
Abstract
Background
Minimal hepatic encephalopathy (MHE) is associated with poor driving skills and insight. Increasing insight may improve receptiveness for therapy or driving restrictions.
Aim
To evaluate the change in the self-assessment of driving skills (SADS) using a driving simulator.
Methods
Cirrhotic patients and age/education-matched controls underwent MHE testing with inhibitory control (ICT) and the psychometric hepatic encephalopathy score (PHES). SADS, a Likert scale from 0 to 10, was administered just before and after a standardized driving simulation comprising testing and navigation tasks. The percentage SADS change from baseline was compared within/between groups.
Results
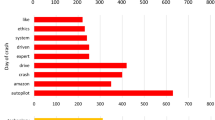
A total of 84 patients (60% men, age 55 years) and 12 controls were included. Controls were significantly better than cirrhotics on cognitive/simulator testing. The baseline SADS was similar between the groups. The baseline patient SADS was only correlated with ICT lures (r = −0.4, P = 0.001). Post-simulation, 60% of patients improved their insight, i.e., reduced SADS (from 8 to 6.5, P = 0.0001) compared to 25% of controls (P = 0.02). The mean percentage SADS reduction was also higher in cirrhotics (18% vs. 8%, P = 0.03). MHE on ICT patients had a significantly higher SADS improvement (P = 0.004) compared to the other patients; no difference was seen in those with/without MHE due to the PHES. The percentage SADS reduction in patients was correlated with getting lost (r = 0.468, P < 0.0001), crashes (P = 0.002), and centerline/road-edge excursions (P = 0.01). There was a significantly higher percentage SADS reduction in cirrhotics who got lost (25%) compared to those who did not get lost (12%) and controls (8%, P = 0.014).
Conclusions
Insight into driving skills in cirrhosis improves after driving simulation and is highest in those with navigation errors and MHE on ICT. Driving simulator-associated insight improvement may be the first step towards the cognitive rehabilitation of driving skills in cirrhosis.
Similar content being viewed by others


References
Bajaj JS, Wade JB, Sanyal AJ. Spectrum of neurocognitive impairment in cirrhosis: implications for the assessment of hepatic encephalopathy. Hepatology. 2009;50:2014–2021.
Bajaj JS, Saeian K, Schubert CM, et al. Minimal hepatic encephalopathy is associated with motor vehicle crashes: the reality beyond the driving test. Hepatology. 2009;50:1175–1183.
Kircheis G, Knoche A, Hilger N, et al. Hepatic encephalopathy and fitness to drive. Gastroenterology. 2009;137:1706–1715, e1–e9.
Bajaj JS, Stein AC, Dubinsky RM. What is driving the legal interest in hepatic encephalopathy? Clin Gastroenterol Hepatol. 2011;9:97–98.
Cohen SM, Kim A, Metropulos M, Ahn J. Legal ramifications for physicians of patients who drive with hepatic encephalopathy. Clin Gastroenterol Hepatol. 2011;9:156–160, quiz e17.
Bajaj JS, Saeian K, Hafeezullah M, Hoffmann RG, Hammeke TA. Patients with minimal hepatic encephalopathy have poor insight into their driving skills. Clin Gastroenterol Hepatol. 2008;6:1135–1139, quiz 1065.
Ferenci P, Lockwood A, Mullen K, Tarter R, Weissenborn K, Blei AT. Hepatic encephalopathy—definition, nomenclature, diagnosis, and quantification: final report of the working party at the 11th World Congresses of Gastroenterology, Vienna, 1998. Hepatology. 2002;35:716–721.
Kurz A, Pohl C, Ramsenthaler M, Sorg C. Cognitive rehabilitation in patients with mild cognitive impairment. Int J Geriatr Psychiatry. 2009;24:163–168.
Clare L, Linden DE, Woods RT, et al. Goal-oriented cognitive rehabilitation for people with early-stage Alzheimer disease: a single-blind randomized controlled trial of clinical efficacy. Am J Geriatr Psychiatry. 2010;18:928–939.
Weissenborn K, Ennen JC, Schomerus H, Rückert N, Hecker H. Neuropsychological characterization of hepatic encephalopathy. J Hepatol. 2001;34:768–773.
Bajaj JS, Hafeezullah M, Franco J, et al. Inhibitory control test for the diagnosis of minimal hepatic encephalopathy. Gastroenterology. 2008;135:1591–1600, e1.
