
Abstract
Patients with systemic lupus erythematosus (SLE) form a vulnerable group in terms of the impact of the COVID-19 pandemic on disease management. We conducted this overview by searches through Medline/PubMed, Scopus, and the Directory of Open Access Journals (DOAJ). The prevalence and severity of COVID-19, efficacy of COVID-19 vaccination, impact on the management of SLE, and the attitudes of SLE patients to COVID-19 and vaccination were explored. After screening and due exclusions, 198 studies were included for the final review. Patients with SLE have a greater risk of acquiring COVID-19 (0.6–22%) and related hospitalization (30%), severe disease (13.5%), and death (6.5%) than the general population. Older age, male gender, comorbidities, moderate or high disease activity, and glucocorticoid, rituximab, and cyclophosphamide use are associated with unfavorable outcomes, whereas methotrexate and belimumab use showed no association with outcomes. COVID-19 vaccines are safe in SLE with minimal risk of severe flares (< 2%). Vaccine efficacy is negatively associated with glucocorticoids. The overall attitude of patients towards vaccination is positive (54–90%). The pandemic has negatively affected access to medical care, hospitalizations, procurement of drugs, employment, and the mental health of patients which need to be addressed as part of holistic care in SLE.
Key Points • Lupus patients are at a greater risk of acquiring COVID-19, related hospitalization, severe disease, and death than the general population. • COVID-19 vaccines are relatively safe for lupus patients with minimal risk of severe flares. • Lupus patients’ attitude towards COVID-19 vaccination is predominantly positive. |
Similar content being viewed by others


Introduction
The coronavirus disease 2019 (COVID-19) pandemic has ravaged the world with over four billion cases and close to six million deaths (as of April 1, 2022) over the last 2 years [1]. The USA is plagued by the highest number of cases to date with the highest mortality in terms of deaths/million followed closely by Brazil and the UK [1]. These numbers represent only the tip of the iceberg with respect to the adverse impact of the pandemic on other aspects of healthcare that have taken a back foot since then.
The characteristics of the novel coronavirus or severe acute respiratory syndrome-coronavirus-2 (SARS-Cov-2) infection include more severe presentation in vulnerable populations with various comorbidities as observed in Wuhan right from the early stages of the pandemic [2]. The concern about infections in patients with autoimmune rheumatic diseases (AIRDs) is understandable and springs from various disease- and treatment-related factors. With the emergence of COVID-19, there was a palpable apprehension among physicians about the risk, severity of infection, and post-infective sequelae secondary to the underlying immune dysregulation as well as the immunosuppressant drugs used for their management. These issues represent the imminent problems posed by the COVID-19 pandemic.
The near paralysis of the non-COVID healthcare delivery system with countrywide lockdowns resulted in lack of access to care and follow-up visits, doubts about the initiation and continuation of immunosuppressive therapy, and, above all, the safety and efficacy of vaccination against COVID-19. The recognition of these issues was promptly dealt with by researchers across the globe, and early reports from the Global Rheumatology Alliance (GRA) described a higher rate of hospitalization (46%) and mortality (9%) than the general population [3]. The scientific community has stood up to the challenge, and numerous studies have been undertaken to answer these questions posed by the pandemic [4, 5]. Constraints on resources and manpower during the pandemic have resulted in studies with flaws in design and methodology with multiple biases. Hence, it is difficult to translate the results of individual studies to the clinic.
Systemic lupus erythematosus (SLE) is a prototype AIRD with a wide range of severity and organ involvement. It requires a delicate evaluation and follow-up with management centered around immunosuppressive therapy. There is an added vulnerability of common comorbidities such as diabetes mellitus and arterial hypertension which are commonly associated with SLE and are risk factors for severe COVID-19 [2]. Furthermore, the drugs used for its management may result in further suppression of immunity with a greater risk of severe COVID disease as well as poor vaccine efficacy, especially in patients on glucocorticoids (GC) and rituximab (RTX) therapies [4, 6, 7]. Therefore, a detailed evaluation of the impact of the COVID-19 pandemic on patients with SLE assumes great importance.
Previous reviews have summarized the severity of COVID-19 in SLE and the influence of immunomodulatory drugs; however, the rapid addition of information warrants newer insights into this area [8,9,10,11]. There are recent studies on the impact of COVID-19 on SLE as well as various aspects of vaccination in patients with SLE. Thus, this narrative review is undertaken to gain an overall perspective of SLE in the time of the ongoing pandemic.
The aim of this narrative review is to explore the impact of the COVID-19 pandemic on SLE in terms of prevalence and severity of infection, efficacy of COVID-19 vaccination, management of SLE, and the patients’ attitudes to the disease and related vaccines.
Search strategy
Searches through Medline/PubMed and Scopus were performed in line with previously published recommendations [12]. Articles published until March 28, 2022, were retrieved and analyzed using the following keywords: (“COVID-19” OR “SARS-CoV-2”) AND (“SLE” OR “lupus”). Of the 360 and 688 articles obtained, respectively, in PubMed/Medline and Scopus, articles in a language other than English were excluded [13] (Fig. 1). Studies including both adults and children were studied, and trials, observational studies, letters, and case reports were included. After an initial screening of titles and abstracts, 198 relevant articles were retained (132 articles and 66 case reports). Those studies reporting general outcomes in rheumatic diseases without detailed data on patients with SLE were excluded. Additionally, information about specific sections was obtained through an individualized search strategy (“COVID-19” AND “lupus” AND “severity,” “COVID-19” AND “lupus” AND “hospitalizations,” “COVID-19” AND “lupus” AND “vaccines”). Relevant articles searchable at the Directory of Open Access Journals (DOAJ) and references of included articles were also processed for eligibility and inclusion for this review.

Methodology of comprehensive and systematic searches through databases and registers
Features of COVID-19 in patients with SLE and effects of drugs
Prevalence
The early reports of features of COVID-19 in SLE from China, Europe, and the USA during the first wave of the pandemic described a similar prevalence of infection as compared to the general population [14] except from France and the USA [15, 16]. The French study was a telephonic survey of presumptive cases where a prevalence of 6.6% (versus 0.11% in the general population) was found [15], whereas the study from New York reported a prevalence of 4% in the Columbia Lupus Cohort (versus 2% in the general population) [16]. Single-center studies from Napoli and Pisa also reported a higher rate of 18–20% in patients with SLE than in other studies; however, the rates in the general population were not reported in parallel [17, 18]. Conclusion on the severity of COVID-19 in SLE patients could not be drawn effectively from these early studies due to small sample sizes and biases involved in the interpretation of hospital-based studies.
Subsequent studies reported a mixed prevalence of 0.6–22% [19,20,21] with variability likely due to the different timings of subsequent waves of the pandemic across different countries, high prevalence of infection in certain regions, and the different methodologies of the surveys conducted (Table 1).
