
Abstract
Introduction
Skin melanoma incidence has risen in the last decades becoming a major public health problem in many regions of the world. Geographic variation of rates is not well understood.
Purpose
To assess the spatial distribution of skin melanoma in Gran Canaria Island (Canary Islands, Spain) and to evaluate the role of environmental, socio-economic, and demographic factors in this distribution.
Methods
We performed a small-area study with disease mapping at the census-tract level (CT) in Gran Canaria between 2007 and 2018. After testing for spatial autocorrelation, we integrated individual-level health data with census-based demographic and socio-economic indicators, and satellite-based environmental data. Finally, we assessed the role of demographic, socio-economic and environmental factors on skin melanoma incidence using a Bayesian analytical framework, with options for non-spatial and spatial random effects.
Results
1058 patients were diagnosed with invasive skin melanoma in the study period and geolocated to a CT (number of CT in Gran Canaria = 565). We found evidence of global spatial autocorrelation in skin melanoma incidence (Moran’s I = 0.09, pseudo p-value = 0.001). A few hotspots were detected, fundamentally in urban northern tracts. A radial pattern of high values was also observed in selected ravines with historical isolation. Multivariable conditional autoregressive models identified urbanicity, percent of females, and a high socio-economic status as risk factors for disease. Solar radiation did not show a significant role.
Conclusion
Urbanicity and a high socio-economic status were identified as the main risk factors for skin melanoma. These associations might reflect differential melanoma susceptibilities or be explained by health inequalities in detection. This study also uncovered high-risk areas in particular ravines. Future targeted research in these regions might help better understand the role of genetic and toxic factors in melanoma pathogenesis.
Similar content being viewed by others


Introduction
Geographic variability in skin melanoma incidence is a long-standing observation, with the highest rates occurring in Australasia, North-western Europe, and Northern America [1]. Environmental, phenotypic, and socio-economic factors are thought to explain this variation [2, 3] that is still poorly understood.
Excessive ultraviolet radiation (UV) exposure among fair-skinned populations has been identified as the main environmental risk factor to develop disease [4] and high socio-economic status (SES) populations have consistently been associated with increased incidence rates [3], which has given rise to the concepts of a latitudinal and a social gradient in melanoma distribution [5,6,7]. However, many regions escape these gradients and, despite the potential confounding role that environmental and socio-demographic factors could have for one another, the influence of both types of risk factors has deserved little attention [8, 9].
The evolution of spatial epidemiology in the last two decades as Geographic Information Systems (GIS) have become more available, together with the advent of methodological and computational developments, has enabled the assessment of geographic variations of disease with a new scope [10]. By allowing to integrate and link data from multiple sources at a small-area level, spatial methods have become an asset in cancer surveillance and as a hypothesis generating tool [11].
The Canary Islands are a Spanish archipelago located in the Atlantic Ocean off the coast of North-western Africa, with a subtropical climate. The population in the islands is exposed to a high environmental risk for the development of skin cancers [12], yet unexpectedly the incidence of skin melanoma in the region is among the lowest in Spain and below the estimates provided by the World Health Organization for Southern Europe [1, 13].
Mapping skin melanoma distribution in Gran Canaria, one of the main Islands, and evaluating the factors driving this geographic distribution could provide insight into this unexpected epidemiological finding and contribute to disentangle the role of environmental and socio-economic factors in melanoma incidence at a small geographic scale.
In this study, we assessed the spatial heterogeneity of skin melanoma incidence at the census-tract (CT) level across Gran Canaria in the period 2007–2018. In addition, we aimed at identifying the occurrence of potential hotspots, namely areas at higher risk of skin melanoma across the island, and at evaluating whether demographic, socio-economic, and environmental variables could represent risk factors for skin melanoma occurrence and explain its spatial variation.
Methods
Study site and study population
Gran Canaria is one of the two main islands of the Canary Islands archipelago. With a population of about 850,000 inhabitants, its area is relatively small (1,560 km2), yet the altitude range is high (0–1,956 m), reflecting its volcanic origin. With an almost circular shape of diameter 47 km, it can be topographically divided into ravines that start in the central summit down to the coast, in a radial configuration (Supplementary Fig. S1) [14]. The capital city of Las Palmas de Gran Canaria (LPGC) is located in the northeast corner of the island and concentrates about half of the island’s population.
Universal health coverage is available in the region and delivered through the government-funded Canary Islands Healthcare Service (CIHS). Access to dermatologic care in the CIHS is available through a General Practitioner (GP) referral, and GPs are assigned based on residential address.
Data sources
Skin melanoma cases were obtained from the Gran Canaria skin melanoma dataset specified below, and covariate data were downloaded from the open-data sources listed in supplementary Table S1. A detailed description of the datasets is also provided.
Skin melanoma cases
The Gran Canaria skin melanoma dataset used in this study has been previously described in detail [13]. It includes demographic, clinical, and histological information of all invasive skin melanoma cases evaluated at the CIHS among GC residents, diagnosed between January 2007 and December 2018. It has a comprehensive geographic coverage within the island and contains all cases diagnosed in the public CIHS facilities (which represent 86% of all healthcare in the region) [15] and most cases diagnosed in the private setting. It was compiled following the International Classification of Diseases ICD-10 diagnosis code C43 (malignant melanoma of skin), thereby excluding in situ and mucosal melanomas. In case multiple melanomas were diagnosed in a patient, only the first one was counted, in accordance with the International Agency for Research on Cancer rules [16].
The information about the residential address of patients at the time of diagnosis was retrieved from the clinical records before the dataset was de-identified for further analyses. Cases were located at the street level and then reassigned to a CT by georeferencing the street.
Spatial unit
CTs are the smallest geographic unit for which census data are available in Spain. Population data for Gran Canaria and the outline of CTs were downloaded from the Spanish National Institute of Statistics (INE) and corresponded to the Spanish Population and Housing Censuses of 2011 (SPHC2011)[17].