Bajaj JS, Hafeezullah M, Hoffmann RG, et al. Navigation skill impairment: another dimension of the driving difficulties in minimal hepatic encephalopathy. Hepatology. 2008;47:596–604.
Marcotte TD, Wolfson T, Rosenthal TJ, et al. A multimodal assessment of driving performance in HIV infection. Neurology. 2004;63:1417–1422.
Bajaj JS, Hafeezullah M, Zadvornova Y, et al. The effect of fatigue on driving skills in patients with hepatic encephalopathy. Am J Gastroenterol. 2009;104:898–905.
Bajaj JS, Hafeezullah M, Hoffmann RG, Saeian K. Minimal hepatic encephalopathy: a vehicle for accidents and traffic violations. Am J Gastroenterol. 2007;102:1903–1909.
Weniger G, Ruhleder M, Lange C, Wolf S, Irle E. Egocentric and allocentric memory as assessed by virtual reality in individuals with amnestic mild cognitive impairment. Neuropsychologia. 2011;49:518–527.
Iachini I, Iavarone A, Senese VP, Ruotolo F, Ruggiero G. Visuospatial memory in healthy elderly, AD and MCI: a review. Curr Aging Sci. 2009;2:43–59.
Devos H, Akinwuntan AE, Nieuwboer A, Truijen S, Tant M, De Weerdt W. Screening for fitness to drive after stroke: a systematic review and meta-analysis. Neurology. 2011;76:747–756.
Cox DJ, Davis M, Singh H, et al. Driving rehabilitation for military personnel recovering from traumatic brain injury using virtual reality driving simulation: a feasibility study. Mil Med. 2010;175:411–416.
Classen S, Levy C, McCarthy D, Mann WC, Lanford D, Waid-Ebbs JK. Traumatic brain injury and driving assessment: an evidence-based literature review. Am J Occup Ther. 2009;63:580–591.
Wang PS, Lane M, Olfson M, Pincus HA, Wells KB, Kessler RC. Twelve-month use of mental health services in the United States: results from the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62:629–640.
Pia L, Neppi-Modona M, Ricci R, Berti A. The anatomy of anosognosia for hemiplegia: a meta-analysis. Cortex. 2004;40:367–377.
Antoine C, Antoine P, Guermonprez P, Frigard B. Awareness of deficits and anosognosia in Alzheimer’s disease. Encephale. 2004;30:570–577.
Stuss DT. Disturbance of self-awareness after frontal system damage. In: Prigatano GP, Schacter DL, eds. Awareness of deficit after brain injury: clinical and theoretical issues. New York, NY: Oxford University Press; 1991:63–83.
Zafiris O, Kircheis G, Rood HA, Boers F, Häussinger D, Zilles K. Neural mechanism underlying impaired visual judgement in the dysmetabolic brain: an fMRI study. Neuroimage. 2004;22:541–552.
Groeneweg M, Quero JC, De Bruijn I, et al. Subclinical hepatic encephalopathy impairs daily functioning. Hepatology. 1998;28:45–49.
Prasad S, Dhiman RK, Duseja A, Chawla YK, Sharma A, Agarwal R. Lactulose improves cognitive functions and health-related quality of life in patients with cirrhosis who have minimal hepatic encephalopathy. Hepatology. 2007;45:549–559.
Bajaj JS, Heuman DM, Wade JB, et al. Rifaximin improves driving simulator performance in a randomized trial of patients with minimal hepatic encephalopathy. Gastroenterology. 2011;140:478–487, e1.
Sidhu SS, Goyal O, Mishra BP, Sood A, Chhina RS, Soni RK. Rifaximin improves psychometric performance and health-related quality of life in patients with minimal hepatic encephalopathy (the RIME Trial). Am J Gastroenterol. 2011;106:307–316.
Acknowledgments
This study was partly supported by the American College of Gastroenterology (ACG) Junior Faculty Development Award, R01DK087913 from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), National Institutes of Health (NIH), and award UL1RR031990 from the National Center for Research Resources (NCRR), NIH.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bajaj, J.S., Thacker, L.R., Heuman, D.M. et al. Driving Simulation Can Improve Insight into Impaired Driving Skills in Cirrhosis. Dig Dis Sci 57, 554–560 (2012). https://doi.org/10.1007/s10620-011-1888-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-011-1888-3