Hospitalization
The rate for hospitalization was variable ranging from 0.8 to 80% across various countries; results from the Global Rheumatology Alliance (GRA) of 1606 patients with SLE reported a rate of 30% [22]. A wide range for hospitalization was observed due to different time points of conduction of the studies and different methodologies with major differences between surveys and hospital-based studies. Studies from very early phases of the pandemic have a low prevalence of 0.8% likely due to countrywide lockdowns. Subsequently hospitalization rates increased which were predominantly due to severe disease, but a small proportion seemed to be due to anxiety of the comorbid status. However, most studies do not clearly mention the reason for hospitalizations and is a subject for further study. Recent studies report a lower rate possibly due to decline in anxiety associated with COVID-19 as well as ramping up of the immunization against it. Furthermore, healthcare policies have been modified with better understanding of the disease process in subsequent waves of the pandemic that may have led to fewer hospitalizations, especially of the asymptomatic and mild cases in the later part of the pandemic.
The risk for hospitalization was three-fold higher than the general population as per a nationwide study in Denmark [23]. There was an increased risk associated with race (odds ratio [OR] 7.78 for non-Whites versus Whites, 95% CI 1.13–53.58), presence of comorbidities (OR 4.66, 95% CI 1.02–21.20), and body mass index (BMI) (1.08 per increase in kg/m2, 95% CI 0.99–1.18) as per results from the New York University (NYU) Lupus Cohort [24]. Rituximab use was associated with the risk of hospitalization (OR 12, 95% CI 5.8–28) [21, 25]. Contrasting associations with belimumab and GC use were observed with regard to the risk of hospitalization [23, 24, 26]. There was no effect of hydroxychloroquine (HCQ) on the risk of COVID-19 and hospitalization across all studies [17, 19, 27].
Severity and outcomes
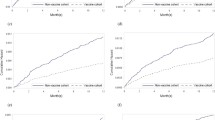
The rates of severe COVID-19 and related deaths were variable across studies owing to the different timeframes of recruitment, study designs, and country-wise prevalence of COVID-19 [17, 19, 27] (Table 1). As per the GRA report [22], severe disease (13.5%) and death (6.5%) were higher in the SLE than the general population and were associated with older age of SLE patients (OR 1.03, 95% CI 1.02–1.04), male gender (OR 1.5, 95% CI 1.01–2.23), no current treatment (OR 1.8, 95% CI 1.17–2.75), comorbidities (kidney disease OR 3.51, 95% CI 2.42–5.09; cardiovascular disease/arterial hypertension OR 1.69, 95% CI 1.25–2.29), and moderate or high SLE disease activity (versus remission; OR 1.61, 95% CI 1.02–2.54 and OR 3.94, 95% CI 2.11–7.34, respectively). A study from Brazil reported twice the frequency of unfavorable outcomes in SLE as compared with the general population without comorbidities, but the risk was similar when compared to the general population with comorbidities (Table 1) (Fig. 2) [28].

Factors associated with severity of COVID-19 in lupus patients. CYC, cyclophosphamide; MMF, mycophenolate mofetil; AZA, azathioprine
Two studies in pediatric SLE reported favorable outcomes, with a prevalence of 2.6% and none requiring hospitalization in the study from the USA [29], whereas the Spanish study reported eight cases with one requiring hospitalization [30].
Influence of immunosuppressants
HCQ was widely prescribed for the prevention of COVID-19 in the early phases of the pandemic based on observational studies, but no influence of HCQ on the prevention was proven subsequently [31]. Likewise, across all observational studies in SLE, no effect of HCQ was observed in the prevention of symptomatic COVID-19 (Table 1). The absence of evidence supporting the positive role of HCQ in COVID-19 as well as the risk of arrhythmias when used in combination with azithromycin resulted in phasing out the over-prescription of HCQ during the pandemic [32,33,34]. Furthermore, no QTc prolongation was observed with the standard doses used in SLE in a study from the Colombia Lupus Cohort [35].
Concerns regarding GC use during the pandemic stem from the pan immunosuppressive effect and increased risk of infections as well as severity observed with them. GC are irreplaceable for the management of SLE, and hence the impact of GC on the risk and severity of COVID-19 infection was of concern. A nationwide cohort study in Denmark [23] and a telephonic survey in Belgium [26] found no impact of GC on the risk of COVID-19 infections [23, 26]. Most other studies have observed an increased association of GC use with the risk of COVID-19 infection, hospitalizations, and unfavorable outcomes even in SLE patients with low disease activity or remission; and use of low dose GC (< 7.5 mg/day) [19, 26, 27, 36]. The initial report from the GRA observed twice the odds for hospitalizations with GC doses above 10 mg/day [3], whereas the latest report observed an increased association of GC with unfavorable outcomes in COVID-19 with GC doses less than 5 mg/day (1–5 mg/day OR 1.86, 95% CI 1.2–2.66; 6–9 mg/day OR 2.47, 95% CI 1.24–4.86; and ≥ 10 mg/day OR 1.95, 95% CI 1.27–2.99) [22]. Furthermore, data from the ReumaCov registry from Brazil showed recent pulse methylprednisolone (MPS) therapy in addition to oral GC had twice the odds for hospitalization and intensive care unit admission, with pulse MPS alone associated with death [36]. Despite the risks associated with GC use, control of disease activity in SLE is of prime importance and is an additional factor for unfavorable COVID-19 outcomes. Hence, most guidelines recommend appropriate GC use without abrupt discontinuation [37].
Patients of SLE with COVID-19 were 2.3 times and 7.7 times more likely to be on azathioprine (AZA) and cyclosporine (CsA), respectively, as per an Italian web-based survey [27]. Mycophenolate mofetil (MMF) (OR 1.2, 95% CI 0.93–1.55) and CYC (OR 1.92, 95% CI 0.95–3.91) use were not associated with unfavorable outcomes across multiple studies including the GRA [22, 27, 36]. Also, no association was found between methotrexate (OR 0.71, 95% CI 0.5–1.01) and unfavorable outcomes of COVID-19 in SLE [22]. Other studies have shown no associations of the risk of infection and severity with conventional immunosuppressants such as AZA, CsA, MTX, MMF, and CYC (Table 1) [26, 38].
Rituximab and belimumab are the most frequent biologics used in SLE [39]. Rituximab directly targets B cells, whereas the latter inhibits soluble B lymphocyte stimulator BLyS and prevents its interaction with its receptors on B cells, decreasing their survival. RTX therapy has been associated with increased hospitalization and unfavorable outcomes with OR 1.62 in the GRA study [22]. A study in Belgium reported a higher risk of hospitalization with belimumab [26]. However, the sample size was small with only two hospital admissions, thus making it difficult to interpret the findings [26]. Other studies reported no effect of belimumab on outcomes of COVID-19 [22, 27].