In Spain, the census is updated every ten years. SPHC2011 was the first census based on a sampling survey and included 12.3% of the population. Surface areas of CTs in Gran Canaria varied from 8,798 to 12,306,130 m2, the population size range was 320 to 5,565 inhabitants and the number of CTs 565.
Demographic and socio-economic variables
Demographic (age and sex composition of the population) and educational attainment indicators were obtained from the SPHC2011 database.
Some additional economic indicators, such as unemployment rates, income type, and rent, were obtained from Spain’s Household income distribution atlas for 2015 at the same geographic scale (CT level) [18].
In addition, we also considered the first deprivation index with full geographic coverage in Spain (IP2011) that has recently been made publicly available [19]. Based on socio-economic indicators from the SPHC2011 and elaborated using principal component analysis, IP2011 integrates information regarding percentages of the following indicators: manual workers, temporary workers, unemployment, insufficient (incomplete compulsory) education overall, insufficient education among youth (16 to 29-year-olds), and dwellings without internet access [19]. Constructed as a quantitative variable at the CT level, it is a standardized index with a mean of 0 and standard deviation of 1 and is to be interpreted on relative terms, with values close to 0 indicating the average deprivation of the country, positive values indicating more deprivation (meaning more poverty) and negative values less deprivation.
Environmental variables
Cartographic data included administrative boundaries, roads, water surfaces, and altitude data. Land cover information was obtained from the European Environmental Agency’s satellite data of the Copernicus Land Monitoring Service [20]. Solar radiation data were downloaded from the global climate and weather data WorldClim (version 2.0) [21].
Data preparation
Georeferencing skin melanoma cases
We georeferenced the residential addresses of cases at the street level with two widely used Application Programming interfaces (APIs): OpenCage geocoder and Google Earth Engine, extracting longitude and latitude for each occurrence with both APIs. For this, we used the packages opencage v0.2.2 and ggmap v3.0.0 in R v3.6.3 [22,23,24]. We mapped coordinates to cross-check for spatial consistency. Discordant cases and those with potential geolocation errors were manually geolocated with OpenStreetMap. As a second step, we aggregated the spatial point data to the CT level. Gran Canaria is divided into 565 CTs, yet when linking the shapefile to the census, three tracts did not exist and were merged to the corresponding ones with a final number of 562 tracts. A shapefile was created with these aggregated data.
Spatial covariates: potential predictors of the distribution of cases
The proportion of females per CT was obtained by dividing the total number of females by the total population, within each CT.
Regarding SES variables available at the census, we generated a new variable named p_basic (basic studies) by aggregating the variables: (i) illiterate persons, (ii) those without studies (less than 5 years of schooling), and (iii) those with first-level studies (elementary school completed, as higher educational attainment). For each CT, all variables of educational attainment were divided by the population aged over 16 years, to obtain a proportion of the population with different degrees of educational attainment within each CT (p_basic, p_2_grd, and p_3_grd, supplementary Tables S1, S2). Economic indicators of 2015 were aggregated to their corresponding CT.
The deprivation index covariate had the same geographic coverage as the other SES variables and was linked to the census shapefile without incidences.
Land cover and climatic data were downloaded at a global scale in a raster format (continuous surface divided into regular grids) and extracted for the Canary Islands with the Mask feature of ArcGIS and projected in ETRS89/UTM zone 30 N (EPSG: 25830) at 1km2 resolution. Land cover data originally had 44 different categories and were obtained at 100-m resolution. It was expected that data scarcity for many categories would be troublesome, therefore a simplified Corine classification with broader categories was used, those being: artificial surfaces (urban), agricultural areas, and forests and semi-natural areas. In case a CT contained many categories, it was assigned the modal value (most frequent category). In order to allow for modeling with binary or numeric variables, a further simplified categorization of these three categories was performed, finally using percent of urban land and percent of non-urban land (agricultural, forests and semi-natural areas).
Hillshade and slope rasters were created using the corresponding ArcGIS Spatial Analysis tools, by integrating the information about altitude and azimuth from cartographic data.
For rasters with numeric values (Hillshade, solar radiation, digital elevation, and slope), the mean value for each cell was extracted. Input grids were resampled to a common spatial resolution of 1 km2 using the nearest neighbor approach and clipped to match the geographic extent of a map of Gran Canaria and eventually aligned to it. Raster manipulation and processing were undertaken using raster [26] package in R and final map layouts created with ArcGIS 10.8 software [25].
Missing data for covariates were scarce (the maximum missing data of a covariate occurred in 16 CTs). For missing values, multiple imputation was performed with mice [27] R package, by means of a linear regression using bootstrapping.
Statistical analyses
Outcome definition
The outcome of this study was the spatial distribution of skin melanoma incidence in Gran Canaria in 2007–2018, measured as standardized incidence ratios (SIR) per CT for the study period. SIR is defined as a ratio of the number of observed cases to the number that would be expected, if the study population experienced the same incidence rates as the reference population. In our study, the reference population was the total population of Gran Canaria. An SIR was calculated for each CT, taking the number of cases and the CT population into account: SIRi = Observedi/Expectedi, where Oi is the observed number of cases, Ei = rPi is the expected number of cases, Pi is the population, and r = sum of (observed cases/total population) is the overall incidence ratio. An SIR of 1 indicated an incidence equal to that expected for the CT, based on the overall crude incidence in the island.
Skin melanoma incidence is known to increase with age. To account for the potential confounding effect that age composition per CT might have, expected counts were calculated for each age group category available at the census (< 16, 16 to 64, and > 64 years) and then added, to obtain an age-adjusted SIR (aSIR) = Observed cases/Age-adjusted expected cases, for each CT [28]. An aSIR of 1 indicates an incidence equal to that expected for the CT, taking into account the total population of the CT and its age composition. An aSIR > 1 indicates a higher incidence than expected, and an aSIR < 1 a lower incidence than expected.
