
Abstract
Introduction
Acute stress, the psychological response to short-term challenging stimuli, is frequently encountered in the high-pressure environment of the operating theatre. Surgeon stress is associated with deterioration in surgical performance, surgical team working and compromised patient safety. Given these concerns, the aim of this review was to understand the impact of acute stress on surgical performance in technical and non-technical domains as well as patient outcomes.
Methods
A systematic review was conducted following PRISMA guidelines. Electronic databases were searched for studies examining acute stress in medical professionals during real or simulated surgical procedures that reported performance outcomes in technical and non-technical skills. Risk of bias assessment was conducted using appropriate tools for each study design.
Results
Out of 1445 identified studies, 19 met the inclusion criteria. In simulated environments, acute stress consistently led to impairment in both technical and non-technical skills during surgical procedures. Technical skill deterioration included higher procedural error rates, longer task completion times and diminished instrument handling. Non-technical skills, such as teamwork and communication, also were impaired under stress conditions. Real-world studies echoed these findings, demonstrating acute stress resulting in higher error rates and impaired non-technical skills. No studies identified surgeon stress as having a causal relationship with patient outcomes.
Conclusion
Acute stress significantly impacts both technical and non-technical skills during surgical procedures, impairing performance in simulated and real-world surgical environments. Despite the growing understanding of the detrimental effects of stress, gaps remain in comprehensively assessing its impact on patient outcomes. Further research is warranted to develop reliable stress measurement methods applicable in surgical settings and explore effective stress management strategies.
Similar content being viewed by others


Explore related subjects
Discover the latest articles and news from researchers in related subjects, suggested using machine learning.Avoid common mistakes on your manuscript.
The operating theatre is a high-pressure environment, where time-critical decision making and immediate consequence can induce surgeon stress. The American Psychological Association defines stress as “the physiological or psychological response to internal or external stressors” [1]. Stress can also be thought of as a condition that results in a state of arousal, in preparation for a response or adaption [2]. From a physiological perspective, the perception of a stressor involves a vast array of neuronal networks [3, 4]. There differences in the parthway utilised for processing between physical and psychological stimuli, with physical stressors being processed largely in the hypothalamic and brainstem regions and the latter having greater involvement of higher cortical regions [3].
Stress can also be defined using different classifiers such as the source, timing or psychological experience of the stressor. Psychological stress can be experienced from acute (unexpected intraoperative haemorrhage) or chronic events (general life stressors and burnout). Within health research, acute stress is generally defined as short-term exposure to external stressors, whilst internal stressors are typically associated with chronic stress [5]. There is some suggestion that the response to the external stressor may be modulated by the internal environment [5, 6]. In reality, both sources co-exist, jointly contributing to the psychophysiological response [5, 6].
Acute stress can result from multiple sources within the complex environment of the operating theatre. Arora et al. demonstrated high levels of surgeon stress from several factors that could compromise patient safety: patient problems, technical problems as well as equipment and team-work issues [7]. Attempts have been made to clarify the relationship between these factors, such as the Surgical Stress Effects Framework [8]. This model identifies how individual and team characteristics, influenced by organisational and environmental conditions, dynamically interact with job demands and resources. These summate in a stress response affecting both individual and team performance. This performance impacts patient outcome with various factors posing immediate or latent safety threats, errors and adverse events [8]. It is therefore clear that there is a complex relationship between stress and surgical performance.
There are also longer-term effects with exposure to acute stress, with evidence suggesting prolonged exposure contributing to the development of mental health disorders [9]. This may partially explain the high prevalence of mental health disorders in healthcare workers, with 10–20% of doctors experiencing depression during their career and suicide being a disproportionate cause of death amongst doctors relative to the general population [10]. Stress is also an important factor in workforce sustainability with high prevalence of burnout amongst surgeons contributing to work place shortages [11]. Surgeons appear to understand the negative effects of stress, although less insightful views of stress as a “sign of failure” that should be “tolerated” have also been identified [12]. Despite perceptions of resilience, surgeons are not exempt from the consequences of stress and the interaction between acute and chronic stressors within the operating environment is still poorly understood.
