
Abstract
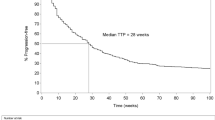
To determine if a low fixed dosing strategy of capecitabine would produce comparable clinical activity with less adverse toxicities compared to published data with higher doses in the setting of metastatic breast cancer (mBC). We retrospectively analyzed patients treated with a low fixed dose of capecitabine (CAPE-L) at 1,000 mg twice daily for 14 days every 21 days. Outcomes included clinical benefit rate (CBR), overall response rates (ORR), time to progression (TTP), and overall survival (OS). A historical comparison group of mBC patients treated on 12 prior trials at the package-insert dose of capecitabine (n = 1,949) was utilized. Eighty-six patients were analyzed in our cohort. Positive hormone receptor status (79.1 vs. 50.6 %), and capecitabine as first-line chemotherapy (44.2 vs. 16.5 %) were more frequent in our cohort relative to the historical comparison. The median starting dose in our cohort was 633.5 mg/m2. The CBR was similar between the CAPE-L and the standard dose cohorts (55.8 vs. 49.5 %), as was ORR (24.3 vs. 24 %), and median TTP (7 mo, 95 % CI 5.5–8.5 vs. 5.1 mo, 95 % CI 4.5–5.7). Median OS was longer in our cohort (24 mo, 95 % CI 16.8–31.2) than the historic standard dose cohort (12.1 mo, 95 % CI 9.6–14.4), a difference that was likely explained by the higher proportion of patients in the CAPE-L cohort who received capecitabine as first-line chemotherapy and who had hormone receptor positive disease. As expected, adverse events were less frequent with CAPE-L. We found that CAPE-L, which translates into a dose of 600–650 mg/m2, appeared to have good clinical efficacy and acceptable toxicity.
Similar content being viewed by others


References
Mackean M, Planting A, Twelves C et al (1998) Phase I and pharmacologic study of intermittent twice-daily oral therapy with capecitabine in patients with advanced and/or metastatic cancer. J Clin Oncol 16:2977–2985
Miwa M, Ura M, Nishida M et al (1998) Original paper design of a novel oral fluoropyrimidine carbamate, capecitabine, which generates 5-fluorouracil selectively in tumours by enzymes concentrated in human liver and cancer tissue. Eur J Cancer 34:1274–1281
Beslija S, Bonneterre J, Burstein H et al (2007) Second consensus on medical treatment of metastatic breast cancer. Ann Oncol 18:215–225. doi:10.1093/annonc/mdl155
O’Shaughnessy J, Kaufmann M, Siedentopf F et al (2012) Capecitabine monotherapy: review of studies in first-line HER-2-negative metastatic breast cancer. Oncologist 17:476–484. doi:10.1634/theoncologist.2011-0281
Debled M, Madranges N, Trainaud A et al (2009) First-line capecitabine monotherapy for slowly progressing metastatic breast cancer: do we need aggressive treatment? Oncology 77:318–327. doi:10.1159/000260904
Stockler MR, Harvey VJ, Francis P et al (2011) Capecitabine versus classical cyclophosphamide, methotrexate, and fluorouracil as first-line chemotherapy for advanced breast cancer. J Clin Oncol 29:4498–4504. doi:10.1200/JCO.2010.33.9101
O’Shaughnessy J, Blum J, Moiseyenko V et al (2001) Randomized, open-label, phase II trial of oral capecitabine (Xeloda®) vs. a reference arm of intravenous CMF (cyclophosphamide, methotrexate and 5-fluorouracil) as first-line therapy for advanced/metastatic breast cancer. Ann Oncol 12(9):1247–1254
Zielinski C, Gralow J, Martin M (2010) Optimising the dose of capecitabine in metastatic breast cancer: confused, clarified or confirmed? Ann Oncol 21:2145–2152. doi:10.1093/annonc/mdq069
O’Shaughnessy, Joyce; Blum J (2000) A retrospective evaluation of the impact of dose reduction in patients treated with xeloda (capecitabine). Proc Am Soc Clin Oncol. 19:2000 (abstr 400)
Blum J (2001) Capecltabine (xeloda) in 162 patients with MBC: updated results and analysis of dose modification. J Clin Oncol 17:S190
Bajetta E, Procopio G, Celio L et al (2005) Safety and efficacy of two different doses of capecitabine in the treatment of advanced breast cancer in older women. J Clin Oncol 23:2155–2161. doi:10.1200/JCO.2005.02.167
Kaufmann M, Sütterlin MW, Schrader I et al (2009) 5002 MoniCa: a multicenter phase II study to determine the efficacy of capecitabine as first line monochemotherapy in patients with HER2 negative, medium-risk, metastatic breast cancer (GBG39). Eur J Cancer Suppl 7:260. doi:10.1016/S1359-6349(09)70894-8
Rossi D, Alessandroni P, Catalano V et al (2007) Safety profile and activity of lower capecitabine dose in patients with metastatic breast cancer. Clin Breast Cancer 7:857–860
El-Helw L, Coleman RE (2005) Reduced dose capecitabine is an effective and well-tolerated treatment in patients with metastatic breast cancer. Breast 14:368–374. doi:10.1016/j.breast.2004.12.005
Sezgin C, Kurt E, Evrensel T et al (2007) Efficacy of lower dose capecitabine in patients with metastatic breast cancer and factors influencing therapeutic response and outcome. South Med J 100:27–32
Yap YS, Kendall A, Walsh G et al (2007) Clinical efficacy of capecitabine as first-line chemotherapy in metastatic breast cancer—how low can you go? Breast 16:420–424. doi:10.1016/j.breast.2007.01.012