Analysis of spatial clustering
We initially tested for global spatial autocorrelation with Moran’s I statistic using GeoDA software [29], to identify whether geographic variations in incidence were random or whether there was evidence for spatial clustering in the data.
The spatial weights matrix used to define the spatial relationships of the CTs was based on Queen’s contiguity, with a spatial lag of one (first-order adjacency). Queen contiguity defines neighbors as spatial units sharing a common edge or a common vertex and seemed more appropriate for Gran Canaria than the available alternatives due to the geographic variability of tracts in morphology and size. Monte Carlo simulation was performed in order to test the statistical significance of Moran’s I coefficient. 999 permutations were used to obtain more stable pseudo p-values.
In case evidence for spatial autocorrelation was found, local spatial autocorrelation with Local Moran’s I statistic (LISA) would be performed to check for the presence of clusters/outliers, and Monte Carlo methods applied again. We performed sensitivity analyses and increased the significance level to 0.01 to decrease the risk of false positives arising from multiple comparisons.
Bayesian statistical modeling
CTs are small areas, and limitations of SIR comparisons across small areas have previously been noted. Bayesian modeling methods allow to adjust for data from neighboring small areas and to obtain a quantification of the uncertainty around the estimates, improving former approaches [30]. Since the dataset was too sparse to fit a spatiotemporal model due to the relatively low melanoma incidence in the region, annual cases were aggregated to consider a spatial model for the whole study period (2007–2018).
We modeled the incidence of skin melanoma in Gran Canaria by fitting multivariable spatial generalized linear mixed models with inference in a Bayesian setting, using Integrated Nested Laplace Approximations. Models were implemented with INLA and CARBayes packages in R [22, 31, 32]. The response variable, aSIR, was fitted using multiple Bayesian Poisson models with a range of explanatory variables as potential risk factors (fixed effects) and different options for random effects with (i) no random effects (Model 1), (ii) independent random effects (Model 2), and (iii) spatially correlated random effects, implemented through a conditional autoregressive model (CAR, Model 3). Independent random effects are a tool conceived for modeling and structuring the sources of variability underlying the data [33]. Model 2, fitted with the effect of covariates and with independent random effects, provided a baseline to assess whether residual spatial dependence (added in model 3) was required to model the data [34]. Model 3 was fitted using the widely used Besag, York, and Mollié (BYM) spatial model [35, 36].
For the selection of covariates, based on previous evidence we decided a priori that an adjustment for age, sex, and SES needed to be included in the final model, apart from the effect of environmental variables that we aimed to test [3, 13]. Age was accounted for by modeling age-adjusted SIR, and sex by adjusting for percent of females per CT. For the other predictors, we explored the distribution of each covariate and fitted univariable models using simple Poisson regression without accounting for random effects. A correlogram of all covariates was performed to (i) evaluate the relationship between them, (ii) assess how the deprivation index IP2011 behaved compared to other SES measures in the region, and (iii) exclude correlated covariates in order to reduce the risk of collinearity and overfitting in the final model (see Supplementary Fig. S3). All covariates were scaled ((value-mean)/standard deviation) and then the selected ones fitted as fixed effects in all models.
The adequacy of the fitted models was explored using standard posterior predictive checks. A final comparison was made to select the best model using the deviance information criterion (DIC), i.e., the one with a lowest DIC [37]. Details on the specifications of these Bayesian Poisson models are given in the supplementary file (Supplementary Text T1).
Ethical clearances
The study was approved by the regional Research Ethics Committee (CEI/CEIm HUGCDN, Code 2019-515-1).
Results
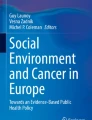
In the period 2007–2018, 1,058 skin melanoma cases were diagnosed among Gran Canaria residents, of which 1,055 (99.7%) could be ascribed to a CT and mapped. The overall incidence rate was of 10.4 cases per 100,000 person-years. The age-specific rate in the 16- to 64-year-old age stratum was of 9.4 cases per 100,000 person-years, while in people older than 64, the rate rose to 29.4. No cases were diagnosed in people younger than 16 in the whole study period. Age-adjusted SIR (aSIR) were obtained for each CT across the island, with a median of 0.77 (IQR 0.00–1.56) and a maximum value of 7.85. The distribution of aSIR across the island is presented in Fig. 1, where high values can be observed in some CTs of the capital city (LPGC) and following selected ravines of the island (Tirajana, Telde, Azuaje, and end of Guiniguada ravines, supplementary Fig. S1).

Choropleth map showing the incidence of skin melanoma in Gran Canaria Island and in the capital city of Las Palmas de Gran Canaria (LPGC) in 2007–2018, at the census-tract level.
Incidence presented as Age-adjusted Standardized Incidence Ratios (aSIR) per census tract (CT). An aSIR of 1 in a CT indicates an observed number of cases equal to that expected for the CT in the study period, based on the overall incidence in the island and considering the total population of the CT and its age composition. An aSIR > 1 indicates a higher incidence than expected, and aSIR < 1 a lower incidence than expected. An aSIR of 3 indicates an incidence 3 times higher than expected for the CT
We found evidence of spatial heterogeneity in the distribution of skin melanoma incidence across the island. Moran’s I coefficient of spatial global autocorrelation indicated positive clustering with SIR (I = 0.09, pseudo p-value = 0.001), meaning cases were more spatially clustered than expected by chance, and neighboring tracts tended to have more similar incidences than distant tracts. After adjusting for the effect of age using aSIR, there was still evidence for spatial autocorrelation although the magnitude was lower (I = 0.06, pseudo p-value = 0.009).
Figure 2 shows the results of the analysis of local spatial autocorrelation (LISA), highlighting CTs that are clustering based on measured aSIR. A few areas at increased risk (hot spots) were identified in the northern region of the island, particularly in Triana, an urban, high-SES area of LPGC and in neighborhoods of Agaete and Firgas municipalities. Clusters of low aSIR (cold spots) were also identified in more deprived, central rural neighborhoods of Tejeda and La Vega de San Mateo and in the northern municipality of Santa Maria de Guía (Fig. 2 and supplementary Figs. S1 and S2).