Alongside the mental health of the surgeon, there is also evidence to suggest that acute stress has a negative impact surgical performance and thus patient outcomes [13]. Superior technical skills have been shown to have a direct impact on both short-term and long-term patient outcomes [14, 15]. This has been demonstrated in technical domains such as procedural error as well as non-technical domain skills such as communication and teamwork [8, 13, 14]. The effect of stress is not only limited to the operating surgeon themselves, with emotional “contagion” transferring stressed emotional states to other surgical team members [8, 12]. Patients are also affected by the resultant deterioration in non-technical skills, with a third of communication errors resulting in errors endangering patient safety [16]. These negative effects can also occur in the chronic setting. In a systematic review, surgeons reporting burnout were shown to have a 2.5-fold increased risk of making medical errors [11].
Although chronic stress is important, the acute stress that is experienced during a surgical procedure is a prime target for the utilisation of training and technology within the operating theatre. Advances in simulation technology, including virtual and augmented reality, are increasingly being utilised to assess surgeons responses to stress in a safe environment. Although previous reviews on surgical stress have, by and large, not specifically looked at performance in the context of understanding stress within surgery [13, 14, 17, 18]. Furthermore, none of these reviews attempted to define the effect of stress on patient outcomes. Thus, the primary objective of the current article is an up to date review on the effects of acute psychological stress on both technical and non-technical surgical skills in both simulated environments and in real-world surgery. The secondary objective aims to define the literature on how stress in operating surgeons relates to patient outcomes.
Methods
A systematic review was performed in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) [19]. The review was pre-registered prior to searching (CRD42024529018). An electronic search of databases including PsycINFO, Ovid MEDLINE, EMBASE, Cochrane Database was performed on 19/03/2024. Screening was performed by two reviewers independently and a separate adjudicator was available in the event of inter-rater differences. Cognitive load and anxiety, common synonyms of stress, were also used as search terms given the variable definitions of stress used in the literature. Acute stress was defined in this review as a short-term direct or indirect exposure to a stressor. The search strategy is detailed in Appendix 1. The search was repeated prior to submission for publication (02/06/2024) to ensure no recent publications were omitted.
Inclusion criteria are summarised in Table 1. Studies without defined comparators were included if stress was demonstrated during the exposure period. Comparators could also include situations where surgeons were not under stress or a recognized lower stress situation (e.g., assistant vs primary operator, low vs high risk procedure or elective vs emergency surgery). However studies that compared stress between two methods of surgery (for example robotic versus laparoscopic surgery) were excluded as a causality between stress and outcome cannot be ascertained. Measurements of stress could include subjective measures such as questionnaires and objective measures such as validated physiological measurements (for example heart rate variability). Retrospective measurement of stress was included if the exposure to stress was in the peri-procedural period.
The main outcome was surgical performance in either technical or non-technical domains during the procedure. Technical domains include but were not limited to outcomes such as dexterity, procedural length and blood loss as well as validated scoring systems such as the Observed Structured Assessment of Technical Skills (OSATS). Non-technical domains include but were not limited to outcomes such as verbal communication, situational awareness or other forms of validated non-technical skills testing. Studies that did not contain a measure of surgeon performance or did not measure this at the time of the procedure were excluded.
After screening, the following data were extracted: Publication details, study data, participant data, data related to acute stress exposure; including timing, nature of stress and the validated or non-validated measurement tools used to measure either physiological or psychological reaction to stress and the use of self-report or objective metrics; outcomes in technical and non-technical domains as well as patient outcomes. Results were synthesised qualitatively through descriptive and thematic analysis covering technical, non-technical skills and patient outcome.
Risk of bias was assessed using the Newcastle–Ottawa Scale for observational studies, the ROBINS-I score for non-randomised experimental studies and the Rob2 score for randomised controlled trials [20,21,22].
Results
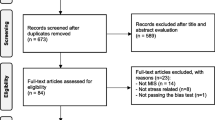
In total, 1445 studies were identified and screened by two separate reviewers (see Fig. 1) with substantial inter-rater agreement (Cohens κ = 0.75, SE = 0.09, CI 0.58–0.92). A total of 19 articles fulfilled the inclusion criteria, consisting of ten non-randomised, prospective experimental studies, five randomised controlled trials and four prospective observational trials. Study summaries are shown in Table 2. Twelve studies involved direct exposure to a stressful stimulus (Five simulated patient-related crises, three additional cognitive loading, one exposure to different music, one exposure to different ambient temperature, one exposure to visual stimuli, one simulated procedure on a live animal). Only four studies were crossover trials [23,24,25,26]. Risk of bias was low to moderate for most studies, with six studies rated low risk, twelve studies medium risk and one high risk of bias.

