
Abstract
Background
The mortality rate of patients with brain oedema after malignant middle cerebral artery (MCA) infarction approaches 80 % without surgical intervention. Surgical treatment with ipsilateral decompressive hemicraniectomy (DHC) has been shown to dramatically improve survival rates. DHC currently lacks established inclusion criteria and additional research is needed to assess the impact of prognostic factors on functional outcome. The aim of this study was to assess the impact of prognostic factors on functional outcome.
Method
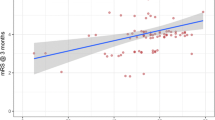
A retrospective cohort study was carried out including 46 patients who underwent DHC at the Karolinska University Hospital between 2004 and 2014. The maximum time to surgery was 5 days after symptom debut. The primary endpoint was a dichotomised score on the modified Rankin Scale (mRS) 3 months after surgery, with favourable outcome defined as mRS ≤ 4.
Results
When the study population was dichotomised according to the primary endpoint, a significant difference between the groups was seen in preoperative Glasgow Coma Score (GCS), blood glucose levels and the infarction’s involvement of the basal ganglia (p < 0.05). In a logistic regression model, preoperative GCS contributed significantly with a 59.6 % increase in the probability of favourable outcome for each point gained in preoperative GCS (p = 0.035).
Conclusions
The results indicate that preoperative GCS, blood glucose and the infarction’s involvement of the basal ganglia are strong predictors of clinical outcome. These factors should be considered when assessing the probable outcome of DHC, and additional research based on these factors may contribute to improved inclusion criteria for DHC.