Cluster maps of skin melanoma incidence showing the type of spatial association between adjacent neighborhoods in Gran Canaria and in LPGC city in 2017–2018.
Local Indicator of Spatial Autocorrelation (LISA) cluster map. High–high and low–low indicate clustering of similar values and high–low and low–high indicate spatial outliers. Spatial weights with Queen’s contiguity of first order, with age-adjusted SIR as outcome and significance filter of p < 0.01
Maps showing the distribution of covariates at the CT level, and correlation plots of covariates are presented in supplementary Figs. S2 and S3. Regarding SES variables, IP2011 showed correlation (Pearson’s correlation coefficient > 0.5 or < -0.5) with both economic and educational attainment variables, including those from the SPHC2011 used to elaborate the index itself and with the supplementary economic covariates of Spain’s Household income distribution atlas. Therefore, IP2011 was selected as the covariate to adjust for SES in further modeling steps.
Urbanization, measured as the percentage of CT area covered by urban land, showed strong negative correlation with altitude, slope, and other land cover types and was selected as the single land cover and topographic variable, as it was deemed as potentially more relevant based on previous findings [38, 39]. Solar radiation and Hillshade did not show collinearity with other potential explanatory factors and were then selected for further analyses.
Bayesian Poisson regression models of aSIR were fitted with the selected explanatory covariates (deprivation index, percent of females, percent of urbanized land, solar radiation) and with different options for random effects implemented through a BYM CAR model. The model accounting for independent random effects (model 2) outperformed the model with only fixed effects (Table 1). There was no evidence of spatial autocorrelation in the residuals, indicating that the covariates reasonably accounted for the existing spatial structure in the aSIR.
Bayesian CAR models with spatially structured random effects (global and local spatial smoothing, models 3 and 4, respectively) did not show a significant improvement on model fit compared to the fitted model with independent random effects (Table 1). Therefore, the model with independent random effects was selected as the final model. Sex, deprivation index, and urbanicity were the covariates that better explained case distribution in the region (Table 2). We explored adding Hillshade as a covariate, but it did not improve model fit and led to slightly decreased dispersion of the residuals and was therefore discarded. Figure 3 shows the fitted aSIR values throughout Gran Canaria with the final model (modeled aSIR with fixed effects—the explanatory covariates—and with independent random effects).

Modeled skin melanoma incidence in Gran Canaria Island and in the city of Las Palmas de Gran Canaria (LPGC) in 2007–2018 at the census-tract level, with the final model.
A Fitted values of median aSIR with the Bayesian conditional autoregressive model accounting for fixed and independent random effects. B Lower and upper bounds of the 95% CI for modeled aSIR across the island. aSIR age-adjusted standardized incidence ratios, CI credible interval
Discussion
We found evidence of spatial heterogeneity in the distribution of skin melanoma incidence in Gran Canaria for the period 2007–2018, at the CT level (Moran’s I = 0.06, pseudo p-value = 0.009). Hot spots were identified in northern urban CTs, whereas a few cold spots clustered in central non-urban CTs (Figs. 1, 2). In the Bayesian multivariable model, a high SES and urbanicity were independently associated with an increased incidence (Table 2). This supports the existence of a social and an urban–rural gradient in melanoma incidence in the island and adds to the international body of evidence that high-SES populations present higher rates of skin melanoma [3].
Previous studies have suggested that high-SES populations might present higher rates of disease due to an easier access to recreational sun-related activities; hence, more sunburns and melanoma risk [3, 40, 41]. However, Gran Canaria is a sun-and-beach destination itself and the hypothesis of a differential accessibility to sun-related activities would not hold in this region. Additionally, low-SES CTs tended to suffer from higher solar radiation than high-SES ones (Supplementary Fig. S2), and lower-SES populations might struggle to buy sunscreen products. A differential sun-tanning behavior based on SES, with high-SES populations seeking sun tanning more intensively, rather than accessibility, could explain the social gradient in Gran Canaria [41].
Urbanicity was also associated with a higher incidence (Table 2). This is consistent with previous studies conducted in some Northern European countries and Canada [9, 38, 42]. Conversely, rurality was found to be a risk factor in Costa Rica [39], mostly linked to pesticide exposure. Urbanicity might also be associated with increased sun-seeking behaviors, with differential perceptions of tanned skin or clothing trends, posing individuals living in urban neighborhoods at an increased risk of melanoma [41]. Future qualitative studies in GC might help disentangle the mechanisms explaining these associations.
An alternative explanation of these social and urban–rural gradients might be the presence of a diagnostic access bias, with early-stage forms of melanoma going underdiagnosed in deprived and remote settings [3, 43]. Although Spain’s universal healthcare should make this hypothesis unlikely, a previous study showed that in northern Gran Canaria, a low educational attainment was associated with late-stage melanoma diagnoses [44]. Future research should aim at clarifying whether the aforementioned gradients reflect a health inequality [45].
The distribution of incidence was a revealing finding that might deserve further study. A radial pattern could be observed, overlapping to the ravines’ map of the island (Fig. 1 and supplementary Fig. S1). High values could be observed following the ravines of Tirajana, Telde, Azuaje, and end of Guiniguada. On the other hand, low values were found in the Arguineguín, Mogan, Tasartico, La Aldea, Moya, and Tenoya ravines. The regression model that showed better fitting of aSIR was a model with fixed effects (the selected explanatory covariates) and independent random effects. The latter, associated to each CT, are intended to account for any variance unexplained by the fixed effects and can be explained as unmeasured individual or CT factors which might have helped better explain the spatial distribution of skin melanoma (Table 1). Genetic and toxic factors are especially relevant in the epidemiology of geographically isolated areas, like islands [46], and might account for this uncaptured variability and explain this radial pattern. Historically, communication across the steep ravines was very difficult due to the lack of roads [47], favoring inbreeding and similar water supplies within ravines.