PRISMA flow diagram of included studies
The effect of acute stress during surgical procedures in simulated environments
Fifteen studies were identified in simulated environments (Table 3).
Technical skills
In a simulated environment, ten prospective experimental studies and five randomized trials were identified with low to medium risk of bias. All studies demonstrated deterioration of technical skills in response to acute stress. Six studies demonstrated the negative impact of stressors on operator kinematics [24, 26,27,28,29,30]. Increased instrument path length, velocity, acceleration and jerk as well as deterioration in usage metrics such as economy of motion, economy of volume and smoothness were also demonstrated during stressed conditions [24, 28, 29]. Deterioration in scores for tissue handling, instrument handling as well as higher procedural error rates were demonstrated in six studies [26, 29, 31,32,33,34]. Zheng et al. demonstrated a linear relationship between instrument velocity, acceleration, jerk as well as path length and increasing levels of stress, with a corresponding reduction of economy of motion under increasing stress [28]. Moorthy et al. reported an increase in time to diagnose and control unexpected bleeding in novices who reported higher stress scores [34].
Stress was demonstrated to increase the time taken to perform the procedures as well as a general decline in operative performance [24, 27, 29, 35]. Despite the heterogeneity of the simulated procedures involved, from peg transfer to more realistic femoral vein exposure, all studies described a decrease in global technical skills, more rapid and less economical movements in response to stress. Four studies compared non-stress performance against simulated patient crises, although only two of these validated the stress event with subjective or objective markers of stress [28, 33, 34, 36]. Both realistic and non-realistic stressors resulted in similar impairments of performance, suggesting that these laboratory-based findings could have real-world implications. However, the confidence of these findings is weakened given the heterogeneity in study design and mixed use of comparative and non-comparative stress exposure.
Three studies did not demonstrate deteriorations in performance. Bahksh et al. did not demonstrate any global difference in technical performance in simulated carotid endarterectomy, although increased sympathetic tone (a physiological maker of stress) was associated with poorer technical performance [36]. The two other studies that did not demonstrate a negative effect of stress used external sensory manipulations which the authors acknowledged was likely insufficiently stressful enough to provoke a response [23, 25]. Chung et al. did not demonstrate any significant difference in performance during exposure to three different auditory stimuli and Berg et al. did not demonstrate any difference in technical performance between groups exposed to two different ambient temperatures although they did note increased physical demand and distraction [23, 25].
Non-technical skills
Two randomised trials of low risk of bias and a single prospective experimental study of moderate risk of bias demonstrated non-technical skill stress effects [32, 34, 35]. In a comparison between a mental practice and conventional practice group, a statistically significant decrease in teamwork scores (OSATS) was demonstrated in a group with higher stress reported during a simulated carotid endarterectomy [35]. In a simulated bleeding crisis, Moorthy et al. did not demonstrate any overall difference in human factors skills although noted a higher number of communications to the surgical team from the expert group who reported lower stress [34]. Louridas et al. compared non-technical skills in jejunostomy formation with a simulated mid-procedural crisis, however, no deterioration in non-technical skills was demonstrated [32]. However the authors acknowledged that the stress-inducing scenario may have not been adequate and relatively insensitive metrics (averaged heart rate and blood pressure) were used to measure stress [32]. The overall lack of significant findings may be a result of the large array of tools used to measure non-technical skills alongside large heterogeneity of study design.
The effect of acute stress during real-world surgical procedures
Four prospective observational studies were performed in real-world operating theatres. All studies did not have a comparative measure between stress and non-stressed states but demonstrated higher levels of stress affecting performance (Table 4).
Technical skills
A single prospective observational study of high risk of bias demonstrated the effect of stress on technical skills. The study of 23 bariatric procedures, demonstrated a statistically significant higher error rate using the Generic Error Rating Tool in stressed time periods, compared to baseline heart rate variability in 1-, 2- and 5-min time periods [37]. The study only involved a single surgeon resulting in the high degree of bias and thus limits the generalisability of these findings.