COVID-19 vaccination in SLE
Vaccine safety
Multiple studies evaluating various COVID-19 vaccines have reported safety of these in adolescent and adult patients with SLE [40,41,42]. An online survey in Denmark explored the safety of BNT162b2 (Pfizer/BioNTech) vaccine and compared it to the original vaccine trial in patients with SLE (n = 182) and rheumatoid arthritis (RA) (n = 103). An increased frequency of local side effects in the form of pain (74% versus 66%) and swelling (26% versus 7%) was reported, and the majority of the effects were mild. Fatigue (69% versus 51%) and headache (52% versus 39%) were the most common systemic side effects. Five of 285 patients (1.8%) reported adverse events requiring emergency hospitalization [43]. Other studies from India [44], Mexico [45], the EU [41, 46, 47], and the USA [48, 49] reported similar results with local pain, headache, and fatigue being the most common adverse effects of different COVID-19 vaccines (Table 2). Severe reactions were noted in 0–1.8% across various studies [43, 44, 51]. The EULAR Coronavirus Vaccine (COVAX) physician-reported registry has examined vaccine-related adverse events in 5121 patients, including 369 with SLE. Vaccine-related adverse events were reported in 37% overall; mRNA-1273 (Moderna) had the highest risk of local adverse events (40%) compared with others (12%) [41]. AZD1222 had the highest risk for systemic adverse events in the form of fever (12%) compared with others (6%) [41]. Arrhythmia, myocarditis, liver injury, arthritis, and rash were observed in SLE as adverse events without major consequences [41].
In a single-center study evaluating the safety of COVID-19 vaccination in pediatric SLE, adverse events were noted in 4 of 16 patients (25%), and none were severe [40]. The adverse events were more frequent with the BNT162b2/Pfizer BioNTech vaccine than CoronaVac inactivated SARS-CoV-2. Post vaccination lupus flares were seen in two patients, and both were mild [40].
Vaccine-induced lupus flares
Vaccines can trigger and flare autoimmunity due to both the viral proteins and adjuvants used in the manufacturing process [50]. Studies from the NYU Lupus Cohort as well as the GRA reported a flare rate of 11% and 13%, respectively, of which 1.3% were severe in the former study and 4.6% required a change of medication in the latter study [42, 48]. The EULAR COVAX registry reported a flare rate of 3% with severe flares being infrequent (< 1%) [41]. Most other studies also reported a similar flare rate and severity irrespective of the vaccine type [42, 46, 48]. These differences are likely due to the higher adverse effects reported by patients in questionnaire-based studies, whereas lower rates were observed with physician-reported events (Table 2). Thus, vaccine-induced lupus flares are infrequent, mild, and only about 5% require a change in medications.
Vaccine-induced SLE
The reports of new-onset SLE following COVID-19 vaccination are summarized in Table 3. These cases were seen irrespective of age and gender bias, with known autoimmune disease or family history of the same being risk factors. Lupus symptoms were seen predominantly with B162b2/PfizerBioNTech (8 of 10) after either of the doses. Most patients were treated with GC along with steroid-sparing drugs, and all patients improved in the short term (Table 3) [51,52,53,54,55,56,57,58,59,60].
COVID-19 vaccine efficacy in SLE
SLE is characterized by immune dysregulation due to the disease itself compounded by the use of immunosuppressants. Most live vaccines are contraindicated in SLE, and inactivated vaccines need to be given before starting immunosuppression [61]. The humoral immune response examined in a prospective observational study from the NYU Lupus Cohort (90 lupus patients and 20 healthy controls [HC]) was found to be lower in SLE than in HC with 28% having anti-receptor binding domain (RBD) antibodies below 100 IU/ml which was the lowest level observed in controls [48]. Positive predictors of anti-RBD antibodies were baseline immunoglobulin levels, B lymphocyte percentage, and young age, whereas negative predictors included the use of MMF, MTX, GC, and RTX [47, 48]. A moderate correlation (R = 0.57, P = 0.0135) was observed between anti-RBD antibodies and cell-mediated response with 57% having T cell responses among those with good neutralizing antibodies compared to only 10% in those without neutralizing antibodies [46, 48]. No association was observed between SLE disease activity, GC, HCQ, belimumab, baseline interferon-alpha levels, and total lymphocyte count with anti-RBD antibodies [46, 48]. Another study in Hong Kong also reported lower neutralizing antibodies in patients with SLE (n = 65) as compared to healthy controls (n = 65) [62]. In the EULAR COVAX registry, breakthrough COVID-19 infections were seen in 0.7% of the fully vaccinated SLE patients [41].
Thus, COVID-19 vaccines appear to be safe in SLE patients with more local reactions with mRNA vaccines. The side effects included mild local pain, fatigue, and headache. The risk of severe lupus flares is minimal. The efficacy of COVID-19 vaccination is lower than in the general population, especially for those on MMF, RTX, GC, and inactivated vaccines.
Surveys of patients’ attitudes to COVID-19 vaccines
Concerns about COVID-19 vaccination in patients with AIRDs stem from the exclusion of these patients from vaccine trials with reservations about potential adverse effects, flares, and interaction with drugs. These are compounded further by misinformation most commonly from social media [63].
In a questionnaire-based study from the SMILE cohort in Italy (n = 317), 76% of patients had a positive attitude towards vaccination, with the remaining having concerns about the potential risk of flare and side effects [27]. Likewise, in a nationwide survey of 908 participants with AIRDs in Brazil, including 188 patients with SLE, the vaccine acceptance rate was 80% with the most frequent reasons for vaccine hesitancy being short vaccine trials followed by concerns of side effects and flares [64]. Those treated with HCQ, belimumab, pulse MPS, and having kidney disease, cancer, and fibromyalgia were more likely to be vaccine hesitant [64].
An early report from the GRA of 900 patients, including 397 patients with SLE, revealed that the majority (80%) discussed this issue with their physicians and received positive feedback from them [42]. About two-thirds of all patients were willing to withhold immunosuppression temporarily during vaccination; the remaining had concerns about plausible lupus flares [42]. In contrast, a study from Egypt exploring rheumatology faculty opinion on this topic found that only 70% of surveyees were willing to recommend COVID-19 vaccination to patients with AIRDs, of which SLE was the disease with the highest priority for vaccination [65]. A survey (VAXICOV study) with respondents predominantly from South America and Europe reported willingness to receive vaccine in 54%, and uncertainty in 30% in patients with AIRDs, including 492 patients with SLE. This figure increased to 62% when the vaccination was recommended by a physician [66]. A similar observation was noted in a Chinese survey where only 30% of patients with SLE showed willingness for vaccination which improved to 90% after recommendation by a physician [67].
Thus, a majority of lupus patients have a positive attitude towards vaccination, especially after receiving physicians’ recommendation. Concerns are mainly due to short-term follow-ups and fear for adverse events and flares.
Impact of the COVID-19 pandemic on patients with SLE
Patients with chronic diseases are prone to more severe COVID-19 and unfavorable outcomes [68]. Psychological stress due to lockdowns and social distancing has resulted in a rise in anxiety and depression among patients with SLE [69]. Irregular supply of medications, difficulty in scheduling hospital appointments, and inaccessibility of medical care have further complicated the issue [69]. Similar themes emerged from a social media–based study providing real-time data on concerns of patients with AIRDs during the pandemic [70].