Similar content being viewed by others

References
Berrouschot J, Sterker M, Bettin S, Köster J, Schneider D (1998) Mortality of space-occupying (‘malignant’) middle cerebral artery infarction under conservative intensive care. Intensive Care Med 24(6):620–623
Chen C-C, Cho D-Y, Tsai S-C (2007) Outcome of and prognostic factors for decompressive hemicraniectomy in malignant middle cerebral artery infarction. J Clin Neurosci 14(4):317–321
Flechsenhar J, Woitzik J, Zweckberger K, Amiri H, Hacke W, Jüttler E (2013) Hemicraniectomy in the management of space-occupying ischemic stroke. J Clin Neurosci 20(1):6–12
Gupta R, Connolly ES, Mayer S, Elkind MSV (2004) Hemicraniectomy for massive middle cerebral artery territory infarction: a systematic review. Stroke 35(2):539–543
Hacke W, Schwab S, Horn M, Spranger M, De Georgia M, von Kummer R (1996) “Malignant” middle cerebral artery territory infarction: clinical course and prognostic signs. Arch Neurol 53(4):309–315
Hofmeijer J, Kappelle LJ, Algra A, Amelink GJ, van Gijn J, van der Worp HB (2009) Surgical decompression for space-occupying cerebral infarction (the Hemicraniectomy After Middle Cerebral Artery infarction with Life-threatening Edema Trial [HAMLET]): a multicentre, open, randomised trial. Lancet Neurol 8(4):326–333
Holtkamp M, Buchheim K, Unterberg A, Hoffmann O, Schielke E, Weber JR, Masuhr F (2001) Hemicraniectomy in elderly patients with space occupying media infarction: improved survival but poor functional outcome. J Neurol Neurosurg Psychiatry 70(2):226–228
Jüttler E, Bösel J, Amiri H, Schiller P, Limprecht R, Hacke W, Unterberg A (2011) DESTINY II: DEcompressive Surgery for the Treatment of malignant INfarction of the middle cerebral arterY II. Int J Stroke 6(1):79–86
Jüttler E, Schellinger PD, Aschoff A, Zweckberger K, Unterberg A, Hacke W (2007) Clinical review: therapy for refractory intracranial hypertension in ischaemic stroke. Crit Care 11(5):231
Jüttler E, Schwab S, Schmiedek P, Unterberg A, Hennerici M, Woitzik J, Witte S, Jenetzky E, Hacke W (2007) Decompressive Surgery for the Treatment of Malignant Infarction of the Middle Cerebral Artery (DESTINY): a randomized, controlled trial. Stroke 38(9):2518–2525
Jüttler E, Unterberg A, Woitzik J, Bösel J, Amiri H, Sakowitz OW, Gondan M, Schiller P, Limprecht R, Luntz S, Schneider H, Pinzer T, Hobohm C, Meixensberger J, Hacke W (2014) Hemicraniectomy in older patients with extensive middle-cerebral-artery stroke. N Engl J Med 370(12):1091–1100
Kagansky N, Levy S, Knobler H (2001) The role of hyperglycemia in acute stroke. Arch Neurol 58(8):1209–1212
Kasner SE, Demchuk AM, Berrouschot J, Schmutzhard E, Harms L, Verro P, Chalela JA, Abbur R, McGrade H, Christou I, Krieger DW (2001) Predictors of fatal brain edema in massive hemispheric ischemic stroke. Stroke 32(9):2117–2123
Knecht S (2000) Handedness and hemispheric language dominance in healthy humans. Brain 123(12):2512–2518
Luitse MJA, Biessels GJ, Rutten GEHM, Kappelle LJ (2012) Diabetes, hyperglycaemia, and acute ischaemic stroke. Lancet Neurol 11(3):261–271
Merenda A, Perez-Barcena J, Frontera G, Benveniste RJ (2015) Predictors of clinical failure of decompressive hemicraniectomy for malignant hemispheric infarction. J Neurol Sci 355(1-2):54–58
Quinn TM, Taylor JJ, Magarik JA, Vought E, Kindy MS, Ellegala DB (2011) Decompressive craniectomy: technical note. Acta Neurol Scand 123(4):239–244
Rahme R, Zuccarello M, Kleindorfer D, Adeoye OM, Ringer AJ (2012) Decompressive hemicraniectomy for malignant middle cerebral artery territory infarction: is life worth living? J Neurosurg 117(4):749–754
Rangel-Castilla L, Rangel-Castillo L, Gopinath S, Robertson CS (2008) Management of intracranial hypertension. Neurol Clin 26(2):521–541
Socialstyrelsen (2009) Hjärninfarkt med expansiv effekt (malign mediainfarkt) hos patienter under cirka 60 år. Nationella riktlinjer för strokesjukvård 2009—Stöd för styrning och ledning.The National Board of Health and Welfare, Stockholm
Vahedi K, Hofmeijer J, Juettler E, Vicaut E, George B, Algra A, Amelink GJ, Schmiedeck P, Schwab S, Rothwell PM, Bousser M-G, van der Worp HB, Hacke W (2007) Early decompressive surgery in malignant infarction of the middle cerebral artery: a pooled analysis of three randomised controlled trials. Lancet Neurol 6(3):215–222
Vahedi K, Vicaut E, Mateo J, Kurtz A, Orabi M, Guichard J-PP, Boutron C, Couvreur G, Rouanet F, Touzé E, Guillon B, Carpentier A, Yelnik A, George B, Payen D, Bousser M-GG (2007) Sequential-design, multicenter, randomized, controlled trial of early decompressive craniectomy in malignant middle cerebral artery infarction (DECIMAL Trial). Stroke 38(9):2506–2517
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
Karolinska Institutet provided financial support in the form of funding for the Department of Neurosurgery. The sponsor had no role in the design or conduct of this research.
Conflicts of interest
None.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required. The study was approved by the Ethical Review Board in Stockholm, Sweden.
Additional information
Comment
This is a quality manuscript and worthy of our consideration. It is gratifying to see that such good information can be mined from a retrospective study design, and I commend the authors for their rigorous and scientific approach to the subject.
There is useful information in this report that impacts our clinical decision making, specifically, that in cases of malignant MCA infarction, surgery is worthwhile, and that favorable surgical outcome can be predicted by three preoperative factors—a higher GCS score, lower blood glucose, and lack of basal ganglia involvement. Equally important to us is that other factors which we traditionally hold sacred don’t seem to impact outcome, like left/right infarct laterality, size of bone flap, age, sex, or time to surgery.
For our own practice in the USA we customarily let the patient’s family make the final decision. We have no hesitation to perform DHC for MCA infarcts, and we do it routinely. When we do it we try our best to do it early, before a falling GCS sets in, and before frank cerebral herniation has occurred.
We believe in this treatment as a strategy for patient salvage and we believe that this report extends our knowledge base regarding patient selection and the path to a successful outcome. The alternative in malignant MCA infarct, absent surgery, is customarily death, which we seek to avoid when we can.
Christopher M. Loftus
Illinois, USA
Rights and permissions
About this article

Cite this article
von Olnhausen, O., Thorén, M., von Vogelsang, AC. et al. Predictive factors for decompressive hemicraniectomy in malignant middle cerebral artery infarction. Acta Neurochir 158, 865–873 (2016). https://doi.org/10.1007/s00701-016-2749-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-016-2749-9