Non-technical skills
Three prospective observational studies of moderate risk of bias demonstrated a deterioration of non-technical skills in response to acute stress. Anton et al. demonstrated higher stress and workload resulting in lower non-technical skills amongst 15 surgeons [38]. Overall, stress was associated with impaired situational awareness, decision making and the consideration, selection and communication of surgical options, irrespective of experience [38]. In a general surgical environment, two experienced surgeons demonstrating lower stress (measured using physiological variables) were found to have higher task engagement [39]. Sexton et al. demonstrated significantly higher anticipation ratio, higher non-verbal requests and longer request durations in three surgeons performing robotic prostatectomies when reporting stress [40]. These findings are again limited by the large heterogeneity in the methods used to assess non-technical skills utilising both validated and non-validated criteria.
Effect of acute stress on surgeons with patient outcomes
No studies were identified demonstrating that surgeon stress may have a causal relationship on patient outcome. Multiple studies were encountered during screening that compared outcomes for laparoscopic versus robotic surgery, however, none fulfilled the inclusion criteria as they did not directly examine a causal relationship between stress and performance.
Discussion
From the available literature it can be seen that acute stress within the peri-operative period has a direct impact on surgical performance. In both simulated and live surgical environments, there is a negative effect of acute stress on both technical and non-technical skills.
Technical skill impairment from stress was well described in the included studies. Surgeon kinematics appear to have clear linear relationships with acute stress [28]. Increased procedural time under stress, despite more rapid movements is explained by increased path lengths, reduction in economy and higher error rates. The adage of “slow is smooth and smooth is fast” certainly holds true when stress is high. Questions of the underlying mechanism of this movement inefficiency is yet to be understood. Whether this is due to direct effects of stress on visuomotor skills, cognitive processes or a combination of both is unclear. Further research could explore the degree to which the increase in movement inefficiency is caused by changes in movement planning or control.
Non-technical skills were also affected by acute stress. As non-technical skills require additional cognitive resources it is unsurprising that in the presence of stressors, performance in this domain deteriorates. Although Anton et al. demonstrated a general association with stress and non-technical skills regardless of experience, the literature suggests that experience may have a protective effect [8, 13]. This may be explained by the reduction of cognitive load by caching of skills and procedural automaticity gained from experience, resulting in reduced overall workload thus freeing up cognitive resources to maintain performance [13, 41]. Three studies investigated the use of mental practice with relation to performance under stress conditions [31, 32, 42]. Louridas et al. did not demonstrate any difference in non-technical performance with mental practice although did observe improvement in technical skills [32]. Two other studies reported improvements in mental practice groups, suggesting that stress reduction via mental practice improves performance which collaborates with findings from qualitative studies [12]. Given the evidence for the significant impact of non-technical skills on surgical performance, it is surprising that only a minority of studies examined this domain [8].
Several factors were found to moderate the effect of acute stress on performance. Crewther et al. demonstrated that practice resulted in reduction in stress and subsequent improvement of performance [43]. Stress coping strategies also appear to moderate the effect of stress on technical performance [31, 33]. This finding supports those found in qualitative literature and supports a linear relationship between stress and performance deterioration [12]. Further to deterioration of physical technical skills, cognitive load from stress may result in attempts to compensate for reduced cognitive resources, with cognitive lock-up, use of heuristics and simplification of decision making strategies used to compensate but thus resulting in further performance deterioration [8].
No studies were identified demonstrating the effect of acute stress on patient outcomes. Given that qualitative evidence suggests that acute stress has significant effects on surgeon performance this was somewhat surprising. Anton et al. demonstrated 40% of surgeon respondents directly linked surgeon stress with an adverse patient outcome [44]. This would collaborate with the findings of a recent systematic review on burnout in surgeons which demonstrated a heightened risk of medical adverse events in clinicians reporting burnout [11]. It is also well recognised that there is a positive relationship between technical skill and patient outcome [15]. It is therefore concerning that despite previous reviews noting the outcomes of stress on surgical performance and the correlation between performance and patient outcomes not much has changed in over a decade [13]. Although establishing a causal effect of acute stress directly impacting on patient outcomes is challenging given the multitude of factors involved, there is clearly a need for such enquiry.