Thus, the pandemic has posed multiple issues concerning COVID-19, management of SLE, and repercussions on patients’ mental health. Having said that, most lupus patients have a positive attitude towards social distancing, masks, and alcohol-based hand rubs for the prevention of infection [69, 71].
Impact on disease
In a questionnaire-based study from the SMILE Lupus Cohort in Italy, the median overall health reported as per Numerical Rating Scale was 7 (6–8) during 2020, with 30% requiring treatment escalation (62% GC, 51% new immunosuppressant, 7% addition of belimumab) predominantly for joint and skin disease [27]. Thirty-four percent of patients reported adequately controlled disease allowing tapering of GC (68%) and/or immunosuppressants (35%). About two-thirds reported missed appointments secondary to healthcare delivery disruption. Overall, 54% reported no significant effect of the pandemic on their disease, while the remaining reported worsening (17%) and improvement (4%). Twenty-five percent were uncertain about the same [27].
An online survey from the INSPIRE Lupus Cohort in India reported difficulty in procuring medications and scheduling hospital visits due to the lockdown restrictions [72]. Worsening of disease during the pandemic was noted in 25%, and the mean patient global assessment value was 6.69 (1.26) [72]. Interestingly, 61% felt confident of the correct management of disease during the lockdown by being associated with the cohort [72]. Another survey from the Philippines with 405 lupus patients reported similar findings, with two-thirds reporting their health status as good [73]. An irregular supply of HCQ resulted in increased frequency of myalgia and rash [73, 74]. Similar results from Egypt, Poland, Saudi Arabia, and the GRA were observed (Table 4) [75, 76].
When 97 patients with lupus nephritis from Brazil were analyzed, fear for COVID-19 was rated to be 8 of 10, for flare 7 of 10, with > 90% compliance to the use of masks and drugs for SLE, and fear for the use of immunosuppressants was zero [10]. Another study from Egypt also reported a greater likelihood of patients with SLE for drug adherence and social distancing [71]. Hence, the attitude of patients towards COVID-19 and medications also depends on SLE severity. Those on biologics were also more likely to follow social distancing norms as per an American study [77].
From the Padua Lupus Cohort, 3% of patients discontinued medications during the first wave of the COVID-19 pandemic [18]; a study from Pisa reported a discontinuation rate of 11% either by physician recommendation or patient choice with a significant association with flares [19].
In a retrospective study in Malaysia, the frequency of hospitalization of patients with lupus was reduced by 65% but required more intensive treatment due to higher severity of symptoms [78, 79]. Elective admissions for renal biopsies and hemodialysis training in them also reduced significantly [78, 79].
Thus, worsening disease activity was noted in 8–50% of patients with SLE across multiple studies based on patient-reported questionnaires. Up to 75% of patients with lupus encountered difficulties with medical care access, and 70% of them had difficulty procuring drugs (Table 4).
Impact on psychosocial health
A questionnaire-based study of 361 patients with rheumatic diseases, including 125 patients with lupus, revealed overall frequencies of 9% for depression and 7% for anxiety [76, 80,81,82,83]. The rates have been reported to be as high as 40% in studies from France and the Philippines [74, 84]. However, an Italian study concluded that these rates were comparable with the general population [85]. Poor access to medical care rather than the risk of COVID-19 stirred anxiety in a large survey in the UK [69]. Female gender, rural residency, and GC use were all positively associated with anxiety and depression. Anxiety and depression were negatively associated with satisfaction with available health information and wearing of face masks [83].
The way forward
The management of SLE in times of COVID-19 should include appropriate counseling and healthcare delivery to ensure compliance with COVID protective measures, medications, and promote vaccine willingness. The use of telemedicine to monitor lupus activity and disseminate evidence-based information holds prime importance at the time of COVID-19 waves and lockdowns. Additionally, telemedicine can be employed to follow up lupus patients with stable disease to reduce strain on hospitals. In a large American survey of 3000 patients, although drug compliance is better with physical visits, it is still higher with telemedicine than with no visits [77]. It is also an opportunity to reinforce the importance of vaccination and boosters as per the local recommendations [77].
Although the use of GC and immunosuppressants are associated with severe COVID-19, these drugs should not be abruptly stopped as active disease itself is a risk factor for unfavorable COVID-19 outcomes. GC should be used in the lowest possible doses. The preference of belimumab over rituximab for the management of SLE needs to be explored further. Minor organ manifestations can be treated with HCQ, MTX, or AZA, reserving MMF, CYC, and RTX for major organ disease.
Adequate control of arterial hypertension, diabetes mellitus, and other comorbidities is of prime importance. COVID-19 vaccination should be reinforced in patients with SLE as adverse events are few. Breakthrough infections are uncommon and are usually mild. This should be coupled with appropriate COVID protective measures like the use of face masks and social distancing. More studies are warranted to explore the impact of stopping immunosuppressants at the time of vaccination on the overall vaccine efficacy in SLE. Home-based exercise programs along with the dissemination of appropriate health information should be carried out for reducing anxiety and depression [86].
Although there is significant amount of data on the prevalence and severity of COVID-19, there are definite lacunas in various aspects. More active research is needed in the areas of safety and efficacy of vaccination. Recommendations on the use of drugs during COVID-19 vaccination are largely based on older studies of influenza vaccination. Most studies are questionnaire-based; thus, prospective cohort studies and controlled trails are the need of the hour specially to study vaccine effectiveness in SLE. Innovative strategies to manage SLE in the light of COVID-19 need to be devised and assessed objectively.
We acknowledge inherent limitations related to the design of the narrative review with a subjective assessment of the retrieved studies. Most current studies are medical records review or questionnaire-based studies with heterogeneity of results across countries.
In conclusion, patients with SLE seem to have a greater risk of COVID-19 infection and hospitalization than the general population. Older age, male gender, associated comorbidities, GC, CYC, MMF, and RTX use are associated unfavorable outcomes. COVID-19 vaccines are safe and efficacious in SLE with minimal risk for severe flares. The overall attitude of patients towards vaccination is positive, with an influence of physician recommendation on the same. The pandemic has significantly affected access to medical care, hospitalizations, access to drugs, employment, and the mental health of patients which need to be addressed as a part of holistic care in SLE.
