
Abstract
Background
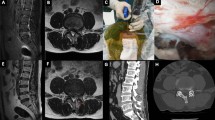
Although percutaneous endoscopic lumbar discectomy (PELD) has been popularized as an alternative to microscopic lumbar discectomy, it has been reported to be associated with a re-herniation rate of 5–11%. Recurrent lumbar disc herniation (RLDH) might occur not only at the same level previously operated upon but also at the annular penetration site created during PELD procedures.
Method
Biportal endoscopic paraspinal approach (BE-Para) was used for revisional foraminal lumbar discectomy. Procedures and some discussions regarding indications, advantages, potential complications, and ways to avoid complications were described.
Conclusion
BE-Para may be an effective modality for RLDH after PELD.


Similar content being viewed by others

Data and/or code availability
Not applicable.
References
Ayturk UM, Garcia JJ, Puttlitz CM (2010) The micromechanical role of the annulus fibrosus components under physiological loading of the lumbar spine. J Biomech Eng 132:061007
Carragee EJ, Han MY, Suen PW, Kim D (2003) Clinical outcomes after lumbar discectomy for sciatica: the effects of fragment type and anular competence. JBJS 85:102–108
Dave BR, Degulmadi D, Krishnan A, Mayi S (2020) Risk factors and surgical treatment for recurrent lumbar disc prolapse: a review of the literature. Asian Spine J 14:113
Heo DH, Sharma S, Park CK (2019) Endoscopic treatment of extraforaminal entrapment of L5 nerve root (far out syndrome) by unilateral biportal endoscopic approach: technical report and preliminary clinical results. Neurospine 16:130
Krames ES (2014) The role of the dorsal root ganglion in the development of neuropathic pain. Pain Med 15:1669–1685
Lee JH, Choi K-C, Lee JH (2019) Could the splitting of the annulus during percutaneous endoscopic lumbar diskectomy (PELD) be a culprit for recurrent disk herniation?: an analysis of the reherniation pattern after PELD. World Neurosurg 132:e623–e629
Li Z-Z, Cao Z, Zhao H-L, Shang W-l, Hou S-X (2020) A pilot study of full-endoscopic annulus fibrosus suture following lumbar discectomy: technique notes and one-year follow-up. Pain Physician 5:E497–E505
Pan M, Li Q, Li S, Mao H, Meng B, Zhou F, Yang H (2020) Percutaneous endoscopic lumbar discectomy: indications and complications. Pain Physician 23:49–56
Shepard N, Cho W (2019) Recurrent lumbar disc herniation: a review. Global Spine J 9:202–209
Shiri R, Euro U, Heliövaara M, Hirvensalo M, Husgafvel-Pursiainen K, Karppinen J, Lahti J, Rahkonen O, Raitakari OT, Solovieva S (2017) Lifestyle risk factors increase the risk of hospitalization for sciatica: findings of four prospective cohort studies. Am J Med 130(1408–1414):e1406
Acknowledgements
The authors appreciate the Editage (www.editage.co.kr) for English language editing.
Author information
Authors and Affiliations
Contributions
SCP, JHY, WJJ, and MSK contributed to the conception of the study. SCP and MSK wrote the manuscript. JHY and WJJ reviewed the manuscript. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
This study protocol was approved by the Institutional Review Board (IRB file no.: BMH 2022–03-024) and adhered to the guidelines of the Declaration of Helsinki.
Consent to participate
Not applicable.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Key points
I. BE-Para is a minimally invasive alternative to conventional microscopic technique that provides some advantages such as tissue sparing and minimal blood loss.
II. The annular defect created by cannular penetration during PELD might be a route for RLDH.
III. Despite some concerns regarding the revision surgery, BE-Para is a viable option for the revisional foraminal lumbar discectomy.
IV. Two independent 0.8-cm-sized vertical incisions should be made at 2 cm lateral to the lateral margin of the pedicle over the midportion of the transverse processes of adjacent vertebrae.
V. When dissecting and removing the facet joint capsule from the isthmus, attention should be paid to prevent severe bleeding because the articular branch of lumbar radicular artery passes inside the joint capsule.
VI. The portion where the exiting root originates from the dural sac should be secured before adhesiolysis to avoid root injury, because the fibrotic scar tissue is usually not seen at this site.
VII. Blunt dissection starts from the origin of the root and should advance peripherally using a dissector.
VIII. When working around the exiting nerve root, care should be taken to avoid damaging dorsal root ganglion, which is sensitive to the neuropathic pain.
IX. Lifestyle modifications, such as regular walking, blood sugar control, cessation of smoking, and weight reduction, are as necessary as meticulous surgical techniques.
X. BE-Para discectomy, a non-fusion technique, for the recurrent disc herniation, might have the risk of re-recurrent disc herniation requiring a third surgery.
This article is part of the Topical Collection on Spine Degenerative
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 (MP4 101483 KB)
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Park, S.C., Kang, MS., Yang, J.H. et al. How I do it: biportal endoscopic paraspinal approach for recurrent lumbar disc herniation following percutaneous endoscopic lumbar discectomy. Acta Neurochir 164, 3057–3060 (2022). https://doi.org/10.1007/s00701-022-05368-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-022-05368-7