This review has several limitations. Given the lack of clarity in terminology and the difficulty in defining stress, it is understandable that the literature is highly heterogeneous. A mixed population of healthcare professionals were included due to the sparsity of the literature amongst surgeons alone. The reporting of stress in both subjective and objective physiological measurements was also highly varied. Outcome measurements for both technical and non-technical skills were also highly variable although most utilised objective quantitative measurements. Only 11 of the 19 studies provided a specific exposure to stressful stimuli with the remainder measuring stress during surgical cases. Thus, a causal effect is challenging to ascertain, especially when associating errors to stress or vice versa. In interpreting the results, it is therefore crucial to acknowledge the significant heterogeneity across multiple domains, serving as the key limitation of this review.
Overall, these findings corroborate the qualitative evidence looking at the effects of acute stress on surgeons [12]. With eleven of the included papers published within the last decade, there has been an increased focus on the effect of stress on surgical performance but there are still many unanswered questions.
One key question is how stress and performance can be reliably and objectively quantified, using methods applicable to real-world operating theatres, to allow measurement of acute stress within the operating environment. Psychophysiological metrics, including electroencephalography, eye-tracking, heart rate variability and surgeon kinematics, may be the key real-time objective measurement of stress [18]. This may also address a key limitation when addressing causality between stress and outcome; allowing determination of the presence of stress prior an adverse event such as intra-operative bleeding or as a result of the event. Thus, validated objective measurements would not only improve the understanding of stress within surgery but other high-pressure environments as well.
Using validated objective measures to derive where the threshold between appropriate and excessive levels of stress for optimal performance would not only benefit surgical procedures and patients but also have beneficial effects in the training of surgeons and surgical teams. This review did not specifically examine the effect of stress in training scenarios. Several studies did however demonstrate benefit from strategies to manage and reduce the impact of stress [32, 42]. This finding highlights the utility of applying stress to training in a safe simulated environments; a practice that is frequent in many other fields such as aviation and industry. Given the varying responses noted between experts and novices, there may also be a role for the operators response to stress to act as a marker for surgical skill and expertise [8, 12].
Utilising objective measurement would also allow research into the impact of the multiple factors contributing to stress within this environment. It is clear from the literature that a multi-modal approach is a more sensitive to multiple factors [45]. However, implementation is not without challenge, given that previous methods such as the Imperial Stress Assessment Tool have not been widely utilised [45]. Improved objective quantitative measurement may also allow validation and refinements to currently utilised stress mitigation techniques; mental practice shown to not only improve performance but also retain skills without interim practice, these are yet to be widely utilised [31, 32, 42]
Given the growing recognition of the effects of mental health conditions, an even larger question is the relationship between acute and chronic stress as well as its effect on surgical performance. This is challenging area to investigate given the multitude of factors that give rise to chronic stress and the very individual response to both internal and external stressors. The growing adoption of biometric devices such as smart watches and rings within the population may hold the key to understanding this relationship given their ability for longer-term non-invasive monitoring.
In summary, acute stress has a direct effect on both technical and non-technical skills of surgeons in both simulated and real-world environments. Further research is required to understand how to reliably measure stress in the real-world operating theatre and mitigation strategies to prevent stress reducing surgical performance.
References
VendenBos G (2007) APA Dictionary of Psychology. In: VandenBos G (ed) American Psychological Association