References
COVID Live - Coronavirus statistics - Worldometer. https://www.worldometers.info/coronavirus/. Accessed 1 Apr 2022
Huang C, Wang Y, Li X et al (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395:497–506. https://doi.org/10.1016/S0140-6736(20)30183-5
Gianfrancesco M, Hyrich KL, Al-Adely S et al (2020) Characteristics associated with hospitalisation for COVID-19 in people with rheumatic disease: data from the COVID-19 Global Rheumatology Alliance physician-reported registry. Ann Rheum Dis 79:859–866. https://doi.org/10.1136/annrheumdis-2020-217871
Montero F, Martínez-Barrio J, Serrano-Benavente B et al (2020) Coronavirus disease 2019 (COVID-19) in autoimmune and inflammatory conditions: clinical characteristics of poor outcomes. Rheumatol Int 40:1593–1598. https://doi.org/10.1007/s00296-020-04676-4
Doskaliuk B, Yatsyshyn R, Klishch I, Zimba O (2021) COVID-19 from a rheumatology perspective: bibliometric and altmetric analysis. Rheumatol Int 41:2091–2103. https://doi.org/10.1007/s00296-021-04987-0
Lee ARYB, Wong SY, Chai LYA et al (2022) Efficacy of covid-19 vaccines in immunocompromised patients: systematic review and meta-analysis. BMJ 376:e068632. https://doi.org/10.1136/bmj-2021-068632
Manzi S, Meilahn EN, Rairie JE et al (1997) Age-specific incidence rates of myocardial infarction and angina in women with systemic lupus erythematosus: comparison with the Framingham Study. Am J Epidemiol 145:408–415. https://doi.org/10.1093/oxfordjournals.aje.a009122
Thanou A, Sawalha AH (2021) SARS-CoV-2 and systemic lupus erythematosus. Curr Rheumatol Rep 23:8. https://doi.org/10.1007/s11926-020-00973-w
Ceccarelli F, Covelli V, Olivieri G et al (2021) Systemic lupus erythematosus before and after COVID-19 lockdown: how the perception of disease changes through the lenses of narrative medicine. Healthcare (Basel) 9:726. https://doi.org/10.3390/healthcare9060726
Pedrosa T, de Kupa LVK, Aikawa NE et al (2020) Lupus nephritis-related issues during COVID-19 pandemic quarantine. Lupus 29:1978–1980. https://doi.org/10.1177/0961203320957098
Mason A, Anver H, Lwin M et al (2021) Lupus, vaccinations and COVID-19: what we know now. Lupus 30(10):1541–1552. https://doi.org/10.1177/09612033211024355
Gasparyan AY, Ayvazyan L, Blackmore H, Kitas GD (2011) Writing a narrative biomedical review: considerations for authors, peer reviewers, and editors. Rheumatol Int 31:1409. https://doi.org/10.1007/s00296-011-1999-3
Salameh J-P, Bossuyt PM, McGrath TA et al (2020) Preferred reporting items for systematic review and meta-analysis of diagnostic test accuracy studies (PRISMA-DTA): explanation, elaboration, and checklist. BMJ 370:m2632. https://doi.org/10.1136/bmj.m2632
Mathian A, Mahevas M, Rohmer J et al (2020) Clinical course of coronavirus disease 2019 (COVID-19) in a series of 17 patients with systemic lupus erythematosus under long-term treatment with hydroxychloroquine. Ann Rheum Dis 79:837–839. https://doi.org/10.1136/annrheumdis-2020-218795
Gartshteyn Y, Askanase AD, Schmidt NM et al (2020) COVID-19 and systemic lupus erythematosus: a case series. Lancet Rheumatol 2:e452–e454. https://doi.org/10.1016/S2665-9913(20)30161-2
Holubar J, Le Quintrec M, Letaief H et al (2021) Monitoring of patients with systemic lupus erythematosus during the COVID-19 outbreak. Ann Rheum Dis 80:e56. https://doi.org/10.1136/annrheumdis-2020-217919
Fasano S, Ciccia F (2020) Incidence of COVID-19 in an Italian cohort of patients with systemic lupus erythematosus: an observational survey. Clin Exp Rheumatol 128:13
Zen M, Fuzzi E, Astorri D et al (2020) SARS-CoV-2 infection in patients with autoimmune rheumatic diseases in northeast Italy: a cross-sectional study on 916 patients. J Autoimmun 112:102502. https://doi.org/10.1016/j.jaut.2020.102502
Zucchi D, Tani C, Elefante E et al (2021) Impact of first wave of SARS-CoV-2 infection in patients with systemic lupus erythematosus: weighting the risk of infection and flare. PLoS ONE 16:e0245274. https://doi.org/10.1371/journal.pone.0245274
Hidayat R, Isbagio H, Ariane A, et al. (2020) Characteristics of patients with autoimmune rheumatic disease in the era of COVID-19 pandemic in Indonesia. Indones J Rheumatol 12. https://doi.org/10.37275/ijr.v12i1.159
Boekel L, Hooijberg F, Vogelzang EH et al (2022) Antibody development and disease severity of COVID-19 in non-immunised patients with rheumatic immune-mediated inflammatory diseases: data from a prospective cohort study. RMD Open 8:e002035. https://doi.org/10.1136/rmdopen-2021-002035
Ugarte-Gil MF, Alarcon GS, Izadi Z, et al. (2022) Characteristics associated with poor COVID-19 outcomes in individuals with systemic lupus erythematosus: data from the COVID-19 Global Rheumatology Alliance. Ann Rheum Dis Published Online First: 16 https://doi.org/10.1136/annrheumdis-2021-221636
Cordtz R, Kristensen S, Dalgaard LPH et al (2021) Incidence of COVID-19 hospitalisation in patients with systemic lupus erythematosus: a nationwide cohort study from Denmark. J Clin Med 10:3842. https://doi.org/10.3390/jcm10173842
Fernandez-Gutierrez B, Leon L, Madrid A et al (2021) Hospital admissions in inflammatory rheumatic diseases during the peak of COVID-19 pandemic: incidence and role of disease-modifying agents. Ther Adv Musculoskelet Dis 13:1759720X20962692. https://doi.org/10.1177/1759720X20962692
Bachiller-Corral J, Boteanu A, Garcia-Villanueva MJ et al (2021) Risk of severe COVID-19 infection in patients with inflammatory rheumatic diseases. J Rheumatol 48:1098–1102. https://doi.org/10.3899/jrheum.200755
Gendebien Z, von Frenckell C, Ribbens C et al (2020) Systematic analysis of COVID-19 infection and symptoms in a systemic lupus erythematosus population: correlation with disease characteristics, hydroxychloroquine use and immunosuppressive treatments. Ann Rheum Dis 80:e94. https://doi.org/10.1136/annrheumdis-2020-218244
Ramirez GA, Argolini LM, Bellocchi C et al (2021) Impact of the COVID-19 pandemic in patients with systemic lupus erythematosus throughout one year. Clin Immunol 231:108845. https://doi.org/10.1016/j.clim.2021.108845
Bertoglio IM, de Valim LJM, Daffre D et al (2021) Poor prognosis of COVID-19 acute respiratory distress syndrome in lupus erythematosus: nationwide cross-sectional population study of 252 119 patients. ACR Open Rheumatol 3:804–811. https://doi.org/10.1002/acr2.11329
