
Abstract
Multivalvular heart disease (MVD) is an aggregate of regurgitant and/or stenotic lesions of at least two cardiac valves. Ventricular tissue deformation imaging is a powerful predictor of subclinical myocardial dysfunction in patients with MVD.The aim of this study was to examine the left and right ventricular strain patterns in MVD as well as observe any association between right–sided valvular involvement (tricuspid or pulmonary valve lesion) with that of aortic and/or mitral valve lesion. Patients with at least moderate forms of MVD were included in the present study. 72 patients with mean age of 56.69 ± 14.59 years and various presentations of MVD were finally enrolled in this study. The commonest cause for MVD was rheumatic heart disease in these patients. Conventional 2-dimensional parameters as well as tissue deformation imaging parameters were assessed in offline mode for these patients. The Mean ± SD values for various quantitative 2D echocardiographic conventional and tissue deformation imaging were assessed. It was observed that LV strain parameters including the global longitudinal strain (GLS) were preserved whereas the RV strain parameters were mildly reduced (RV GLS total is − 19.49 ± 6.08%). Also, when conventional echocardiographic parameters were assessed to see any association between aortic and/or mitral valve disease with that of right-sided valvular lesions (tricuspid or pulmonary); 2D conventional echocardiographic parameters like left atrial dimension (p = 0.034), TAPSE (tricuspid annular plane systolic excursion) (p < 0.001), RVSP (right ventricular systolic pressure) (p < 0.001) and IVC (inferior vena cava) dimensions (p < 0.001) showed a statistically significant result; whereas, when strain parameters for LV and RV were assessed, they did not show any statistical difference for the same. In this series of patients with significant MVD, our findings suggest that ventricular strain parameters may be reliable markers of myocardial dysfunction, but may alter depending on the underlying combination of MVD, and right ventricular strain should also be an important parameter while assessing different combinations of MVD.
Similar content being viewed by others


Introduction
Multivalvular heart disease (MVD) is defined as aggregate of regurgitant and/or stenotic lesions of at least two cardiac valves [1]. Valves affected in multivalvular heart disease are aortic, mitral, tricuspid and/or pulmonary. The most common associations of multiple valve lesions were aortic stenosis (AS) and mitral regurgitation (MR) and also aortic regurgitation (AR) plus mitral regurgitation (MR).
Global prevalence for MVD was reported to be 63.9 per 1, 00,000 person-years [2]. According to Euro Heart Survey, for patients presenting with MVD, the in- hospital mortality rates were 6.5% [3]. Rheumatic heart disease (RHD) is the major cause for primary or organic MVD. According to Euro Heart Survey, rheumatic fever was the most common pathogenesis accounting for about 51% of MVD cases, also other causes included degenerative valve diseases accounting for almost 41% [3]. In India, almost 44,000 patients are added every year, and expected mortality is 1.5%–3.3% per year due to RHD causing MVD [4].
Strain echocardiography/tissue deformation imaging, is one of the best imaging echocardiographic modality in diagnosis and prognostic evaluation of valvular lesions. Indication for use of strain imaging in MVD is to detect subclinical myocardial dysfunction before an overt reduction of LV ejection fraction and thus can be used to determine the exact intervention time before the ventricular function further deteriorates and also determines prognosis of MVD [5].
Most of the patients visiting our cardiology OPD present with either single (more common) or with concomitant multiple valvular lesions. Limited studies focused on ventricular loading response to multivalvular heart disease in literature. Tissue deformation imaging in identifying subclinical myocardial dysfunction among these population have not been studied thoroughly.
This study is one of its kind to emphasize ventricular strain mechanics in multiple valvular disease loading conditions. The purpose of this study was to assess left and right ventricular strain patterns in multivalvular heart disease and also to assess involvement of right sided valvular lesions with aortic and/or mitral valvular lesions.
