
Summary
Background
Primary spontaneous pneumothorax (PSP) is a common medical condition in the emergency department. Clinically stable patients with large pneumothoraces usually undergo chest tube drainage. During the course of hospital stay, several chest X-rays are ordered at various time points. Because the number of chest X-rays during diagnosis and management of PSP can be quite high and lung ultrasound has a proven efficacy for the assessment of lung re-expansion, we decided to investigate the use of lung ultrasound for the management and decision-making regarding chest drains for PSP.
Material and methods
A total of 25 patients with PSP were evaluated. A comparison between chest X-rays and lung ultrasound was made at four different time points during patient hospitalization (T1—immediately after drainage, T2–third or fourth post-drainage day, T3—before chest tube removal, T4—after chest tube removal). The rate of agreement between the two investigations was analyzed, as their result impacts decision-making regarding chest tube management and removal.
Results
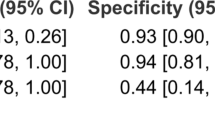
Overall, positive and negative agreements were high in all time points, except time point 3. Calculated p values using Fisher’s and Barnard’s test were also good for time points 1, 2, and 4 (< 0.05).
Conclusions
For all time points except the third, we can safely reject the null hypothesis, thereby arriving at the conclusion that lung ultrasound can substitute chest X-rays after tube drainage of PSP.




Similar content being viewed by others


References
Melton LJ 3rd, Hepper NG, Offord KP. Incidence of spontaneous pneumothorax in Olmsted County, Minnesota: 1950 to 1974. Am Rev Respir Dis. 1979;120:1379–82.
Baumann MH, Strange C. Treatment of spontaneous pneumothorax: a more aggressive approach? Chest. 1997;112:789–804.
Baumann MH, Strange C. The clinician’s perspective on pneumothorax management. Chest. 1997;112:822–8.
Baumann MH, et al. Management of spontaneous pneumothorax: an American College of Chest Physicians Delphi consensus statement. Chest. 2001;119:590–602.
Koenig SJ, Narasimhan M, Mayo PH. Thoracic ultrasonography for the pulmonary specialist. Chest. 2011;140(5):1332–41.
Gargani L, Volpicelli G. How I do it: lung ultrasound. Cardiovasc Ultrasound. 2014;12(1):25.
Volpicelli G, Elbarbary M, Blaivas M, et al., International Liaison Committee on Lung Ultrasound (ILC-LUS) for International Consensus Conference on Lung Ultrasound (ICC-LUS) (2012) International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 38:577–91.
Berlet T, Fehr T, Merz TM. Current practice of lung ultrasonography (LUS) in the diagnosis of pneumothorax: a survey of physician sonographers in Germany. Crit Ultrasound J. 2014;6(1):16.
Lichtenstein DA, Menu Y. A bedside ultrasound sign ruling-out pneumothorax in the critically ill. Lung sliding. Chest. 1995;108:1345–8.
Marusteri M, Bacarea V. Comparing groups for statistical differences: how to choose the right statistical test? Biochem Med. 2010;20(1):15–32.
Bipasa B Assessing agreement for diagnostic devices. FDA/Industry Statistics Workshop. 2006.
Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1(8476):307–10.
Longo D, Fauci A, Kasper D, Hauser S, Jameson J, Loscalzo J. Harrison’s principles of internal medicine. McGraw Hill, New York. 2008.
Jakobson DJ, Iftach S. Merging ultrasound in the intensive care routine. Isr Med Assoc J. 2013;15:688–92.
Chira R, Chira A, Săplăcan R, et al. Pleural ultrasonography. Pictorial essay. Med Ultrason. 2014;16(4):364–71.
Lichtenstein DA, Meziere G, Lascols N, et al. Ultrasound diagnosis of occult pneumothorax. Crit Care Med. 2005;33:1231–8.
Lichtenstein DA, Lascols N, Prin S, et al. The lung pulse: an early ultrasound sign of complete atelectasis. Intensive Care Med. 2003;29:2187–92.
Agricola E, Bove T, Oppizzi M, et al. Ultrasound comet-tail images: a marker of pulmonary edema. A comparative study with wedge pressure and extravascular lung water. Chest. 2005;127:1690–5.
Lichtenstein D, Meziere G, Biderman P, et al. The comet-tail artifact, an ultrasound sign ruling out pneumothorax. Intensive Care Med. 1999;25:383–8.
Lichtenstein DA, Meziere G, Biderman P, et al. The lung point: an ultrasound sign specific to pneumothorax. Intensive Care Med. 2000;26:1434–40.
Monti JD, Younggren B, Blankenship R. Ultrasound detection of pneumothorax with minimally trained sonographers: a preliminary study. J Spec Oper Med. 2009;9:43–6.
Lavingia KS, Soult MC, Collins JN, et al. Basic ultrasound training can replace chest radiography for safe tube thoracostomy removal. Am Surg. 2014;80(8):783–6.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Constantin, V., Carap, A., Zaharia, L. et al. High correlation of lung ultrasound and chest X-ray after tube drainage in patients with primary spontaneous pneumothorax: can we omit X-rays for tube management?. Eur Surg 47, 175–180 (2015). https://doi.org/10.1007/s10353-015-0333-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10353-015-0333-9