
Abstract
Purpose
To assess the cost-effectiveness of Multiplex Ligation-dependent Probe Amplification (MLPA, P095 kit) compared to karyotyping.
Methods
A cost-minimization analysis alongside a nationwide prospective clinical study of 4,585 women undergoing amniocentesis on behalf of their age (≥36 years), an increased risk following first trimester prenatal screening or parental anxiety.
Results
Diagnostic accuracy of MLPA (P095 kit) was comparable to karyotyping (1.0 95% CI 0.999–1.0). Health-related quality of life did not differ between the strategies (summary physical health: mean difference 0.31, p = 0.82; summary mental health: mean difference 1.91, p = 0.22). Short-term costs were lower for MLPA: mean difference €315.68 (bootstrap 95% CI €315.63–315.74; −44.4%). The long-term costs were slightly higher for MLPA: mean difference €76.42 (bootstrap 95% CI €71.32–81.52; +8.6%). Total costs were on average €240.13 (bootstrap 95% CI €235.02–245.23; −14.9%) lower in favor of MLPA. Cost differences were sensitive to proportion of terminated pregnancies, sample throughput, individual choice and performance of tests in one laboratory, but not to failure rate or the exclusion of polluted samples.
Conclusion
From an economic perspective, MLPA is the preferred prenatal diagnostic strategy in women who undergo amniocentesis on behalf of their age, following prenatal screening or parental anxiety.
Similar content being viewed by others

Introduction
In many countries, prenatal diagnosis by chorionic villus sampling or amniocentesis is routinely offered to pregnant women who have an increased risk of carrying a child with a chromosomal abnormality. Amniocentesis is the most commonly used invasive prenatal diagnostic procedure in western countries and is performed in about one in 30 pregnancies [1, 2].
Karyotyping is considered the reference test to detect fetal genetic abnormalities in amniotic fluid cells with considerable accuracy [3, 4]. However, it is labor-intensive and the costs are high. Furthermore, obtaining results takes 2–3 weeks and the extensive detection capacity of karyotyping can be perceived as a disadvantage due to the detection of abnormalities with unclear or mild clinical relevance, causing difficult counseling issues, patient anxiety, emotional dilemmas concerning the continuation of pregnancy and, albeit rare, unwarranted pregnancy terminations [5, 6].
Due to these disadvantages, karyotyping as a routine test has been challenged for relatively low-risk indications. In 2003, a molecular PCR-based technique, multiplex ligation-dependent probe amplification (MLPA) became available to detect fetal aneuploidies in amniotic fluid cells [7]. Following the results of preclinical laboratory studies, MLPA has been proposed as a promising alternative for the detection of the most common chromosomal aneuploidies, i.e. trisomy 13, 18, 21 and sex chromosome aneuploidies. Compared to karyotyping, MLPA has several potential advantages; the waiting time for test results is reduced with simultaneous reduction of anxiety, the preceding prenatal counseling process can focus on the most common chromosomal aneuploidies, and the technique is considerably less labor-intensive and more suitable for high-throughput testing, thereby exploiting economies of scale.
Nowadays, much effort has been put into priority setting based on a trade-off of costs and health gains. From an economic perspective, the preferred prenatal diagnostic strategy is the one that overall yields favorable health gains relative to associated cost differences [8].
In order to compare the MLPA and karyotyping strategies in terms of diagnostic accuracy, health-related quality of life and cost-effectiveness, we initiated a prospective diagnostic study comparing MLPA with karyotyping in routine clinical practice; the MLPA And Karyotyping, an Evaluation (MAKE) study (ISRCTN47252164) [9]. If MLPA has comparable diagnostic accuracy and is able to reduce maternal anxiety and costs in routine clinical practice, MLPA could present a suitable substitute for karyotyping. Our research question was: what are the costs and effects of MLPA compared to karyotyping when applied to the indications advanced maternal age, increased risk following prenatal screening and anxiety?
Materials and methods
Clinical study
The clinical MAKE study was set up as a prospective nationwide cohort study enrolling 4,585 consecutive women undergoing amniocentesis for advanced maternal age (≥36 years), increased risk following prenatal screening or anxiety. Other referral indications were excluded (e.g. ultrasound abnormalities) since these are associated with an increased risk of a chromosomal abnormality other than trisomies 13, 18, 21 and sex chromosome abnormalities. Details of the study design have been published elsewhere [9, 10]. In summary, after obtaining informed consent, amniocentesis was carried out by specifically trained obstetricians. All amniotic fluid samples were tested with both MLPA and karyotyping, allowing a pair-wise comparison of MLPA and the reference test; karyotyping. Sample size was estimated to demonstrate non-inferiority (i.e. comparable diagnostic accuracy) of MLPA to karyotyping. During a pre-trial meeting, experts in prenatal diagnosis, clinical epidemiology and statistics agreed on a critical non-inferiority margin of 0.002. At least 4,497 paired test results were needed (one-sided alpha 0.05, power 0.90) to be able to reject the null hypothesis that MLPA is inferior to karyotyping.