Materials and methods
Study protocol and patient selection
A total of 72 patients with MVD involving more than or equal to two valves with a severity of at least more than moderate valvular lesion examined in echocardiography laboratory at the Department of Cardiology, KMC, Manipal enrolled from March 2020 to May 2021 were considered eligible for the study. Exclusion criteria included any associated ischemic heart disease, LV ejection fraction < 50%, previous history or intracardiac/prosthetic heart surgery and restrictive cardiomyopathy(RCM).The study protocol was intended to have sample size of 100 as we wished to take samples based on time bound pattern;i.e., 5 to 10 patients per month. The study was approved by the Board of Ethics Committee, Kasturba Hospital, Manipal (contact no.0820–292371) and also the subjects gave the informed consent.
Clinical data
Clinical data included age, gender, height, weight, body mass index, history of hypertension and diabetes, smoking or drinking status, food habits and history of coronary artery disease of the subjects. Also, surface electrocardiographic (ECG) recordings of the subjects were taken and reported.
Echocardiography
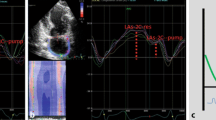
At entry in the study, all patients underwent a comprehensive echocardiography using commercially available equipment (VIVID S60 echocardiographic system, GE Healthcare) at rest. Standard views were obtained with patient positioned in left lateral decubitus position. Standard views (i.e. parasternal long axis and short axis at three levels of LV and apical 4, 5, 3 and 2 chamber) views were recorded and stored LVEF measurements are taken by M mode and Simpson’s method. Left ventricular (LV) end diastolic dimensions (IVS thickness, LV posterior wall thickness and LV internal dimension) were acquired from the parasternal long axis view at the mitral valve leaflet tips. TAPSE values obtained from M mode at tricuspid valve annulus. 2 dimensional tissue deformation imaging of LV and RV strain parameters were measured offline in an echocardiography core laboratory using dedicated commercial software system (Echo-Pac) (Fig. 1). Three consecutive cardiac cycles were acquired in apical 4ch, 2ch, 3ch and short axis at 3 levels (base, mid, apex) for LV and for RV strain was measured at 3 levels of free wall (base, mid ,apex) respectively. Analysis was done by tracing the endocardial border and the region of interest is split in six segments automatically by the software. After the region of interest is selected the software spontaneously displays the strain and strain rate curve patterns of different segments along with Bull’s eye of 17 segments. Strain rates at peak systole, early diastole and late diastole were obtained.
Data analysis
All data were entered in excel sheet. Statistical analysis was carried out using the EZR (32 bit) version 1.37. Continuous variables was expressed as Mean ± SD and compared using one way analysis of variance. Categorical data was expressed as frequency, percentage and analyzed using Chi Square test. Results were considered significant with p value less than 0.05.

Transthoracic echocardiographic and 2D strain analysis in one of the present study’s patient with MVD (Moderate mitral stenosis and regurgitation + severe aortic regurgitation + moderate tricuspid regurgitation; (A). Tissue deformation imaging showing LV global longitudinal strain of (− 17.3%) and (B). Tissue deformation imaging showing RV strain of − 20.2%
Results
Patient characteristics
All patients who met the inclusion criteria and met no exclusion criteria were included for analysis on the basis of their diagnosis. This study included 72 patients with MVD with mean age of 56.69 ± 14.59 years, among them 34(42.7%) were males and 38(52.8%) were females, and other baseline demographic and clinical characteristics are mentioned in (Table 1).
Multivalvular disease types of presentation and 2D conventional and tissue deformation imaging parameters of the study population
Out of these 72 patients included in the present study, majority of patients presented with left-sided valvular lesions (aortic and/or mitral) along with concomitant right- sided valvular lesions (tricuspid/pulmonary); remaining patients had AR and MR, AR and MS, AS and MR, AS and MS respectively (Fig. 2). The conventional 2D echocardiographic parameters were assessed for LV and RV, the results were within the normal range for both.LV and RV tissue deformation imaging parameters were also assessed like global strain, peak systolic strain, systolic strain rate, early and late diastolic strain rates respectively. The LV strain parameters were well preserved; whereas RV global strain was mildly reduced (Table 2).