Distinct genetic populations might exist in Gran Canaria [48, 49] reflecting the influx of the varying ethnical groups that progressively populated the island. New mutations with founder effects have been discovered, with some genetic diseases clustering in particular ravines [50, 51]. Gran Canaria islanders are fundamentally of Spanish descent [52], due to the colonization process occurring in the fifteenth century by the Crown of Castile [49, 53, 54]. Settlers from Italy, Portugal, Flanders, and north African territories represented significant population influxes during the sixteenth century onward [55] and tended to group together according to origin [49, 55]. British communities followed later on, settling predominantly in urban regions of Gran Canaria capital city, LPGC [56,50,51,59]. Particularly, British merchants established in the commercial area of Triana and around the modern La Luz port [51, 57, 60] of LPGC, where a hotspot was identified (Fig. 2). Genetic susceptibility to melanoma is still poorly understood [61], and the particular distribution of cases in Gran Canaria, together with its anthropological evolution, might render the island a setting of particular interest for future genetic research.
An alternative explanation of the radial pattern could be related to water toxicity. Radon and pesticides have been attributed a potential causal role in skin melanoma [39, 62,56,64]. The cleanest waters of the island are considered to be in the top central areas of Tejeda and Artenara, where spring water is available. Those municipalities were classically the most isolated areas of the island, with the higher intensities of solar radiation, yet they constitute the predominant cold spot of incidence. Additionally, the Azuaje, Guiniguada, and Tirajana ravines (regions with high incidence) have long suffered from polluted waters [65,59,60,68]. A comparative study of water composition across ravines would allow to test potential associations between selected chemicals and skin melanoma occurrence. Future research should aim at clarifying whether genetic, toxic factors, or both might better explain the radial pattern of skin melanoma incidence in Gran Canaria.
Regarding the covariates used, this study supports the validity of IP2011 [19] as a measure to assess SES in Spain [69]. Despite SES being a multidimensional construct, most health studies have used a single variable to adjust for SES, either related with education, wealth, or occupation, but seldom integrating many of them, which might have led to biased adjustments [3, 70]. Deprivation indexes have been developed in some regions to overcome these limitations [71]. Until very recently, Spain had a deprivation index available for major cities [72] but not for the whole extension of the country. In this study, IP2011 correlated well with wealth and educational variables others than the ones used for its composition (Supplementary Fig. S3).
Our study has some limitations. First, the relatively low number of cases per year did not allow to evaluate the temporal fluctuations within the study period, nor to perform separate calculations for men and women. The effect of sex on incidence was therefore measured as percent of females per CT and the population denominator of the 2011 neighborhood considered as fixed for the entire study period, which might have produced residual confounding.
Second, our assessment of the role of solar radiation might not have provided an adequate measurement of the effect of this variable. Epidemiological studies using a small-area approach are ecologic, and exposure estimates of covariates are assigned to individuals based on location of residence. This approach has been validated for demographic and socio-economic variables [73], but might be more limited for solar radiation. Due to data availability, exposure was estimated at the place of residence, at the time of diagnosis. Yet a long spatial lag is expected between sun exposure and melanoma development [40, 74].
Finally, this study relies on the assumption that all incident skin melanoma cases diagnosed in Gran Canaria residents in the study period were considered. Because of how the dataset was elaborated, we have certainty that all cases diagnosed in the public healthcare system (CIHS) were included, but a few cases diagnosed in private practices might have been missed [13]. The CIHS covers about 87% of all healthcare in the region, and cases diagnosed in private clinics in our dataset represented 15.8%, that is, more than expected [13, 15]. Therefore, the plausible number of missing cases is unlikely to have meaningfully biased the results. Moreover, the uptake of private healthcare services in Spain is more common among high-SES individuals [75], and the plausible missing cases would be more likely to reside in high-SES neighborhoods, thereby increasing the effect estimates found.
Our study also has many strengths. The small-area approach used allowed the integration of individual-based health data and high-resolution small-area data, providing high-level granularity. This “semi-ecological” design is considered to allow a finer adjustment than traditional ecological studies, thereby diminishing the risk for ecological fallacy and improving causal inference [73].
The geospatial approach allowed disease mapping in Gran Canaria, providing the first identification of high- and low-risk areas in the region. It also establishes the role of demographic, socio-economic, and environmental variables in the relative risk of skin melanoma occurrence in Gran Canaria and provides new opportunities to assess their impact from a public health perspective [76]. Both the insularity and the anthropological evolution of Gran Canaria might provide a unique setting to test unresolved questions in melanoma epidemiology and pathogenesis.
Conclusion
We found evidence of spatial heterogeneity in the distribution of skin melanoma incidence in Gran Canaria in 2007–2018 at the CT level. High values were identified in northern urban CTs and in certain ravines of the island, whereas a few cold spots clustered in central non-urban territories. A high SES and urbanicity were independently associated with increased incidence. Future studies will need to address whether SES and urbanicity truly explain differential melanoma susceptibility in the region, or whether they might be the result of health inequalities in skin melanoma detection. The clustering of high values following some ravines with historical isolation might represent an opportunity for future discoveries of the potential role of genetic and toxic factors in melanoma pathogenesis.
Data availability
The data that support the findings of this study are available on reasonable request from the corresponding author (aggregated data). The data are not publicly available due to privacy or ethical restrictions.
