptopurine for the prevention of postoperative recurrence in Crohn’s disease: a meta-analysis. Am J Gastroenterol. 2009;104:2089–2096.
Candy S, Wright J, Gerber M, et al. A controlled double blind study of azathioprine in the management of Crohn’s disease. Gut. 1995;37:674–678.
Lennard-Jones JE. Classification of inflammatory bowel disease. Scand J Gastroenterol Suppl. 1989;170:2–6; discussion 16–19.
Sandborn WJ, Feagan BG, Hanauer SB, et al. A review of activity indices and efficacy endpoints for clinical trials of medical therapy in adults with Crohn’s disease. Gastroenterology. 2002;122:512–530.
Fraser AG, Orchard TR, Jewell DP. The efficacy of azathioprine for the treatment of inflammatory bowel disease: a 30 year review. Gut. 2002;50:485–489.
Kim PS, Zlatanic J, Korelitz BI, et al. Optimum duration of treatment with 6-mercaptopurine for Crohn’s disease. Am J Gastroenterol. 1999;94:3254–3257.
Murakami Y, Matsui T, Hirai F, et al. Efficacy of azathioprine in mild or moderate relapse in Crohn’s disease: clinical and endoscopic evaluation. Dig Endosc. 2010;22:25–32.
Thia KT, Loftus EV Jr, Sandborn WJ, et al. An update on the epidemiology of inflammatory bowel disease in Asia. Am J Gastroenterol. 2008;103:3167–3182.
Sahmoud T, Hoctin-Boes G, Modigliani R, et al. Identifying patients with a high risk of relapse in quiescent Crohn’s disease. The GETAID group. The groupe d’Etudes Therapeutiques des affections inflammatoires digestives. Gut. 1995;37:811–818.
Consigny Y, Modigliani R, Colombel JF, et al. A simple biological score for predicting low risk of short-term relapse in Crohn’s disease. Inflamm Bowel Dis. 2006;12:551–557.
Cosnes J, Carbonnel F, Beaugerie L, et al. Effects of cigarette smoking on the long-term course of Crohn’s disease. Gastroenterology. 1996;110:424–431.
Bouma G, Strober W. The immunological and genetic basis of inflammatory bowel disease. Nat Rev Immunol. 2003;3:521–533.
Macdonald TT, Monteleone G. Immunity, inflammation, and allergy in the gut. Science. 2005;307:1920–1925.
Ginaldi L, De Martinis M, D’Ostilio A, et al. The immune system in the elderly: II. Specific cellular immunity. Immunol Res. 1999;20:109–115.
D’Inca R, Bertomoro P, Mazzocco K, et al. Risk factors for non-adherence to medication in inflammatory bowel disease patients. Aliment Pharmacol Ther. 2008;27:166–172.
Horne R, Parham R, Driscoll R, et al. Patients’ attitudes to medicines and adherence to maintenance treatment in inflammatory bowel disease. Inflamm Bowel Dis. 2009;15:837–844.
Vermeire S, Van Assche G, Rutgeerts P. C-reactive protein as a marker for inflammatory bowel disease. Inflamm Bowel Dis. 2004;10:661–665.
Desai D, Faubion WA, Sandborn WJ. Review article: biological activity markers in inflammatory bowel disease. Aliment Pharmacol Ther. 2007;25:247–255.
Boirivant M, Leoni M, Tariciotti D, et al. The clinical significance of serum C reactive protein levels in Crohn’s disease. Results of a prospective longitudinal study. J Clin Gastroenterol. 1988;10:401–405.
Papi C, Festa V, Leandro G, et al. Long-term outcome of Crohn’s disease following corticosteroid-induced remission. Am J Gastroenterol. 2007;102:814–819.
Solem CA, Loftus EV Jr, Tremaine WJ, et al. Correlation of C-reactive protein with clinical, endoscopic, histologic, and radiographic activity in inflammatory bowel disease. Inflamm Bowel Dis. 2005;11:707–712.
Schnitzler F, Fidder H, Ferrante M, et al. Mucosal healing predicts long-term outcome of maintenance therapy with infliximab in Crohn’s disease. Inflamm Bowel Dis. 2009;15:1295–1301.
Baert F, Moortgat L, Van Assche G, et al. Mucosal healing predicts sustained clinical remission in patients with early-stage Crohn’s disease. Gastroenterology. 2010;138:463–468; quiz e410–e461.
Devlin SM, Panaccione R. Evolving inflammatory bowel disease treatment paradigms: top-down versus step-up. Gastroenterol Clin North Am. 2009;38:577–594.
Colombel JF, Sandborn WJ, Reinisch W, et al. Infliximab, azathioprine, or combination therapy for Crohn’s disease. N Engl J Med. 2010;362:1383–1395.
Lautenbach E, Berlin JA, Lichtenstein GR. Risk factors for early postoperative recurrence of Crohn’s disease. Gastroenterology. 1998;115:259–267.
Bitton A, Dobkin PL, Edwardes MD, et al. Predicting relapse in Crohn’s disease: a biopsychosocial model. Gut. 2008;57:1386–1392.