Different patterns of MVD
Association of right -sided valvular lesions (tricuspid or pulmonary disease) with 2D conventional and speckle- tracking strain echocardiographic parameters
Among 72 patients with MVD who were included in our study as per the inclusion criteria, a majority 38 patients had right -sided valvular lesions along with mitral and/or aortic valvular disease. As mentioned in (Table 3), various echocardiographic parameters were assessed to observe association with right–sided valvular lesions. It was observed that left atrial dimensions (p = 0.034) was statistically significant; TAPSE (p < 0.001), RVSP (p < 0.001) as well as IVC maximum and minimum dimensions (p < 0.001) show a highly significant statistical difference; whereas all other echocardiographic parameters are statistically non- significant.
Also, when tissue deformation imaging parameters for LV and RV were assessed to see any association with right-sided valvular lesions (tricuspid or pulmonary valve disease), none of them showed a statistically significant result.
Discussion
In the present study, 72 individuals (which included 34 males and 38 females) were enrolled after confirming that they had at least moderate forms of multivalvular disease involving any 2 or more cardiac valves. Out of these 72 subjects, 11 of them had already undergone percutaneous balloon mitral valvulotomy (BMV) for mitral stenosis but still had persisting mild to moderate degrees of mitral stenosis.The demographic and clinical features of the patients are given in Table 1.
Rheumatic heart disease (RHD) defined as a manifestation of rheumatic fever, an autoimmune disorders affecting multiple organ systems, is a disease associated with poor hygiene, overcrowding, poverty and low socioeconomic status [6,7,8,9]. In India alone, there has been drastic variations in prevalence of RHD in different demographic regions. In the present study majority of subjects enrolled where illiterate, unemployed and from rural dwelling.
In 1943, Don Carlos et al. [21] reported that “Diet is a predisposing factor for rheumatic fever” collecting data from many countries including India. Rinehart et al. [22], 1934 reported that there is a belief that deficiencies in vitamin D, calcium and phosphorus(less intake of milk, eggs and fish) can predispose to development of rheumatic manifestations during infancy. He believed that the autoantibodies generated in rheumatic fever are a part of macrophage system in the body that are all formed from the mesodermal layer that also gives rise to bones and connective tissue; hence, deficiency of vitamin D, calcium and phosphorus can all make one’s body defense system weak.
However, in the present study, majority of individuals with MVD were non vegetarians, 49(68.1%) rather than vegetarians, 23(31.9%) (Table 1). Hence, concluding that diet alone is not a factor for development of RHD, further research is required in this field.
Rheumatic heart disease and multivalvular heart disease
In this study, a population of significant multivalvular disease was enrolled, predominantly with rheumatic etiology(83.8%) and least were degenerative valvular disease(13.5%) (Table 1); unlike other studies carried out by Cramariuc et al., 2010 [23] and Song Y et al., 2013 [24], which included predominantly degenerative valvular diseases. Out of the 72 patients, majority of 38(52.8%) patients presented with left-sided valvular lesions (aortic and/or mitral) along with concomitant right- sided valvular lesions (tricuspid/pulmonary); remaining21 (29.2%) patients had aortic regurgitation and mitral regurgitation, 21(29.2%) patients had aortic regurgitation and mitral stenosis, 3(4.2%) patients had aortic stenosis and mitral regurgitation, 2(2.8%) had aortic stenosis and mitral stenosis respectively (Fig. 2).
In the Indian subcontinent, as discussed earlier RHD is the commonest cause of MVD accounting for about 2–4 million cases, as reported by Kumar et al., 2013 [25].As MVD remains to be the main setting in RHD, evaluation and management are challenging. There are multiple combinations possible in MVD and hence this variability leads to availability of limited data for management strategies. Although as each case of MVD differs from the other, we need to consider the underlying etiology, pathophysiological presentations, assess clinical features and echocardiographic parameters to provide the best treatment strategy [1, 10,11,12].