Venturini M, Paridaens R, Rossner D et al (2007) An open-label, multicenter study of outpatient capecitabine monotherapy in 631 patients with pretreated advanced breast cancer. Oncology 72:51–57. doi:10.1159/000111094
Fumoleau P, Largillier R, Clippe C et al (2004) Multicentre, phase II study evaluating capecitabine monotherapy in patients with anthracycline- and taxane-pretreated metastatic breast cancer. Eur J Cancer 40:536–542. doi:10.1016/j.ejca.2003.11.007
Wist E, Sommer HH, Ostenstad B et al (2004) Oral capecitabine in anthracycline- and taxane-pretreated advanced/metastatic breast cancer. Acta Oncol (Madr) 43:186–189. doi:10.1080/02841860310023165
Reichardt P, von Minckwitz G, Thuss-Patience PC et al (2003) Multicenter phase II study of oral capecitabine (Xeloda) in patients with metastatic breast cancer relapsing after treatment with a taxane-containing therapy. Ann Oncol 14:1227–1233. doi:10.1093/annonc/mdg346
Talbot D, Moiseyenko V, Van Belle S et al (2002) Randomised, phase II trial comparing oral capecitabine (Xeloda®) with paclitaxel in patients with metastatic/advanced breast cancer pretreated with anthracyclines. Br J Cancer 86(9):1367–1372. doi:10.1038/sj/bjc/6600261
Blum J, Jones S, Buzdar A et al (1999) Multicenter phase II study of capecitabine in paclitaxel-refractory metastatic breast cancer. J Clin Oncol 17:485–493
Blum JL, Ph D, Mucci P et al (2001) Multicenter, phase II study of capecitabine in taxane-pretreated metastatic breast carcinoma patients. Cancer 92:1759–1768
Geyer C, Forster J, Lindquist D et al (2006) Lapatinib plus capecitabine for HER2-positive advanced breast cancer. N Engl J Med 355:2733–2743
Thomas ES, Gomez HL, Li RK et al (2007) Ixabepilone plus capecitabine for metastatic breast cancer progressing after anthracycline and taxane treatment. J Clin Oncol 25:5210–5217. doi:10.1200/JCO.2007.12.6557
Von Minckwitz G, du Bois A, Schmidt M et al (2009) Trastuzumab beyond progression in human epidermal growth factor receptor 2-positive advanced breast cancer: a german breast group 26/breast international group 03–05 study. J Clin Oncol 27:1999–2006. doi:10.1200/JCO.2008.19.6618
Largillier R, Fumoleau P, Clippe C et al (2006) Capecitabine (X) monotherapy after anthracycline and taxane failure in metastatic breast cancer (MBC): long-term survival data. Ann Oncol 17:(abstr 161P)
Miller KD, Chap LI, Holmes FA et al (2005) Randomized phase III trial of capecitabine compared with bevacizumab plus capecitabine in patients with previously treated metastatic breast cancer. J Clin Oncol 23:792–799. doi:10.1200/JCO.2005.05.098
Hennessy BT, Gauthier AM, Michaud LB et al (2005) Lower dose capecitabine has a more favorable therapeutic index in metastatic breast cancer: retrospective analysis of patients treated at M. D. Anderson Cancer Center and a review of capecitabine toxicity in the literature. Ann Oncol 16:1289–1296. doi:10.1093/annonc/mdi253
Blum J, Feldman N, Verma S et al (2012) Pooled analysis of individual patient data from capecitabine monotherapy clinical trials in locally advanced or metastatic breast cancer. Breast Cancer Res Treat 136(3):777–788. doi:10.1007/s10549-012-2288-x
Jäger E, Al-Batran S, Schmidt M et al (2010) A randomized phase III study evaluating pegylated liposomal doxorubicin (PLD) versus capecitabine (CAP) as first-line therapy for metastatic breast cancer (MBC): results of the PELICAN study. J Clin Oncol 28(suppl):1022
Kaufmann M, Maass N, Costa SD et al (2010) First-line therapy with moderate dose capecitabine in metastatic breast cancer is safe and active: results of the MONICA trial. Eur J Cancer 46:3184–3191. doi:10.1016/j.ejca.2010.07.009
Taguchi T, Nakayama T, Masuda N et al (2010) Study of low-dose capecitabine monotherapy for metastatic breast cancer. Chemotherapy 56:166–170. doi:10.1159/000313531
Traina TA, Dugan U, Higgins B et al (2010) Optimizing chemotherapy dose and schedule by Norton–Simon mathematical modeling. Breast Dis 31:7–18. doi:10.3233/BD-2009-0290.Optimizing
Traina TA, Theodoulou M, Feigin K et al (2008) Phase I study of a novel capecitabine schedule based on the Norton–Simon mathematical model in patients with metastatic breast cancer. J Clin Oncol 26:1797–1802. doi:10.1200/JCO.2007.13.8388
Vogel CL, Azevedo S, Hilsenbeck S et al (1992) Survival after first recurrence of breast cancer. The Miami experience. Cancer 70:129–135
Conflict of interest
Dr. Mahtani has held consultant/advisory role for Genetech. Dr. Vogel has received remuneration from Roche and Genetech. Dr. Vogel has held consultant/advisory role for Roche. The remaining authors state that they have no conflict on interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Ambros, T., Zeichner, S.B., Zaravinos, J. et al. A retrospective study evaluating a fixed low dose capecitabine monotherapy in women with HER-2 negative metastatic breast cancer. Breast Cancer Res Treat 146, 7–14 (2014). https://doi.org/10.1007/s10549-014-3003-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-014-3003-x