
Abstract
Purpose
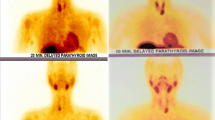
Adenoma is the main parathyroid disorder leading to primary hyperparathyroidism (PHP). Minimally invasive parathyroidectomy (MIP) is recognized as a valid procedure for adenoma-related PHP. It requires precise preoperative localization combining Tc-99m-MIBI (methoxy-isobutyl-isonitrile) scintigraphy and single-photon emission computed tomography (SPECT) with x-ray computed tomography (CT) and intraoperative confirmation of successful excision by change in intact parathormone (iPTH) levels. The study aim was to assess the surgery success in relation to these two parameters.
Methods
All patients operated on for PHP from 2005 to mid-2014 at our institution were retrospectively reviewed. MIP was performed in case of precise preoperative adenoma localization on scintigraphy, absence of past cervical surgery, and absence of concomitant thyroid resection necessity. In these patients, iPTH levels were monitored intraoperatively. Confirmation criteria for iPTH values were a return to normal level or a decrease >50 % of basal iPTH level.
Results
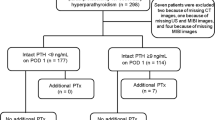
There were 197 PHP operations during the study period: 118 MIP and 79 bilateral neck explorations (BNEs). The MIP success rate was 95 % (112/118) with a preoperative MIBI scan ± CT accurate in 94 % (111/118) of the patients and with correct iPTH in 90 % (106/118) of the cases. Among the 12 iPTH levels that did not meet the confirmation criteria, 10 returned to normal range by postoperative day 2. Treatment failure appeared in three patients (one BNE, two MIPs).
Conclusions
Tc-99m-MIBI dual-phase scintigraphy with SPECT/CT is the key examination for functional and morphological parathyroid adenoma localization. If preoperative scintigraphy is obvious and intraoperative assessment is clear, one could possibly safely omit iPTH, as it may lead to unnecessary BNE in primary PHP.


Similar content being viewed by others
References
Clarke BL (2013) Epidemiology of primary hyperparathyroidism. J Clin Densitom 16:8–13
Press DM, Siperstein AE, Berber E, Shin JJ, Metzger R, Monteiro R et al (2013) The prevalence of undiagnosed and unrecognized primary hyperparathyroidism: a population-based analysis from the electronic medical record. Surgery 154:1232–1237
Hessman O, Westerdahl J, Al-Suliman N, Christiansen P, Hellman P, Bergenfelz A (2010) Randomized clinical trial comparing open with video-assisted minimally invasive parathyroid surgery for primary hyperparathyroidism. Br J Surg 97:177–184
Rio PD, Vicente D, Maestroni U, Totaro A, Pattacini GMC, Avital I et al (2013) A comparison of minimally invasive video-assisted parathyroidectomy and traditional parathyroidectomy for parathyroid adenoma. J Cancer 4:458–463
Tibblin S, Bondeson AG, Ljungberg O (1982) Unilateral parathyroidectomy in hyperparathyroidism due to single adenoma. Ann Surg 195:245–252
Bergenfelz A, Lindblom P, Tibblin S, Westerdahl J (2002) Unilateral versus bilateral neck exploration for primary hyperparathyroidism: a prospective randomized controlled trial. Ann Surg 236:543–551
Staudenherz A, Abela C, Niederle B, Steiner E, Helbich T, Puig S et al (1997) Comparison and histopathological correlation of three parathyroid imaging methods in a population with a high prevalence of concomitant thyroid diseases. Eur J Nucl Med 24:143–149
Sfakianakis GN, Irvin GL, Foss J, Mallin W, Georgiou M, Deriso GT et al (1996) Efficient parathyroidectomy guided by SPECT-MIBI and hormonal measurements. J Nucl Med 37:798–804
Akbaba G, Berker D, Isik S, Aydin Y, Ciliz D, Peksoy I et al (2012) A comparative study of pre-operative imaging methods in patients with primary hyperparathyroidism: ultrasonography, 99mTc sestamibi, single photon emission computed tomography, and magnetic resonance imaging. J Endocrinol Investig 35(4):359–364
Tokmak H, Demirkol MO, Alagöl F, Tezelman S, Terzioglu T (2014) Clinical impact of SPECT-CT in the diagnosis and surgical management of hyper-parathyroidism. Int J Clin Exp Med 7(4):1028–1034
Swanson TW, Chan SK, Jones SJ, Bugis S, Irvine R, Belzberg A et al (2010) Determinants of Tc-99m sestamibi SPECT scan sensitivity in primary hyperparathyroidism. Am J Surg 199:614–620