Prefontaine E, Macdonald JK, Sutherland LR. Azathioprine or 6-mercaptopurine for induction of remission in Crohn’s disease. Cochrane Database Syst Rev. 2010;6:CD000545.
Kim JH, Cheon JH, Hong SS, et al. Influences of thiopurine methyltransferase genotype and activity on thiopurine-induced leukopenia in Korean patients with inflammatory bowel disease: a retrospective cohort study. J Clin Gastroenterol. 2010;44:242–248.
Hindorf U, Lindqvist M, Peterson C, et al. Pharmacogenetics during standardised initiation of thiopurine treatment in inflammatory bowel disease. Gut. 2006;55:1423–1431.
Gisbert JP, Nino P, Rodrigo L, et al. Thiopurine methyltransferase (TPMT) activity and adverse effects of azathioprine in inflammatory bowel disease: long-term follow-up study of 394 patients. Am J Gastroenterol. 2006;101:2769–2776.
Zelinkova Z, Derijks LJ, Stokkers PC, et al. Inosine triphosphate pyrophosphatase and thiopurine s-methyltransferase genotypes relationship to azathioprine-induced myelosuppression. Clin Gastroenterol Hepatol. 2006;4:44–49.
Lowry PW, Franklin CL, Weaver AL, et al. Leucopenia resulting from a drug interaction between azathioprine or 6-mercaptopurine and mesalamine, sulphasalazine, or balsalazide. Gut. 2001;49:656–664.
Gilissen LP, Bierau J, Derijks LJ, et al. The pharmacokinetic effect of discontinuation of mesalazine on mercaptopurine metabolite levels in inflammatory bowel disease patients. Aliment Pharmacol Ther. 2005;22:605–611.
Hande S, Wilson-Rich N, Bousvaros A, et al. 5-aminosalicylate therapy is associated with higher 6-thioguanine levels in adults and children with inflammatory bowel disease in remission on 6-mercaptopurine or azathioprine. Inflamm Bowel Dis. 2006;12:251–257.
Shah JA, Edwards CM, Probert CS. Should azathioprine and 5-aminosalicylates be coprescribed in inflammatory bowel disease?: an audit of adverse events and outcome. Eur J Gastroenterol Hepatol. 2008;20:169–173.
Szumlanski CL, Weinshilboum RM. Sulphasalazine inhibition of thiopurine methyltransferase: possible mechanism for interaction with 6-mercaptopurine and azathioprine. Br J Clin Pharmacol. 1995;39:456–459.
Kim JH, Cheon JH, Kim WH. The frequency and the course of the adverse effects of azathioprine/6-mercaptopurine treatment in patients with inflammatory bowel disease. Korean J Gastroenterol. 2008;51:291–297.
Lee HJ, Yang SK, Kim KJ, et al. The safety and efficacy of azathioprine and 6-mercaptopurine in the treatment of Korean patients with Crohn’s disease. Intest Res. 2009;7:22–31.
Cheon JH, Kim JH, Kim BY, et al. Allele frequency of thiopurine methyltransferase and inosine triphosphate pyrophosphatase gene polymorphisms in Korean patients with inflammatory bowel diseases. Hepatogastroenterology. 2009;56:421–423.
Jung YS, Cheon JH, Park JJ, et al. Correlation of genotypes for thiopurine methyltransferase and inosine triphosphate pyrophosphatase with long-term clinical outcomes in Korean patients with inflammatory bowel diseases during treatment with thiopurine drugs. J Hum Genet. 2010;55:121–123.
Kim DU, Kim YH, Kim BJ, et al. The efficacy of low dose azathioprine/6-mercaptopurine in patients with inflammatory bowel disease. Hepatogastroenterology. 2009;56:1395–1402.
Hibi T, Naganuma M, Kitahora T, et al. Low-dose azathioprine is effective and safe for maintenance of remission in patients with ulcerative colitis. J Gastroenterol. 2003;38:740–746.
Andoh A, Tsujikawa T, Ban H, et al. Monitoring 6-thioguanine nucleotide concentrations in Japanese patients with inflammatory bowel disease. J Gastroenterol Hepatol. 2008;23:1373–1377.
Thia KT, Li M, Ling KL, et al. Azathioprine is effective in corticosteroid-dependent Asian inflammatory bowel disease patients. Inflamm Bowel Dis. 2011;17:809–815.
Korelitz BI, Present DH. Favorable effect of 6-mercaptopurine on fistulae of Crohn’s disease. Dig Dis Sci. 1985;30:58–64.
Ha C, Dassopoulos T. Thiopurine therapy in inflammatory bowel disease. Expert Rev Gastroenterol Hepatol. 2010;4:575–588.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Park, J.J., Cheon, J.H., Hong, S.P. et al. Outcome Predictors for Thiopurine Maintenance Therapy in Patients with Crohn’s Disease. Dig Dis Sci 57, 133–141 (2012). https://doi.org/10.1007/s10620-011-1955-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-011-1955-9