Selye H (1950) Stress and the general adaptation syndrome. Br Med J 1:1383–1392
Godoy LD, Rossignoli MT, Delfino-Pereira P, Garcia-Cairasco N, Umeoka EHL (2018) A comprehensive overview on stress neurobiology: basic concepts and clinical implications. Front Behav Neurosci 12:1–23
Skoluda N, Strahler J, Schlotz W, Niederberger L, Marques S, Fischer S et al (2015) Intra-individual psychological and physiological responses to acute laboratory stressors of different intensity. Psychoneuroendocrinology 51:227–236
Crosswell AD, Lockwood KG (2020) Best practices for stress measurement: how to measure psychological stress in health research. Heal Psychol Open. https://doi.org/10.1177/2055102920933072
Schneiderman N, Ironson G, Siegel SD (2005) Stress and health: psychological, behavioral, and biological determinants. Annu Rev Clin Psychol 1:607–628
Arora S, Hull L, Sevdalis N, Tierney T, Nestel D, Woloshynowych M et al (2010) Factors compromising safety in surgery: stressful events in the operating room. Am J Surg 199(1):60–65
Chrouser KL, Xu J, Hallbeck S, Weinger MB, Partin MR (2018) The influence of stress responses on surgical performance and outcomes: literature review and the development of the surgical stress effects (SSE) framework. Am J Surg 216(3):573–584
McEwen BS (2008) Central effects of stress hormones in health and disease: understanding the protective and damaging effects of stress and stress mediators. Eur J Pharmacol 583(2–3):174–185
Gerada C, Jones R (2014) Surgeons and mental illness: a hidden problem? BMJ. https://doi.org/10.1136/bmj.g2764
Al-Ghunaim T, Johnson J, Biyani CS, Yiasemidou M, O’Connor DB (2023) Burnout and patient safety perceptions among surgeons in the United Kingdom during the early phases of the coronavirus disease 2019 pandemic: a two-wave survey. Scott Med J 68(2):41–48
Arora S, Sevdalis N, Nestel D, Tierney T, Woloshynowych M, Kneebone R (2009) Managing intraoperative stress: what do surgeons want from a crisis training program? Am J Surg 197(4):537–543
Arora S, Sevdalis N, Nestel D, Woloshynowych M, Darzi A, Kneebone R (2010) The impact of stress on surgical performance: a systematic review of the literature. Surgery 147(3):318-330.e6
Fecso AB, Szasz P, Kerezov G, Grantcharov TP (2017) The effect of technical performance on patient outcomes in surgery. Ann Surg 265(3):492–501
Birkmeyer JD, Finks JF, O’Reilly A, Oerline M, Carlin AM, Nunn AR et al (2013) Surgical skill and complication rates after bariatric surgery. N Engl J Med 369(15):1434–1442
Lingard L, Espin S, Whyte S, Regehr G, Baker GR, Reznick R et al (2004) Communication failures in the operating room: an observational classification of recurrent types and effects. Qual Saf Heal Care 13(5):330–334
Budden A, Song S, Henry A, Wakefield CE, Abbott J (2023) A systematic review of biological changes in surgeons’ acute stress levels during surgery. Surg Pract Sci 13:100174
Torkamani-Azar M, Lee A, Bednarik R (2022) Methods and measures for mental stress assessment in surgery: a systematic review of 20 years of literature. IEEE J Biomed Heal Informatics 26(9):4436–4449
Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD et al (2021) PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ 372:n160
Wells G, Shea B, Robertson J, Peterson J, Welch V, Losos M (2012) The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta- Analysis Bias and Confounding Newcastle-Ottowa Scale. Ottawa Hosp Res Inst [Internet]
Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I et al (2019) RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 366:1–8
Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M et al (2016) ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 355:4–10
Berg RJ, Inaba K, Sullivan M, Okoye O, Siboni S, Minneti M et al (2015) The impact of heat stress on operative performance and cognitive function during simulated laparoscopic operative tasks. Surgery 157(1):87–95
Poolton JM, Wilson MR, Malhotra N, Ngo K, Masters RSW (2011) A comparison of evaluation, time pressure, and multitasking as stressors of psychomotor operative performance. Surgery 149(6):776–782
Chung B, Shen J, Yang P, Keheila M, Abourbih S, Khater N, Hogue P, Wong A, Erskine A, Kutzner A, Ritchie C, Cheriyan S, Pierce M, Ruckle H, Baldwin DD (2016) Comparison of three different auditory environments and their effect upon training in novice robotic surgeons. J Endourol 30:A66
Moorthy K, Munz Y, Dosis A, Bann S, Darzi A (2003) The effect of stress-inducing conditions on the performance of a laparoscopic task. Surg Endosc Other Interv Tech 17(9):1481–1484