Slepavicius A, Beisa V, Janusonis V, Strupas K (2008) Focused versus conventional parathyroidectomy for primary hyperparathyroidism: a prospective, randomized, blinded trial. Langenbecks Arch Surg 393:659–666
Westerdahl J, Bergenfelz A (2007) Unilateral versus bilateral neck exploration for primary hyperparathyroidism: five-year follow-up of a randomized controlled trial. Ann Surg 246:976–980
Bergenfelz A, Kanngiesser V, Zielke A, Nies C, Rothmund M (2005) Conventional bilateral cervical exploration versus open minimally invasive parathyroidectomy under local anaesthesia for primary hyperparathyroidism. Br J Surg 92:190–197
Barczyński M, Cichoń S, Konturek A, Cichoń W (2006) Minimally invasive video-assisted parathyroidectomy versus open minimally invasive parathyroidectomy for a solitary parathyroid adenoma: a prospective, randomized, blinded trial. World J Surg 30:721–731
Miccoli P, Bendinelli C, Berti P, Vignali E, Pinchera A, Marcocci C (1999) Video-assisted versus conventional parathyroidectomy in primary hyperparathyroidism: a prospective randomized study. Surgery 126:1117–1121
Irvin GL, Dembrow VD, Prudhomme DL (1993) Clinical usefulness of an intraoperative “quick parathyroid hormone” assay. Surgery 114:1019–1022
Bergenfelz A, Nordén NE, Ahrén B (1991) Intraoperative fall in plasma levels of intact parathyroid hormone after removal of one enlarged parathyroid gland in hyperparathyroid patients. Eur J Surg 157:109–112
Dindo D, Demartines N, Clavien P-A (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Henry J-F, Sebag F, Tamagnini P, Forman C, Silaghi H (2004) Endoscopic parathyroid surgery: results of 365 consecutive procedures. World J Surg 28:1219–1223
Lombardi CP, Raffaelli M, Traini E, Di Stasio E, Carrozza C, De Crea C et al (2008) Intraoperative PTH monitoring during parathyroidectomy: the need for stricter criteria to detect multiglandular disease. Langenbecks Arch Surg 393:639–645
Lee S, Ryu H, Morris LF, Grubbs EG, Lee JE, Harun N et al (2014) Operative failure in minimally invasive parathyroidectomy utilizing an intraoperative parathyroid hormone assay. Ann Surg Oncol 21:1878–1883
Stalberg P, Sidhu S, Sywak M, Robinson B, Wilkinson M, Delbridge L (2006) Intraoperative parathyroid hormone measurement during minimally invasive parathyroidectomy: does it “value-add” to decision-making? J Am Coll Surg 203:1–6
Carter AB, Howanitz PJ (2003) Intraoperative testing for parathyroid hormone: a comprehensive review of the use of the assay and the relevant literature. Arch Pathol Lab Med 127:1424–1442
Bieglmayer C, Prager G, Niederle B (2002) Kinetic analyses of parathyroid hormone clearance as measured by three rapid immunoassays during parathyroidectomy. Clin Chem 48:1731–1738
Ito F, Sippel R, Lederman J, Chen H (2007) The utility of intraoperative bilateral internal jugular venous sampling with rapid parathyroid hormone testing. Ann Surg 245:959–963
Emmolo I, Corso HD, Borretta G, Visconti G, Piovesan A, Cesario F et al (2005) Unexpected results using rapid intraoperative parathyroid hormone monitoring during parathyroidectomy for primary hyperparathyroidism. World J Surg 29:785–788
Sharma J, Milas M, Berber E, Mazzaglia P, Siperstein A, Weber CJ (2008) Value of intraoperative parathyroid hormone monitoring. Ann Surg Oncol 15:493–498
Goltzman D, Hendy G (2001) Parathyroid hormone. Principles and practice of endocrinology and metabolism, 3rd edn. Lippincott Williams & Wilkins, Philadelphia, pp 497–512
Abood A, Vestergaard P (2013) Increasing incidence of primary hyperparathyroidism in Denmark. Dan Med J 60:A4567
Siilin H, Lundgren E, Mallmin H, Mellström D, Ohlsson C, Karlsson M et al (2011) Prevalence of primary hyperparathyroidism and impact on bone mineral density in elderly men: MrOs Sweden. World J Surg 35:1266–1272
Richert L, Trombetti A, Herrmann FR, Triponez F, Meier C, Robert JH et al (2009) Age and gender distribution of primary hyperparathyroidism and incidence of surgical treatment in a European country with a particularly high life expectancy. Swiss Med Wkly 139:400–404
Twigt BA, Vollebregt AM, van Dalen T, Smits AB, Consten ECJ, van Vroonhoven TJMV et al (2011) Shifting incidence of solitary adenomas in the era of minimally invasive parathyroidectomy. A multi-institutional study. Ann Surg Oncol 18:1041–1046