Walters HM, Mian Z, Thomas L, et al. (2021) Seroprevalence and clinical outcomes of SARS-CoV-2 in paediatric patients with rheumatic disease. Rheumatology (Oxford) keab730. https://doi.org/10.1093/rheumatology/keab730
Clemente D, Udaondo C, de Inocencio J et al (2021) Clinical characteristics and COVID-19 outcomes in a regional cohort of pediatric patients with rheumatic diseases. Pediatr Rheumatol Online J 19:162. https://doi.org/10.1186/s12969-021-00648-5
Das RR, Jaiswal N, Dev N et al (2020) Efficacy and safety of anti-malarial drugs (chloroquine and hydroxy-chloroquine) in treatment of COVID-19 infection: a systematic review and meta-analysis. Front Med(Lausanne) 7:482. https://doi.org/10.3389/fmed.2020.00482
Mercuro NJ, Yen CF, Shim DJ et al (2020) Risk of QT interval prolongation associated with use of hydroxychloroquine with or without concomitant azithromycin among hospitalized patients testing positive for coronavirus disease 2019 (COVID-19). JAMA Cardiol 5:1036–1041. https://doi.org/10.1001/jamacardio.2020.1834
O’Connell TF, Bradley CJ, Abbas AE et al (2021) Hydroxychloroquine/azithromycin therapy and QT prolongation in hospitalized patients with COVID-19. JACC Clin Electrophysiol 7:16–25. https://doi.org/10.1016/j.jacep.2020.07.016
Saleh M, Gabriels J, Chang D et al (2020) Effect of chloroquine, hydroxychloroquine, and azithromycin on the corrected QT interval in patients with SARS-CoV-2 infection. Circ Arrhythm Electrophysiol 13:e008662. https://doi.org/10.1161/CIRCEP.120.008662
Park E, Giles JT, Perez-Recio T et al (2021) Hydroxychloroquine use is not associated with QTc length in a large cohort of SLE and RA patients. Arthritis Res Ther 23:1–12. https://doi.org/10.1186/s13075-021-02646-0
Marques CDL, Kakehasi AM, Pinheiro MM et al (2021) High levels of immunosuppression are related to unfavourable outcomes in hospitalised patients with rheumatic diseases and COVID-19: first results of ReumaCoV Brasil registry. RMD Open 7:e001461. https://doi.org/10.1136/rmdopen-2020-001461
Mikuls TR, Johnson SR, Fraenkel L et al (2021) American College of Rheumatology Guidance for the management of rheumatic disease in adult patients during the COVID-19 pandemic: Version 3. Arthritis Rheumatol 73:e1–e12. https://doi.org/10.1002/art.41596
Favalli EG, Gerosa M, Murgo A, Caporali R (2020) Are patients with systemic lupus erythematosus at increased risk for COVID-19? Ann Rheum Dis 80:e25. https://doi.org/10.1136/annrheumdis-2020-217787
Murphy G, Isenberg DA (2020) Biologic therapies for systemic lupus erythematosus: where are we now? Curr Opin Rheumatol 32:597–608. https://doi.org/10.1097/BOR.0000000000000736
Haslak F, Gunalp A, Cebi MN et al (2022) Early experience of COVID-19 vaccine-related adverse events among adolescents and young adults with rheumatic diseases: a single-center study. Int J Rheum Dis 25:353–363. https://doi.org/10.1111/1756-185X.14279
Machado PM, Lawson-Tovey S, Strangfeld A et al (2022) Safety of vaccination against SARS-CoV-2 in people with rheumatic and musculoskeletal diseases: results from the EULAR Coronavirus Vaccine (COVAX) physician-reported registry. Ann Rheum Dis 81:695–709. https://doi.org/10.1136/annrheumdis-2021-221490
Sattui SE, Liew JW, Kennedy K et al (2021) Early experience of COVID-19 vaccination in adults with systemic rheumatic diseases: results from the COVID-19 Global Rheumatology Alliance Vaccine Survey. RMD Open 7:e001814. https://doi.org/10.1136/rmdopen-2021-001814
Bartels LE, Ammitzboll C, Andersen JB et al (2021) Local and systemic reactogenicity of COVID-19 vaccine BNT162b2 in patients with systemic lupus erythematosus and rheumatoid arthritis. Rheumatol Int 41(11):1925–1931. https://doi.org/10.1007/s00296-021-04972-7
Cherian S, Paul A, Ahmed S et al (2021) Safety of the ChAdOx1 nCoV-19 and the BBV152 vaccines in 724 patients with rheumatic diseases: a post-vaccination cross-sectional survey. Rheumatol Int 41:1441–1445. https://doi.org/10.1007/s00296-021-04917-0
Esquivel-Valerio JA, Skinner-Taylor CM, Moreno-Arquieta IA et al (2021) Adverse events of six COVID-19 vaccines in patients with autoimmune rheumatic diseases: a cross-sectional study. Rheumatol Int 41:2105–2108. https://doi.org/10.1007/s00296-021-05017-9
Moyon Q, Sterlin D, Miyara M et al (2022) BNT162b2 vaccine-induced humoral and cellular responses against SARS-CoV-2 variants in systemic lupus erythematosus. Ann Rheum Dis 81:575–583. https://doi.org/10.1136/annrheumdis-2021-221097
Ferri C, Ursini F, Gragnani L et al (2021) Impaired immunogenicity to COVID-19 vaccines in autoimmune systemic diseases. High prevalence of non-response in different patients’ subgroups. J Autoimmun 125:102744. https://doi.org/10.1016/j.jaut.2021.102744
Izmirly PM, Kim MY, Samanovic M et al (2021) Evaluation of immune response and disease status in systemic lupus erythematosus patients following SARS-CoV-2 vaccination. Arthritis Rheumatol 74:284–294. https://doi.org/10.1002/art.41937
Connolly CM, Ruddy JA, Boyarsky BJ et al (2021) Safety of the first dose of mRNA SARS-CoV-2 vaccines in patients with rheumatic and musculoskeletal diseases. Ann Rheum Dis 80:1100–1101. https://doi.org/10.1136/annrheumdis-2021-220231
van der Laan JW, Gould S, Tanir JY (2015) Safety of vaccine adjuvants: focus on autoimmunity. Vaccine 33:1507–1514. https://doi.org/10.1016/j.vaccine.2015.01.073
Kaur I, Zafar S, Capitle E, Khianey R (2022) COVID-19 vaccination as a potential trigger for new-onset systemic lupus erythematosus. Cureus 14(2):e21917. https://doi.org/10.7759/cureus.21917
Raviv Y, Betesh-Abay B, Valdman-Grinshpoun Y, et al. (2022) First presentation of systemic lupus erythematosus in a 24-year-old male following mRNA COVID-19 vaccine. Case Rep Rheumatol 22.https://doi.org/10.1155/2022/9698138
Hidaka D, Ogasawara R, Sugimura S et al (2021) New-onset Evans syndrome associated with systemic lupus erythematosus after BNT162b2 mRNA COVID-19 vaccination. Int J Hematol 23:1–4. https://doi.org/10.1007/s12185-021-03243-2
Baez-Negron L, Vila LM (2022) New-onset systemic lupus erythematosus after mRNA SARS-CoV-2 vaccination. Case Rep Rheumatol 022:6436839. https://doi.org/10.1155/2022/6436839
