
Abstract
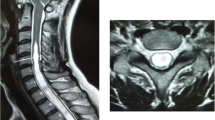
The occurrence of subdural cerebrospinal fluid collections and ventricular dilatation (external hydrocephalus) after foramen magnum decompression is extremely rare. The authors report on a 37-year-old man who developed symptomatic subdural fluid collections (SFC) after uncomplicated foramen magnum decompression for Chiari I–syringomyelia complex. Postoperative magnetic resonance imaging revealed a supratentorial SFC with prominent midline shift. In addition, bilateral infratentorial SFCs extending supratentorially through the tentorial notch, pseudomeningocele and initial shrinkage of the syrinx were observed. Few days after evacuation of supratentorial collection, the patient experienced increasing headache and a computerized tomography scan demonstrated a contralateral subdural collection as well as ventricular dilatation. A programmable ventriculoperitoneal shunt was placed with resolution of supratentorial collection and progressive improvement of infratentorial collections and pseudomeningocele. Although previous reports described the occurrence of extra-axial fluid collections and hydrocephalus after foramen magnum decompression for Chiari malformation, to our knowledge, this is the only report of acute external hydrocephalus after foramen magnum decompression requiring urgent evacuation of SFC in order to reduce the mass effect.




Similar content being viewed by others


References
Anderson H, Elfverson J, Svendsen P (1984) External hydrocephalus in infants. Childs Brain 11:398–402
Aoki N (1994) Extracerebral fluid collections in infancy: role of magnetic resonance imaging in differentiation between subdural effusion and subarachnoid space enlargement. J Neurosurg 81:20–23
Cardoso ER, Schubert R (1996) External hydrocephalus in adults. Report of three cases. J Neurosurg 85:1143–1147
Elton S, Tubbs RS, Wellons JC III, Blount JP, Grabb PA, Oakes WJ (2002) Acute hydrocephalus following a Chiari decompression. Pediatr Neurosurg 36:101–104
Huh PW, Yoo DS, Cho KS, Park CK, Kang SG, Park YS, Kim DS, Kim MC (2006) Diagnostic method for differentiating external hydrocephalus from simple subdural hygroma. J Neurosurg 105:65–70
Krieger MD, McComb JG, Levy ML (1999) Toward a simpler surgical management of Chiari I malformation in a pediatric population. Pediatr Neurosurg 30:113–121
Marshman LAG, Benjamin JC, Chawda SJ, David KM (2005) Acute obstructive hydrocephalus associated with infratentorial subdural hygromas complicating Chiari malformation type I decompression. Report of two cases and literature review. J Neurosurg 103:752–755
Menezes AH (1991) Chiari I malformations and hydromyelia—complications. Pediatr Neurosurg 17:146–154
Paré LS, Batzdorf U (1998) Syringomyelia persistence after Chiari decompression as a result of pseudomeningocele formation: implications for syrinx pathogenesis: report of three cases. Neurosurgery 43:945–948
Perrini P, Benedetto N, Tenenbaum R, Di Lorenzo N (2007) Extra-arachnoidal cranio-cervical decompression for syringomyelia associated with Chiari I malformation in adults: technique assessment. Acta Neurochirurgica 149:1015–1023
Ranjan A, Cast IP (1996) Symptomatic subdural hygroma as a complication of foramen magnum decompression for hindbrain herniation (Arnold–Chiari deformity). Br J Neurosurg 10:301–303
Sindou M, Chávez-Machuca J, Hashish H (2002) Cranio-cervical decompression for Chiari type I-malformation, adding extreme lateral foramen magnum opening and expansile duroplasty with arachnoid preservation. Technique and long-term functional results in 44 consecutive adult cases—comparison with literature data. Acta Neurochir (Wien) 144:1005–1019
Williams B (1986) Progress in syringomyelia. Neurol Res 8:130–145
Yoshimoto Y, Wakai S, Hamano M (1998) External hydrocephalus after aneurysm surgery: paradoxical response to ventricular shunting. J Neurosurg 88:485–488
Author information
Authors and Affiliations
Corresponding author
Additional information
Comments
Jörg Klekamp, Quakenbrück, Germany
The authors describe an unusual complication after foramen magnum decompression for Chiari type I malformation. It is well established that Chiari I malformation causes CSF flow obstruction at the foramen magnum which may lead to syringomyelia. However, little is known about the intracranial consequences of this flow obstruction. Surely, there must be alterations of intracranial CSF flow. However, whereas obstructive hydrocephalus is a regular feature of Chiari type II malformation, it appears in only about 10% of patients with Chiari I. In other words, the intracranial CSF flow abnormalities are well compensated in most cases.
With decompression at the foramen magnum, a CSF passage is provided that leads to a decrease of the syrinx in the overwhelming majority of patients. However, flow patterns inside the cranial cavity are changed as well. Most patients suffer from low pressure symptoms for a few days due to the intraoperative loss of CSF. Postoperative scans taken at this stage almost always demonstrate a dilatation of the subarachnoid space in the posterior fossa. But this phenomenon resolves quickly and has never caused any long-term problems in my experience. On the other hand, about 3% develop a postoperative hydrocephalus withour resolution of the syrinx even though the CSF passage at the foramen magnum is patent. This may happen immediately after surgery or weeks later. With placement of a ventricular shunt this problem resolves and the syrinx decreases.
I think that the patient presented here belongs into this category. The only unusual feature is that the raised CSF pressure led to subdural and large soft tissue CSF collections first, before a ventricular dilatation developed. I don´t think that performing a duraplasty would have prevented this complication. At the moment, we can only speculate why this complication may develop. This case report emphasizes that all patients operated for a Chiari type I malformation should be monitored postoperatively for signs of increased intracranial pressure.
Rights and permissions
About this article
Cite this article
Perrini, P., Rawlinson, A., Cowie, R.A. et al. Acute external hydrocephalus complicating craniocervical decompression for syringomyelia–Chiari I complex. Neurosurg Rev 31, 331–335 (2008). https://doi.org/10.1007/s10143-008-0129-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10143-008-0129-5