Left and right ventricular strain patterns in MVD
In the present study, we have used both conventional echocardiographic parameters along with tissue deformation imaging parameters to determine different LV and RV strain patterns in MVD.Echocardiography being the main diagnostic tool for MVD, there are few pitfalls in considering 2D echocardiographic parameters alone, also it becomes cumbersome when measurements of more than one cardiac valvular involvement has to be ruled out [1, 10].There are many studies that have been conducted to evaluate myocardial function in valvular heart disease using the advanced 2D strain echocardiography, but there is very limited data focusing its application in MVD.
A recent study conducted by Andrew W et al., 2021 [26] considered necessity of strain echocardiography in subjects with mixed aortic valve disease (AS with AR), it was concluded that LV global strain had prognostic associations with clinical outcomes when left ventricular ejection fraction was normal; however, the author also focused on the fact that LV-GLS needs to consider which valvular lesion is the cause for LV remodeling when interpreting GLS,due to more complex relationship among mixed aortic valve disease as opposed to isolated AS or AR.
A study conducted by In-Jeong Cho et al., 2020 [27] was based on “Determinants of clinical outcomes in patients with mixed mitral valve disease”. They only assessed routine echocardiographic parameters to determine the clinical outcomes, strain echocardiographic parameters of LV were not assessed. They concluded that transmitral pressure gradient should be considered as an important echocardiographic parameter to predict the clinical outcomes.
Alex Felix et al., 2018 [15] conducted a study to evaluate right ventricular function in subjects with left-sided valve lesions, but patients with severe TR were excluded from the study as it could interfere during RV strain measurements. They concluded that RV function was depressed in these patients, and hence RV function assessment should also be considered in patients with left-sided valvular lesions. None, of the above mentioned studies used strain echocardiography for different presentations of MVD.
In the present study, we included patients with TR as well, because most of our patients with MVD had significant right-sided valvular disease with either aortic and/or mitral disease (38 patients out of 72) (Fig. 2). Also, it was observed that LV ejection fraction (63.83 ± 4.84.
%), other LV echocardiographic parameters and even strain parameters (LV-GLS: 17.49 ± 41.17%) were normal (Table 3). This may be due to various presentations of LV loading conditions, wall stress and LV remodeling condition based on the underlying presentation of MVD. However, unlike LV echocardiographic parameters, the RV strain parameters like RV free wall strain(basal,mid,apical) (− 19.49 ± 6.08%) showed reduced values (Table 3). This may be due to higher levels of pulmonary pressures and RV pressure overload secondary to left-sided valvular disease [13, 14].
Involvement of right -sided valvular lesions with aortic or mitral valvular lesions
In the present study, out of 72 patients with MVD, 38 of them had right—sided valvular disease (moderate to severe tricuspid valve disease) with mitral and/or aortic valve disease. When RV echocardiographic parameters were compared 2D derived left atrial dimensions (p = 0.034) was significant; TAPSE (p < 0.001), RVSP (p < 0.001) and IVC dimensions (p < 0.001) showed highly statistically significant result (Table 2), whereas none of the tissue deformation imaging derived ventricular (LV and RV) strain parameters were statistically significant.
Mittal et al., 2001 [17] performed a study on “Echocardiographic assessment of RV function in patients with pure mitral stenosis”, they did not find any correlation between right ventricular systolic function and MS.
Another study by Galli et al., 2013 [16] studied 200 patients with degenerative AS, these patients showed RV dysfunction by echocardiography.
Later, in literature many studies were done to assess RV function by echocardiography in left –sided valvular lesions, whereas none included MVD.They concluded that the impairment of RV function in left-sided valvular disease is either due to increased pulmonary capillary pressures, RV overload, ventricular interdependence (due to septal flattening because of RV enlargement) and due to some inflammatory changes due to rheumatic disease in RHD cases [15,16,17,18,19,20].
Limitation of the study
Unequal gender distribution and multivalvular disease type is the major limitation in our study due to constricted time limit. Smaller sample size due to ongoing COVID pandemic, this may have limited our ability to detect significant associations with other factors in MVD subjects.
Clinical implications
Despite of having any presentation of MVD, the prognosis and course of treatment should be based on approach to individual valvular lesions, as the use of strain echocardiographic parameters alone is not sufficient.