Zavala-Miranda MF, Gonzalez-Ibarra SG, Perez-Arias AA et al (2021) New-onset systemic lupus erythematosus beginning as class V lupus nephritis after COVID-19 vaccination. Kidney Int 100:1340–1341. https://doi.org/10.1016/j.kint.2021.09.009
Zengarini C, Pileri A, Salamone FP et al (2022) Subacute cutaneous lupus erythematosus induction after SARS-CoV-2 vaccine in a patient with primary biliary cholangitis. J Eur Acad Dermatol Venereol 36:e179–e180. https://doi.org/10.1111/jdv.17827
Am N, Saleh AM, Khalid A et al (2022) Systemic lupus erythematosus with acute pancreatitis and vasculitic rash following COVID-19 vaccine: a case report and literature review. Clin Rheumatol 17:1–6. https://doi.org/10.1007/s10067-022-06097-z
Molina-Rios S, Rojas-Martinez R, Estévez-Ramirez GM, Medina YF (2022) Systemic lupus erythematosus and antiphospholipid syndrome after COVID-19 vaccination. A case report. Mod Rheumatol Case Rep rxac018. https://doi.org/10.1093/mrcr/rxac018
Nune A, Iyengar KP, Ish P et al (2021) The emergence of new-onset SLE following SARS-CoV-2 vaccination. QJM Int J Med 114:739–740. https://doi.org/10.1093/qjmed/hcab229
Patil S, Patil A (2021) Systemic lupus erythematosus after COVID-19 vaccination: a case report. J Cosmet Dermatol 20:3103–3104. https://doi.org/10.1111/jocd.14386
Furer V, Rondaan C, Heijstek MW et al (2020) 2019 update of EULAR recommendations for vaccination in adult patients with autoimmune inflammatory rheumatic diseases. Ann Rheum Dis 79:39–52. https://doi.org/10.1136/annrheumdis-2019-215882
So H, Li T, Chan V et al (2022) Immunogenicity and safety of inactivated and mRNA COVID-19 vaccines in patients with systemic lupus erythematosus. Ther Adv Musculoskelet Dis 14:1759720X221089586. https://doi.org/10.1177/1759720X221089586
Gupta L, Gasparyan AY, Misra DP et al (2020) Information and misinformation on COVID-19: a cross-sectional survey study. J Korean Med Sci 35:e256. https://doi.org/10.3346/jkms.2020.35.e256
Vieira Rezende RP, Braz AS, Guimarães MFB et al (2021) Characteristics associated with COVID-19 vaccine hesitancy: a nationwide survey of 1000 patients with immune-mediated inflammatory diseases. Vaccine 39:6454–6459. https://doi.org/10.1016/j.vaccine.2021.09.057
Hammam N, Tharwat S, Shereef RRE et al (2021) Rheumatology university faculty opinion on coronavirus disease-19 (COVID-19) vaccines: the vaXurvey study from Egypt. Rheumatol Int 41:1607–1616. https://doi.org/10.1007/s00296-021-04941-0
Felten R, Kawka L, Dubois M et al (2021) Tolerance of COVID-19 vaccination in patients with systemic lupus erythematosus: the international VACOLUP study. Lancet Rheumatol 3(9):e613–e615. https://doi.org/10.1016/S2665-9913(21)00221-6
Chen J, Cai W, Liu T, et al. (2022) The COVID-19 vaccine: attitudes and vaccination in patients with autoimmune inflammatory rheumatic diseases. RheumatolAutoimmun 1-10.https://doi.org/10.1002/rai2.12028
CDC (2022) People with certain medical conditions. In: Cent. Dis. Control Prev. https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html. Accessed 28 Apr 2022
Sloan M, Gordon C, Lever E et al (2021) COVID-19 and shielding: experiences of UK patients with lupus and related diseases. Rheumatol Adv Pract 5:rkab003. https://doi.org/10.1093/rap/rkab003
Reuter K, Deodhar A, Makri S et al (2021) The impact of the COVID-19 pandemic on people with rheumatic and musculoskeletal diseases: insights from patient-generated data on social media. Rheumatology(Oxford) 60:SI77–SI84. https://doi.org/10.1093/rheumatology/keab174
Tharwat S, Mohamed SZ, Nassar MK (2021) Challenges of Egyptian patients with systemic lupus erythematosus during the COVID-19 pandemic. Reumatologia 59:237–243. https://doi.org/10.5114/reum.2021.108620
Rathi M, Singh P, Bi HP et al (2020) Impact of the COVID-19 pandemic on patients with systemic lupus erythematosus: observations from an Indian inception cohort. Lupus 30:158–164. https://doi.org/10.1177/0961203320962855
Salido EO, Tee CA, Reyes PWC et al (2021) Self-reported symptoms in a cohort of rheumatoid arthritis and systemic lupus erythematosus during the COVID-19 quarantine period. Open Rheumatol J 15:16–23. https://doi.org/10.2174/1874312902115010016
Tee CA, Salido EO, Reyes PWC et al (2020) Psychological state and associated factors during the 2019 coronavirus disease (COVID-19) pandemic among Filipinos with rheumatoid arthritis or systemic lupus erythematosus. Open Access Rheumatol 12:215–222. https://doi.org/10.2147/OARRR.S269889
Wańkowicz P, Szylińska A, Rotter I (2020) Evaluation of mental health factors among people with systemic lupus erythematosus during the SARS-CoV-2 pandemic. J Clin Med 9:2872. https://doi.org/10.3390/jcm9092872
Hassen LM, Almaghlouth IA, Hassen IM et al (2020) Impact of COVID-19 outbreak on rheumatic patients’ perceptions and behaviors: a cross-sectional study. Int J Rheum Dis 23:1541–1549. https://doi.org/10.1111/1756-185X.13959
George MD, Baker JF, Banerjee S et al (2021) Social distancing, health care disruptions, telemedicine use, and treatment interruption during the COVID-19 pandemic in patients with or without autoimmune rheumatic disease. ACR Open Rheumatol 3(6):381–389. https://doi.org/10.1002/acr2.11239
Chuah SL, Teh CL, Wan Mohd Akbar SA, et al. (2020) Impact of COVID-19 pandemic on hospitalisation of patients with systemic lupus erythematosus (SLE): report from a tertiary hospital during the peak of the pandemic. Ann Rheum Dis.https://doi.org/10.1136/annrheumdis-2020-218475
Lee WWH, Cheong YK, Teh CL et al (2021) Impact of COVID-19 on hospitalization of patients with systemic lupus erythematosus (SLE). Clin Rheumatol 40:4775–4777. https://doi.org/10.1007/s10067-021-05920-3
Lim SL, Tay VY, Bhullar A et al (2021) A questionnaire-based survey on depression and anxiety among rheumatology patients during the COVID-19 pandemic: patient’s perspective. Oman Med J 36:e305. https://doi.org/10.5001/omj.2022.34
Kasturi S, Price LL, Paushkin V et al (2021) Impact of the first wave of the COVID-19 pandemic on systemic lupus erythematosus patients: results from a multi-center prospective cohort. Lupus 30:1747–1755. https://doi.org/10.1177/09612033211033981