Keenlyside A, Rae B, Brennan PM, Hughes MA (2023) Emotional visual stimuli and simulated laparoscopic surgical performance: a pilot cohort study. Surgeon 21(6):e352–e360. https://doi.org/10.1016/j.surge.2023.06.004
Zheng Y, Leonard G, Tellez J, Zeh H, Fey AM (2021) Identifying kinematic markers associated with intraoperative stress during surgical training tasks. 2021 Int Symp Med Robot ISMR 2021, pp 1–7
Arora S, Aggarwal R, Moran A, Sirimanna P, Crochet P, Darzi A et al (2011) Mental practice: effective stress management training for novice surgeons. J Am Coll Surg 212(2):225–233
Schuetz M, Gockel I, Beardi J, Hakman P, Dunschede F, Moenk S et al (2008) Three different types of surgeon-specific stress reactions identified by laparoscopic simulation in a virtual scenario. Surg Endosc Other Interv Tech 22(5):1263–1267
Hassan I, Weyers P, Maschuw K, Dick B, Gerdes B, Rothmund M et al (2006) Negative stress-coping strategies among novices in surgery correlate with poor virtual laparoscopic performance. Br J Surg 93(12):1554–1559
Louridas M, Bonrath EM, Sinclair DA, Dedy NJ, Grantcharov TP (2015) Randomized clinical trial to evaluate mental practice in enhancing advanced laparoscopic surgical performance. Br J Surg 102(1):37–44
Wetzel CM, Black SA, Hanna GB, Athanasiou T, Kneebone RL, Nestel D et al (2010) The effects of stress and coping on surgical performance during simulations. Ann Surg 251(1):171–176
Moorthy K, Munz Y, Forrest D, Pandey V, Undre S, Vincent C et al (2006) Surgical crisis management skills training and assessment: a stimulation-based approach to enhancing operating room performance. Ann Surg 244(1):139–147
Wetzel CM, George A, Hanna GB, Athanasiou T, Black SA, Kneebone RL et al (2011) Stress management training for surgeons-a randomized, controlled, intervention study. Ann Surg 253(3):488–494
Bakhsh A, Martin GFJ, Bicknell CD, Pettengell C, Riga C (2019) An evaluation of the impact of high-fidelity endovascular simulation on surgeon stress and technical performance. J Surg Educ 76(3):864–871
Grantcharov PD, Boillat T, Elkabany S, Wac K, Rivas H (2019) Acute mental stress and surgical performance. BJS Open 3(1):119–125
Anton NE, Athanasiadis DI, Karipidis T, Keen AY, Karim A, Cha J et al (2021) Surgeon stress negatively affects their non-technical skills in the operating room. Am J Surg 222(6):1154–1157
van Houwelingen BCG, Rutkowski AF, Ganni S, Stepaniak PS, Jakimowicz JJ (2020) Effects of surgical flow disruptions on surgeons’ resources: a pilot study. Surg Endosc 34(10):4525–4535
Sexton K, Johnson A, Gotsch A, Hussein AA, Cavuoto L, Guru KA (2018) Anticipation, teamwork and cognitive load: chasing efficiency during robot-assisted surgery. BMJ Qual Saf 27(2):148–154
Haith AM, Krakauer JW (2018) The multiple effects of practice: skill, habit and reduced cognitive load. Curr Opin Behav Sci 20:196–201
Stefanidis D, Anton NE, Howley LD, Bean E, Yurco A, Pimentel ME et al (2017) Effectiveness of a comprehensive mental skills curriculum in enhancing surgical performance: results of a randomized controlled trial. Am J Surg 213(2):318–324
Crewther BT, Shetty K, Jarchi D, Selvadurai S, Cook CJ, Leff DR et al (2016) Skill acquisition and stress adaptations following laparoscopic surgery training and detraining in novice surgeons. Surg Endosc 30(7):2961–2968
Anton NE, Montero PN, Howley LD, Brown C, Stefanidis D (2015) What stress coping strategies are surgeons relying upon during surgery? Am J Surg 210(5):846–851
Arora S, Tierney T, Sevdalis N, Aggarwal R, Nestel D, Woloshynowych M et al (2010) The imperial stress assessment tool (ISAT): a feasible, reliable and valid approach to measuring stress in the operating room. World J Surg 34(8):1756–1763
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Mr Adam Tam, Mr Samuel Bateman, Prof. Gavin Buckingham, Prof. Mark Wilson, Prof. G.J. Melendez-Torres, Prof. Sam Vine and Dr James Clark have no conflict of interest in relation to this manuscript. Prof G.J. Melendez-Torres is a National Institute for Health and Care Research (NIHR) Senior Investigator. The views expressed in this article are those of the authors and not necessarily those of the NIHR, or the Department of Health and Social Care.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tam, A., Bateman, S., Buckingham, G. et al. The effects of stress on surgical performance: a systematic review. Surg Endosc 39, 77–98 (2025). https://doi.org/10.1007/s00464-024-11389-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-024-11389-3
Keywords
Profiles
- Samuel Bateman View author profile