Conclusion
We have provided new insights about alterations in ventricular strain patterns for different combinations of MVD. Subclinical myocardial dysfunction assessment using strain echocardiography is again dependent on various loading conditions on the ventricles and severity of the lesions. Also, it is extremely important that RV strain analysis should even be employed for MVDs affecting the left-sided heart valves alone.
Data availability
Master sheet with individual patient data will be submitted if requested.
Abbreviations
- MVD:
-
Multivalvular disease
- LV:
-
Left ventricle
- RV:
-
Right ventricle
- GLS:
-
Global longitudinal strain
- TAPSE:
-
Tricuspid annular plane systolic excursion
- RVSP:
-
Right ventricular systolic pressure
- IVC:
-
Inferior vena cava
- RHD:
-
Rheumatic heart disease
- AS:
-
Aortic stenosis
- AR:
-
Aortic regurgitation
- MS:
-
Mitral stenosis
- MR:
-
Mitral regurgitation
- RCM:
-
Restrictive cardiomyopathy
- IVS:
-
Interventricular septum
- EZR:
-
Easy R statistical software
References
Unger P, Rosenhek R, Dedobbeleer C et al (2011) Management of multiple valve disease. Heart 97:272–277
Andell P, Li X, Martinsson A et al (2017) Epidemiology of valvular heart disease in a Swedish nationwide hospital-based register study. 103:1696–1703
Lung B et al (2003) a prospective survey of patients with valvular heart disease in europe: the euro heart survey on valvular heart disease. Eur Heart J 24:1231–1243
Negi PC, Sondhi S, Asotra S et al (2019) Current status of rheumatic heart disease in India. Indian Heart J 71(1):85–90
Jae-Hyeong P et al (2019) Two dimensional echocardiographic assessment of myocardial strain: important echocardiographic parameter readily useful in clinical field. Korean Circ J 49(10):908–931
Watkins DA, Johnson CO, Colquhoun SM et al (2017) Global, regional, and national burden of rheumatic heart disease, 1990–2015. N Engl J Med 377:713–722
de Jessica LD, de Nick K, Jonathan RC et al (2018) How many doses make a difference? An analysis of secondary prevention of rheumatic fever and rheumatic heart disease. J Am Heart Assoc 7(24):e010223
Muhamed B, Parks T, Sliwa K (2020) Genetics of rheumatic fever and rheumatic heart disease. Nat Rev Cardiol 17(3):145–154
Sika-Paotonu D, Beaton A, Raghu A, Steer A, Carapetis J (2016) Acute rheumatic fever and rheumatic heart disease. Streptococcus pyogenes: Basic Biology to Clinical Manifestations. Oklahoma City (OK): University of Oklahoma Health Sciences Center
Suruchi L, Kapoor PM (2017) Challenges in multivalvular heart disease: Indian scenario. J Cardiac Crit Care TSS 01(01):015–020
Vahanian A, Baumgartner H, Bax J et al (2007) Guidelines on the management of valvular heart disease: the task force on the management of valvular heart disease of the European society of cardiology. Eur Heart J 28(2):230–268
Manjunath CN, Srinivas P, Ravindranath KS et al (2014) Incidence and patterns of valvular heart disease in a tertiary care high-volume cardiac center: a single center experience. Indian Heart J 66(3):320–326
Pirat B, McCulloch ML, Zoghbi WA (2006) Evaluation of global and regional right ventricular systolic function in patients with pulmonary hypertension using a novel speckle tracking method. Am J Cardiol 98(5):699–704
Ikeda S, Tsuneto A, Kojima S et al (2014) Longitudinal strain of right ventricular free wall by 2-dimensional speckle-tracking echocardiography is useful for detecting pulmonary hypertension. LifeSci 111(1–2):12–17
dos Felix AS, dos Siciliano APRV, Belém LHJ et al (2018) Echocardiographic assessment of right ventricular function by two dimensional strain in patients with left-sided valvular heart disease: comparison with three-dimensional echocardiography. Int J Cardiovasc Sci 31(6):630–642
Galli E, Guirette Y, Feneon D et al (2015) Prevalence and prognostic value of right ventricular dysfunction in severe aortic stenosis. Eur Heart J Cardiovasc Imaging 16(5):531–538