Gonzalez-Rangel J, Perez-Munoz B, Casillas-Santos D et al (2021) Mental health in patients with rheumatic diseases related to COVID-19 pandemic: experience in a tertiary care center in Latin America. Lupus 30:1879–1887. https://doi.org/10.1177/09612033211038052
Borisova AB, Lisitsyna TA, Veltishchev DY, Nasonov EL (2021) Anxiety, depression and stress tension screening in patients with rheumatic and musculoskeletal diseases at the onset of the 2019 coronavirus disease (COVID-19) pandemic. Hayчнo-Пpaктичecкaя Peвмaтoлoгия 59:676–683. https://doi.org/10.47360/1995-4484-2021-676-683
Scherlinger M, Zein N, Gottenberg J-E et al (2022) Difficulties and psychological impact of the SARS-CoV-2 pandemic in patients with systemic lupus erythematosus: a nationwide patient association study. Healthcare (Basel) 10:330. https://doi.org/10.3390/healthcare10020330
Quartuccio L, De Marchi G, Azzolina D et al (2021) Psychological effects of lockdown measures for the COVID-19 outbreak in patients with systemic lupus erythematosus. J Multidiscip Healthc 14:1475–1488. https://doi.org/10.2147/JMDH.S311325
Maheswaranathan M, English JA, Cunningham MA, Kamen DL (2021) Development and implementation of a virtual lupus patient education event during the COVID-19 pandemic. Lupus Sci Med 8:e000493. https://doi.org/10.1136/lupus-2021-000493
Ramirez GA, Gerosa M, Beretta L et al (2020) COVID-19 in systemic lupus erythematosus: data from a survey on 417 patients. Semin Arthritis Rheum 50(5):1150–1157. https://doi.org/10.1016/j.semarthrit.2020.06.012
Pablos JL, Abasolo L, Alvaro-Gracia JM et al (2020) Prevalence of hospital PCR-confirmed COVID-19 cases in patients with chronic inflammatory and autoimmune rheumatic diseases. Ann Rheum Dis 79:1170–1173. https://doi.org/10.1136/annrheumdis-2020-217763
Mageau A, Papo T, Ruckly S et al (2021) Survival after COVID-19-associated organ failure among inpatients with systemic lupus erythematosus in France: a nationwide study. Ann Rheum Dis 81:569–574. https://doi.org/10.1136/annrheumdis-2021-221599
Espinosa G, Prieto-Gonzalez S, Llevadot M et al (2021) The impact of SARS-CoV-2 coronavirus infection in patients with systemic lupus erythematosus from a single center in Catalonia. Clin Rheumatol 40:2057–2063. https://doi.org/10.1007/s10067-021-05675-x
Attauabi M, Seidelin JB, Felding OK et al (2021) Coronavirus disease 2019, immune-mediated inflammatory diseases and immunosuppressive therapies - a Danish population-based cohort study. J Autoimmun 118:102613. https://doi.org/10.1016/j.jaut.2021.102613
Shobha V, Chanakya K, Haridas V et al (2021) Do all patients with rheumatic diseases have a higher risk of COVID 19? Initial results from the Karnataka Rheumatology Association COVID 19 Cohort Study (KRACC). Indian J Rheumatol 16(16):164–168. https://doi.org/10.4103/injr.injr_261_20
Saadoun D, Vieira M, Vautier M et al (2021) SARS-CoV-2 outbreak in immune-mediated inflammatory diseases: the Euro-COVIMID multicentre cross-sectional study. Lancet Rheumatol 3:e481–e488. https://doi.org/10.1016/S2665-9913(21)00112-0
Schioppo T, Argolini LM, Sciascia S, et al. (2021) Clinical and peculiar immunological manifestations of SARS-CoV-2 infection in systemic lupus erythematosus patients. Rheumatology (Oxford) keab611. https://doi.org/10.1093/rheumatology/keab611
Assar S, Mohamadzadeh D, Pournazari M, Soufivand P (2022) Frequency, characteristics and outcome of corona virus disease 2019 (COVID-19) infection in Iranian patients with rheumatic diseases. Egypt Rheumatol 44:209–213. https://doi.org/10.1016/j.ejr.2021.12.002
Zavala-Flores E, Salcedo-Matienzo J, Quiroz-Alva A, Berrocal-Kasay A (2021) Effects of the COVID-19 quarantine on patients with rheumatoid arthritis and systemic lupus erythematosus. Rev Peru Med Exp Salud Publica 37:783–784. https://doi.org/10.17843/rpmesp.2020.374.6150
Liew J, Gianfrancesco M, Harrison C et al (2022) SARS-CoV-2 breakthrough infections among vaccinated individuals with rheumatic disease: results from the COVID-19 Global Rheumatology Alliance provider registry. RMD Open 8:e002187. https://doi.org/10.1136/rmdopen-2021-002187
Boyarsky BJ, Ruddy JA, Connolly CM et al (2021) Antibody response to a single dose of SARS-CoV-2 mRNA vaccine in patients with rheumatic and musculoskeletal diseases. Ann Rheum Dis 80:1098–1099. https://doi.org/10.1136/annrheumdis-2021-220289
Hausmann JS, Kennedy K, Simard JF, et al. (2021) Immediate effect of the COVID-19 pandemic on patient health, health-care use, and behaviours: results from an international survey of people with rheumatic diseases. Lancet Rheumatol.https://doi.org/10.1016/S2665-9913(21)00175-2
Plantinga LC, Hoge C, Dunlop-Thomas C, et al. (2022) Association of COVID-19 pandemic-related concern and health routine changes with functioning among individuals with systemic lupus erythematosus. Lupus Sci Med.https://doi.org/10.1136/lupus-2022-000658
Ammitzboll C, Bartels LE, Bogh Andersen J, et al. (2021) Impaired antibody response to the BNT162b2 Messenger RNA coronavirus disease 2019 vaccine in patients with systemic lupus erythematosus and rheumatoid arthritis. ACR Open Rheumatol.https://doi.org/10.1002/acr2.11299
Garrido-Cumbrera M, Marzo-Ortega H, Christen L et al (2021) Assessment of impact of the COVID-19 pandemic from the perspective of patients with rheumatic and musculoskeletal diseases in Europe: results from the REUMAVID study (phase 1). RMD Open 7:e001546. https://doi.org/10.1136/rmdopen-2020-001546
Author information
Authors and Affiliations
Contributions
Conceptualization: Gasparyan AY and Zimba O. Methodology: Gasparyan AY and Kitas GD. Writing—original draft: Pankti M and Gasparyan AY. Writing—review and editing: Pankti M, Gasparyan AY, Zimba O, and Kitas GD. All the authors have approved the final manuscript and take full responsibility for the integrity of the contents of the final manuscript.
Corresponding author
Ethics declarations
Disclosures
None.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Mehta, P., Gasparyan, A.Y., Zimba, O. et al. Systemic lupus erythematosus in the light of the COVID-19 pandemic: infection, vaccination, and impact on disease management. Clin Rheumatol 41, 2893–2910 (2022). https://doi.org/10.1007/s10067-022-06227-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-022-06227-7