Clerici T, Brandle M, Lange J, Doherty GM, Gauger PG (2004) Impact of intraoperative parathyroid hormone monitoring on the prediction of multiglandular parathyroid disease. World J Surg 28:187–192
Abboud B, Sleilaty G, Helou E, Mansour E, Tohme C, Noun R et al (2005) Existence and anatomic distribution of double parathyroid adenoma. Laryngoscope 115:1128–1131
Milas M, Wagner K, Easley KA, Siperstein A, Weber CJ (2003) Double adenomas revisited: nonuniform distribution favors enlarged superior parathyroids (fourth pouch disease). Surgery 134:995–1000
Papier A, Kenig J, Barczyński M (2014) Evaluation of different intraoperative iPTH assay criteria in monitoring of minimally invasive parathyroidectomy for primary hyperparathyroidism. Przegla̧d Lek 71:14–18
Barczynski M, Konturek A, Hubalewska-Dydejczyk A, Cichon S, Nowak W (2009) Evaluation of Halle, Miami, Rome, and Vienna intraoperative iPTH assay criteria in guiding minimally invasive parathyroidectomy. Langenbecks Arch Surg 394:843–849
Carneiro DM, Irvin GL (2002) New point-of-care intraoperative parathyroid hormone assay for intraoperative guidance in parathyroidectomy. World J Surg 26:1074–1077
Riss P, Kaczirek K, Heinz G, Bieglmayer C, Niederle B (2007) A “defined baseline” in PTH monitoring increases surgical success in patients with multiple gland disease. Surgery 142:398–404
Irvin GL, Solorzano CC, Carneiro DM (2004) Quick intraoperative parathyroid hormone assay: surgical adjunct to allow limited parathyroidectomy, improve success rate, and predict outcome. World J Surg 28:1287–1292
Carneiro DM, Solorzano CC, Nader MC, Ramirez M, Irvin GL (2003) Comparison of intraoperative iPTH assay (QPTH) criteria in guiding parathyroidectomy: which criterion is the most accurate? Surgery 134:973–979
Mihai R, Palazzo FF, Gleeson FV, Sadler GP (2007) Minimally invasive parathyroidectomy without intraoperative parathyroid hormone monitoring in patients with primary hyperparathyroidism. Br J Surg 94:42–47
Twigt BA, van Dalen T, Vollebregt AM, Kortlandt W, Vriens MR, Borel Rinkes IHM (2012) The additional value of intraoperative parathyroid hormone assessment is marginal in patients with nonfamilial primary hyperparathyroidism: a prospective cohort study. Am J Surg 204:1–6
Schenk WG, Hanks JB, Smith PW (2013) Surgeon-performed ultrasound for primary hyperparathyroidism. Am Surg 79:681–685
Ryan S, Courtney D, Timon C (2014) Co-existent thyroid disease in patients treated for primary hyperparathyroidism: implications for clinical management. Eur Arch Oto-Rhino-Laryngol 272:419–423
Gómez-Ramírez J, Sancho-Insenser JJ, Pereira JA, Jimeno J, Munné A, Sitges-Serra A (2010) Impact of thyroid nodular disease on 99mTc-sestamibi scintigraphy in patients with primary hyperparathyroidism. Langenbecks Arch Surg 395:929–933
Authors’ contributions
GRJ: study conception and design, acquisition of data, analysis and interpretation of data, drafting of the manuscript, and acceptance of the final version.
ND: study conception and design, analysis and interpretation of data, critical revision of the manuscript, and acceptance of the final version.
LP: analysis and interpretation of data, critical revision of the manuscript, and acceptance of the final version.
AB: analysis and interpretation of data, critical revision of the manuscript, and acceptance of the final version.
MM: study conception and design, acquisition of data, analysis and interpretation of data, critical revision of the manuscript, and acceptance of the final version.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
- This study received no particular funding.
- This retrospective study based on chart review was in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
- Informed consent was obtained from all individual participants included in the study.
Sources of financial support
None.
Conflicts of interest
Gaëtan-Romain Joliat, Nicolas Demartines, Luc Portmann, Ariane Boubaker, and Maurice Matter have no conflicts of interest to disclose.
Rights and permissions
About this article

Cite this article
Joliat, GR., Demartines, N., Portmann, L. et al. Successful minimally invasive surgery for primary hyperparathyroidism: influence of preoperative imaging and intraoperative parathyroid hormone levels. Langenbecks Arch Surg 400, 937–944 (2015). https://doi.org/10.1007/s00423-015-1358-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-015-1358-z