Mittal SR, Goozar RS (2001) Echocardiographic evaluation of right ventricular systolic functions in pure mitral stenosis. Int J Cardiovasc Imaging 17:13–18
Castro ML, Barbosa MM, Barbosa JA et al (2013) Value of right ventricular strain in predicting functional capacity in patients with mitral stenosis. Int J Cardiol 168(3):2927–2930. https://doi.org/10.1016/j.ijcard.2013.03.181
Tanboga IH, Kurt M, Bilen E et al (2012) Assessment of right ventricular mechanics in patients with mitral stenosis by two-dimensional deformation imaging. Echocardiography 29(8):956–961
Ozdemir AO, Kaya CT, Zdol CO et al (2010) Two-dimensional longitudinal strain and strain rate imaging for assessing the right ventricular function in patients with mitral stenosis. Echocardiography 27(5):525–533
Don Carlos Peete (1944) Rheumatic fever: diet as a predisposing factor. Annals of internal medicine. https://doi.org/10.7326/0003-4819-21-1-44.
Rinehart JF, Greenberg LD, Olney M et al (1938) Metabolism of vitamin C in rheumatic fever. Arch Intern Med (Chic) 61(4):552–561
Cramariuc D, Gerdts E, Davidsen ES et al (2009) Myocardialdeformation in aortic valvestenosis: relation to left ventricular geometry. Heart (British Cardiac Society). 96(2):106–112
Song Y, Lee S, Kwak Y-L et al (2013) Tissue doppler imaging predicts left ventricular reverse remodeling after surgery for mitral regurgitation. Ann Thorac Surg 96(6):2109–2115
Krishna Kumar R, Tandon R (2013) Rheumatic fever & rheumatic heart disease: the last 50 years. Indian J Med Res 137(4):643–658
Harris AW, Pibarot P, Otto CM (2020) Aortic stenosis: guidelines and evidence gaps. Cardiol Clin 38(1):55–63. https://doi.org/10.1016/j.ccl.2019.09.003
Cho IJ, Lee SE, Jeong H, Chang HJ (2020) Determinants of clinical outcomes in patients with mixed mitral valve disease. Echocardiography 37(8):1164–1170. Epub 2020 Jul 12. https://doi.org/10.1111/echo.14673
Funding
Open access funding provided by Manipal Academy of Higher Education, Manipal. None
Author information
Authors and Affiliations
Contributions
K. Prathiksha. Prabhu collected the data, analysis and excel sheet entry, Dr. Krishnananda Nayak, Dr. Ashwal A J and Dr. M Sudhakar Rao supervised the entire study, Vidya Nayak and Sridevi Prabhu prepared the manuscript, Rekha V did the statistical analysis. All authors have read and approved the manuscript. There is no association with any industry and this is not funded by any. No honorarium, grant, or other forms of payment was given to anyone to produce the manuscript. Each author listed on the manuscript has seen and approved the submission of this version of the manuscript and takes full responsibility for the manuscript. I will also transfer the rights of the article to the journal upon publication.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Conflict of interest
The authors report no financial relationships or conflicts of interest regarding the content herein. The paper is not under consideration elsewhere. None of the paper’s contents have been previously published.
Ethical approval
Institutional ethical committee clearance was obtained.
Informed consent
As it was a prospective study, consent by the participants was obtained .All the participants had given written consent to undergo echocardiographic study.
Consent to participate
Participants gave informed written consent.
Consent for publication
Participants gave their written informed consent for publication of data.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Prathiksha Prabhu, K., Nayak, K., Nayak, V. et al. Ventricular strain patterns in multivalvular heart disease: a cross-sectional study. Int J Cardiovasc Imaging 39, 331–338 (2023). https://doi.org/10.1007/s10554-022-02737-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10554-022-02737-2