References
The Global Cancer Observatory—International Agency for Research on Cancer Melanoma of Skin—Globocan (2020) https://gco.iarc.fr/today/data/factsheets/cancers/16-Melanoma-of-skin-fact-sheet.pdf. Accessed 23 Sept 2021
Gandini S, Sera F, Cattaruzza MS et al (2005) Meta-analysis of risk factors for cutaneous melanoma: I. Common and atypical naevi. Eur J Cancer 41:28–44. https://doi.org/10.1016/J.EJCA.2004.10.015
Jiang A, Rambhatla P, Eide M (2015) Socioeconomic and lifestyle factors and melanoma: a systematic review. Br J Dermatol 172:885–915. https://doi.org/10.1111/bjd.13500
Whiteman DC, Green AC, Olsen CM (2016) The growing burden of invasive melanoma: projections of incidence rates and numbers of new cases in six susceptible populations through 2031. J Investig Dermatol 136:1161–1171. https://doi.org/10.1016/j.jid.2016.01.035
Eklund G, Malec E (1978) Sunlight and incidence of cutaneous malignant melanoma: effect of latitude and domicile in Sweden. Scand J Plast Reconstr Surg 12:231–241. https://doi.org/10.3109/02844317809012999
Bulliard J-L, Cox B, Elwood JM (1994) Latitude gradients in melanoma incidence and mortality in the non-Maori population of New Zealand. Cancer Causes Control 5:234–240
Gandini S, Sera F, Cattaruzza MS et al (2005) Meta-analysis of risk factors for cutaneous melanoma: II. Sun exposure. Eur J Cancer 41:45–60. https://doi.org/10.1016/j.ejca.2004.10.016
Pearce J, Barnett R, Kingham S (2006) Slip! Slap! Slop! Cutaneous malignant melanoma incidence and social status in New Zealand, 1995–2000. Heal Place 12:239–252. https://doi.org/10.1016/j.healthplace.2004.11.006
Augustin J, Kis A, Sorbe C et al (2018) Epidemiology of skin cancer in the German population: impact of socioeconomic and geographic factors. J Eur Acad Dermatol Venereol 32:1906–1913. https://doi.org/10.1111/jdv.14990
Kirby RS, Delmelle E, Eberth JM (2017) Advances in spatial epidemiology and geographic information systems. Ann Epidemiol 27:1–9. https://doi.org/10.1016/j.annepidem.2016.12.001
Sahar L, Foster SL, Sherman RL et al (2019) GIScience and cancer: state of the art and trends for cancer surveillance and epidemiology. Cancer 125:cncr.32052. https://doi.org/10.1002/cncr.32052
Utrillas MP, Marín MJ, Esteve AR et al (2013) Ten years of measured UV Index from the Spanish UVB Radiometric Network. J Photochem Photobiol B Biol 125:1–7. https://doi.org/10.1016/j.jphotobiol.2013.04.005
Grau-Pérez M, Carretero G, Almeida P et al (2021) The incidence of skin melanoma in Gran Canaria (Canary Islands, Spain) is lower than expected in Southern Europe despite high-risk environmental conditions: an island-wide cross-sectional study. Cancer Causes Control 32:525–535. https://doi.org/10.1007/s10552-021-01403-7
Ravines and Basins (2011) Consejo Insular de Aguas de Gran Canaria. http://www.aguasgrancanaria.com/cartografia/medio_fisico/barrancos_cuencas.php. Accessed 5 Jan 2022
Spain’s National Institute of Statistics INE (2017) National Health Survey https://www.ine.es/dyngs/INEbase/en/operacion.htm?c=Estadistica_C&cid=1254736176783&menu=resultados&secc=1254736195650&idp=1254735573175#!tabs-1254736195650. Accessed 4 May 2020
Bray F, Kohler B, Ferlay J (2014) Chapter 5: Data comparability and quality. In: Forman D, Bray F, Brewster DH, et al (eds) Cancer Incidence in Five Continents Vol X. International Agency for Research on Cancer, Lyon, France, pp 89–92
Spain's National Institute of Statistics INE (2013) Population and Housing Census 2011. https://www.ine.es/en/censos2011_datos/cen11_datos_resultados_seccen_en.htm. Accessed 10 Dec 2020
Spain's National Institute of Statistics INE (2020) Spain's Household Income Distribution Atlas. https://www.ine.es/dynt3/inebase/en/index.htm?padre=7132. Accessed 9 Feb 2022
Duque I, Domínguez-Berjón MF, Cebrecos A et al (2021) Deprivation index by enumeration district in Spain 2011. Gac Sanit 35:113–122. https://doi.org/10.1016/j.gaceta.2019.10.008
European Union, Copernicus Land Monitoring Service (2018) European Environment Agency (EEA). CORINE Land Cover, European Environment Agency (EEA), CLC
Fick SE, Hijmans RJ (2017) WorldClim 2: new 1-km spatial resolution climate surfaces for global land areas. Int J Climatol 37:4302–4315. https://doi.org/10.1002/joc.5086
R Core Team (2020) R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria. https://www.r-project.org/
Kahle D, Wickham H. ggmap: Spatial Visualization with ggplot2. The R Journal, 5(1):144–161. http://journal.r-project.org/archive/2013-1/kahle-wickham.pdf
Possenriede D, Sadler J, Salmon M (2018) Opencage: Geocode with the OpenCage API. https://cran.r-project.org/package=opencage
Environmental Systems Research Institute (2021) ArcGIS Pro version 10.8. Esri Inc., Redlands, CA
Hijmans RJ (2021) raster: Geographic data analysis and modeling. https://cran.r-project.org/package=raster
Van Buuren S, Groothuis-Oudshoorn K (2011) mice : Multivariate Imputation by Chained Equations in R. J Stat Softw 45:1–67. https://doi.org/10.18637/jss.v045.i03
La Morte WW (2016) Standardized Incidence Ratios - Boston University School of Public Health. In: Stand. Rates Dis. https://sphweb.bumc.bu.edu/otlt/mph-modules/ep/ep713_standardizedrates/EP713_StandardizedRates6.html. Accessed 29 Sept 2021
Anselin L, Syabri I, Kho Y (2006) GeoDa: an introduction to spatial data analysis. Geogr Anal 38:5–22. https://doi.org/10.1111/j.0016-7363.2005.00671.x
Cramb SM, Mengersen KL, Baade PD (2011) Developing the atlas of cancer in Queensland: methodological issues. Int J Health Geogr 10:9. https://doi.org/10.1186/1476-072X-10-9
Lee D (2013) CARBayes: an R package for Bayesian spatial modeling with conditional autoregressive priors. J Stat Softw 55:1–24. https://doi.org/10.18637/jss.v055.i13
Rue H, Martino S, Chopin N (2009) Approximate Bayesian inference for latent Gaussian models by using integrated nested Laplace approximations. J R Stat Soc Ser B (Stat Methodol) 71:319–392. https://doi.org/10.1111/j.1467-9868.2008.00700.x
Martinez-Beneito MA, Botella-Rocamora P (2019) Some basic ideas of Bayesian inference. In: Martinez-Beneito MA, Botella-Rocamora P (eds) Disease mapping: from foundations to multidimensional modeling. Chapman and Hall/CRC, Boca Raton, FL, pp 15–50
Gómez-Rubio V (2020) Spatial models. In: Gómez-Rubio V (ed) Bayesian Inference with INLA. Chapman & Hall/CRC Press, Boca Raton, FL
Besag J, York J, Mollié A (1991) Bayesian image restoration, with two applications in spatial statistics. Ann Inst Stat Math 43:1–20. https://doi.org/10.1007/BF00116466
Martinez-Beneito MA, Botella-Rocamora P (2019) 4.3 Spatial smoothing. In: Martínez-Beneito MA, Botella-Rocamora P (eds) Disease Mapping: from foundations to multidimensional modeling. CRC Press, Boca Raton, FL, pp 131–178
Spiegelhalter DJ, Best NG, Carlin BP, van der Linde A (2002) Bayesian measures of model complexity and fit. J R Stat Soc Ser B (Stat Methodol) 64:583–639. https://doi.org/10.1111/1467-9868.00353
Johnson-Obaseki SE, Labajian V, Corsten MJ, McDonald JT (2015) Incidence of cutaneous malignant melanoma by socioeconomic status in Canada: 1992–2006. J Otolaryngol Head Neck Surg 44:53. https://doi.org/10.1186/s40463-015-0107-1
Wesseling C, Antich D, Hogstedt C et al (1999) Geographical differences of cancer incidence in Costa Rica in relation to environmental and occupational pesticide exposure. Int J Epidemiol 28:365–374. https://doi.org/10.1093/ije/28.3.365
Menzies SW (2008) Is sun exposure a major cause of melanoma? Yes. BMJ 337:a763. https://doi.org/10.1136/bmj.a763
Chang C, Murzaku EC, Penn L et al (2014) More skin, more sun, more tan, more melanoma. Am J Public Health 104:e92–e99. https://doi.org/10.2105/AJPH.2014.302185
Pérez-Gómez B, Aragonés N, Gustavsson P et al (2008) Socio-economic class, rurality and risk of cutaneous melanoma by site and gender in Sweden. BMC Public Health 8:33. https://doi.org/10.1186/1471-2458-8-33
Banerjee A, O’Sullivan J, Pluddemann A, Spencer E Catalogue of Bias Collaboration (2017) Diagnostic access bias. In: Cat. Biases. https://catalogofbias.org/biases/diagnostic-access-bias/. Accessed 27 Jan 2022
Grau-Pérez M, Cabello C, González-Martín J-M et al (2019) Low educational attainment is still associated with late melanoma diagnosis: a cross-sectional study from a European setting with universal healthcare. Cancer Epidemiol 62:101576. https://doi.org/10.1016/j.canep.2019.101576
Strömberg U, Parkes BL, Holmén A et al (2020) Disease mapping of early- and late-stage cancer to monitor inequalities in early detection: a study of cutaneous malignant melanoma. Eur J Epidemiol 35:537–547. https://doi.org/10.1007/s10654-020-00637-0
Rudan I, Campbell H, Rudan P (1999) Genetic epidemiological studies of eastern Adriatic Island isolates, Croatia: objective and strategies. Coll Antropol 23:531–546
Domínguez Mujica J, Moreno Medina CJ (2004) Pervivencias y cambios en el poblamiento de Gran Canaria (1857–2001). In: XVI Coloquio de Historia Canario-Americana, pp. 102–145
Fuste M (1958) Some observations about the Anthropology of the prehistorical and current populations of Gran Canaria [in Spanish]. El Museo Canario 19-20(65):1–32
Fuste M (1965) Physical anthropology of the Canary Islands: old and new views. Am J Phys Anthropol 23:285–291. https://doi.org/10.1002/ajpa.1330230316
García-Villarreal L, Daniels S, Shaw SH et al (2000) High prevalence of the very rare wilson disease gene mutation Leu708Pro in the Island of Gran Canaria (Canary Islands, Spain): a genetic and clinical study. Hepatology 32:1329–1336. https://doi.org/10.1053/jhep.2000.20152
Peña-Quintana L, Scherer G, Curbelo-Estévez ML et al (2017) Tyrosinemia type II: mutation update, 11 novel mutations and description of 5 independent subjects with a novel founder mutation. Clin Genet 92:306–317. https://doi.org/10.1111/cge.13003
Flores C, Maca-Meyer N, Perez JA et al (2003) A predominant European ancestry of paternal lineages from canary islanders. Ann Hum Genet 67:138–152. https://doi.org/10.1046/j.1469-1809.2003.00015.x
Maca-Meyer N, Arnay M, Rando JC et al (2004) Ancient mtDNA analysis and the origin of the Guanches. Eur J Hum Genet 12:155–162. https://doi.org/10.1038/sj.ejhg.5201075
Santana-Cabrera J, Velasco-Vázquez J, Rodríguez-Rodríguez A et al (2016) The paths of the european conquest of the atlantic: osteological evidence of warfare and violence in Gran Canaria (XV Century). Int J Osteoarchaeol 26:767–777. https://doi.org/10.1002/oa.2476
Lobo Cabrera M (1979) Human groups in the Canarian society of the 16th century [In Spanish]. Mancomunidad de Cabildos, Plan Cultural y Museo Canario, Las Palmas de Gran Canaria
La Luz Port (2020) La Luz Port History. https://www.laluzport.com/MAIN_folder/HISTORY/laluzhistory.html. Accessed 7 Jan 2022
Quintana Navarro F (1996) La Luz Port, 1883–1983: an international scale Port prototype [In Spanish]. Bol. Agustín Millares Carló 15:187–195
Quintana Navarro F (1992) British interests in the Canary Islands in the 1930s: an approach [in Spanish]. Vegueta Anu Fac Geogr Hist 149–172
González Cruz I (2012) English in the Canaries: past and present. English Today 28:20–28. https://doi.org/10.1017/S0266078411000642
Iglesias Fernandez M (1985) Foreigners in Gran Canaria in the first third of the XVIII century [in Spanish]. Santa Cruz de Tenerife
Landi MT, Bishop DT, MacGregor S et al (2020) Genome-wide association meta-analyses combining multiple risk phenotypes provide insights into the genetic architecture of cutaneous melanoma susceptibility. Nat Genet 52:494–504. https://doi.org/10.1038/s41588-020-0611-8
Kulich M, Řeřicha V, Řeřicha R et al (2011) Incidence of non-lung solid cancers in Czech uranium miners: a case–cohort study. Environ Res 111:400–405. https://doi.org/10.1016/j.envres.2011.01.008
Vienneau D, de Hoogh K, Hauri D et al (2017) Effects of radon and UV exposure on skin cancer mortality in Switzerland. Environ Health Perspect 125:067009. https://doi.org/10.1289/EHP825
Wheeler BW, Allen J, Depledge MH, Curnow A (2012) Radon and skin cancer in southwest England: an ecologic study. Epidemiology 23:44–52. https://doi.org/10.1097/EDE.0B013E31823B6139
Navarro E, Alonso J, Concha K et al (2016) Actividad diurética de las aguas minerales termales del balneario de Azuaje (Gran Canaria, Islas Canarias). Bol Soc Española Hidrol Medica 31:65–72. https://doi.org/10.23853/bsehm.2017.0205
Naranjo Ayala G (2009) Hydrogeological study of the Guiniguada and Tenoya creeks (Gran Canaria) [in Spanish]. Universidad de Las Palmas de Gran Canaria
Ruiz-García, Carrascosa-Chisvert, Mena et al (2019) Groundwater quality assessment in a volcanic mountain range (South of Gran Canaria Island, Spain). Water 11:754. https://doi.org/10.3390/w11040754
Alonso H, Cruz-Fuentes T, Rubiano J et al (2015) Radon in groundwater of the Northeastern Gran Canaria Aquifer. Water 7:2575–2590. https://doi.org/10.3390/w7062575
Allik M, Leyland A, Travassos Ichihara MY, Dundas R (2020) Creating small-area deprivation indices: a guide for stages and options. J Epidemiol Community Health 74:20–25. https://doi.org/10.1136/jech-2019-213255
Braveman PA, Cubbin C, Egerter S et al (2005) Socioeconomic status in health research. JAMA 294:2879. https://doi.org/10.1001/jama.294.22.2879
Phillips RL, Liaw W, Crampton P et al (2016) How other countries use deprivation indices—and why the united states desperately needs one. Health Aff 35:1991–1998. https://doi.org/10.1377/hlthaff.2016.0709
Domínguez-Berjón MF, Borrell C, Cano-Serral G et al (2008) Constructing a deprivation index based on census data in large Spanish cities (the MEDEA project) [in Spanish]. Gac Sanit 22:179–187. https://doi.org/10.1157/13123961
Piel FB, Fecht D, Hodgson S et al (2020) Small-area methods for investigation of environment and health. Int J Epidemiol 49:686–699. https://doi.org/10.1093/ije/dyaa006
Shuster S (2008) Is sun exposure a major cause of melanoma? No. BMJ 337:a764. https://doi.org/10.1136/bmj.a764
Lostao L, Blane D, Gimeno D et al (2014) Socioeconomic patterns in use of private and public health services in Spain and Britain: implications for equity in health care. Health Place 25:19–25. https://doi.org/10.1016/j.healthplace.2013.09.011
Schootman M, Gomez SL, Henry KA et al (2017) Geospatial approaches to cancer control and population sciences. Cancer Epidemiol Biomark Prev 26:472–475. https://doi.org/10.1158/1055-9965.EPI-17-0104
Acknowledgments
This study is part of the PhD degree of Mercè Grau-Pérez at Universidad de Las Palmas de Gran Canaria (ULPGC), Las Palmas de Gran Canaria, Spain. We thank Prof. Manuel Lobo Cabrera and Prof. Francisco Quintana Navarro, Professors of Modern and of Contemporary History respectively at ULPGC, for their insightful comments on the geography and settlement of Gran Canaria.
Funding
Open Access funding provided thanks to the CRUE-CSIC agreement with Springer Nature. No funds, grants, or other support were received for conducting this study.
Author information
Authors and Affiliations
Contributions
MGP and JC conceptualized the project and were responsible for study design and data analysis. Data collection was performed by MGP, GC, PA, and JC. MGP prepared the first draft of the manuscript. LB, GC, and JC were responsible for supervision and for critical review of the manuscript. All authors reviewed and approved the final draft.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to declare that are relevant to the content of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Grau-Pérez, M., Borrego, L., Carretero, G. et al. Assessing the effect of environmental and socio-economic factors on skin melanoma incidence: an island-wide spatial study in Gran Canaria (Spain), 2007–2018. Cancer Causes Control 33, 1261–1272 (2022). https://doi.org/10.1007/s10552-022-01614-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-022-01614-6