MLPA
DNA was isolated from 1–8 ml uncultured amniotic fluid samples, depending on the total amount of amniotic fluid received. DNA was isolated from amniotic fluid cells through lysis of cell pellets and proteinase K treatment using standard procedures. This DNA was purified using a QIAamp kit (Qiagen, Germany) according to the manufacturer’s instructions. MLPA samples were analyzed with the commercially available SALSA MLPA P095 kit (MRC Holland, the Netherlands). For each genomic target, a set of two probes is designed to hybridize immediately adjacent to each other on the same target strand. Both probes consist of a short target sequence and a universal polymerase chain reaction (PCR) primer-binding site. One of the probes contains a stuffer sequence with a unique length and sequence. Following hybridization, each pair of adjacent probes is joined by a ligation reaction. Next, PCR is performed using a fluorescent-labeled primer pair, which ensures that the relative yield of each of the PCR products is proportional to the amount of each of the target sequences. The different length products are separated on an automated capillary sequencer. The size and peak areas for each probe are quantified and analyzed by data analyzing software (GeneMarker, SoftGenetics, LLC, State College, PA, USA, or Genescan and Genemapper version 3.7/4.0, Applied Biosystems, CA, USA)[7]. Relative probe signals are calculated and compared with samples of normal male and female sex. In chromosomally normal samples, the relative probe signal is expected to be 1 for all probes. A normal value is defined as a relative probe signal between 0.7 and 1.3. A relative probe value of <0.7 indicates a monosomy, whereas a relative probe value of >1.3 indicates a trisomy. Technicians had a molecular genetics or a cytogenetics background; all were trained in the execution of MLPA prior to the study onset. MLPA was performed in duplicate, provided that at least 2 ml of amniotic fluid was available. All eight genetic centers have different sample throughput, depending on the number of patients in their referring prenatal diagnostic centers.
Karyotyping
Fetal cells were cultured and karyotyped after banding. Routinely, metaphases of at least ten colonies were investigated. All centers followed national quality guidelines but minor differences in the number of cell colonies cultured, chromosome banding and reporting of the results were allowed [11].
Economic analysis framework
The economic analysis was performed from the societal perspective which means that all significant costs and health effects both in the short and long term should be considered, regardless of who experiences the costs or the health gains [8]. The economic evaluation was initially designed as a cost-effectiveness analysis (CEA) [8], with incremental costs per case of Down’s syndrome missed by MLPA. In case of comparable diagnostic accuracy for the detection of Down syndrome, a cost-utility analysis (CUA) was considered the appropriate economic framework, calculating the difference in costs in relation to differences in health-related quality of life [8]. If differences in quality of life between the strategies were also absent, a cost-minimization analysis (CMA) was carried out. CMA implies that the preferred strategy from the societal perspective is the one with lowest costs, since health effects are equal [8]. We did not include a do-nothing strategy, since the target population is eligible for karyotyping.
Health-related quality of life
Alongside the clinical MAKE study we assessed health-related quality of life (HRQoL) in two groups: group 1 having karyotyping and group 2 having MLPA. Included were women with the indications maternal age, increased risk following the findings of prenatal screening for Down syndrome and parental anxiety. We used the MOS SF-36 health survey, measuring overall mental and overall physical health. Mental and physical health were measured before amniocentesis and at day 63 following amniocentesis, since the SF-36 focuses on health status during the preceding 4 weeks. Overall mental and physical health was calculated according to accepted scoring algorithms [12].
Costs
We distinguished the costs of the MLPA and karyotyping strategies in two components; short- and long-term costs. The first component, the short-term costs, comprises all societal costs that occur between amniocentesis and parents’ decision to terminate or continue pregnancy. These costs consist of the costs of the diagnostic tests and other costs. The second component consists of the long-term costs, i.e. all societal costs that occur between parents’ decision to terminate or continue pregnancy and lifetime costs. Although it is controversial whether the costs associated with chromosomal abnormalities should be included in this type of analysis [13–15], we decided to display the impact of missed chromosomal abnormalities on long-term costs.
Short-term and long-term costs were further distinguished in direct medical costs (i.e. laboratory costs, additional in-hospital medical costs during follow-up), direct non-medical costs (patient expenses, e.g. patient time and travel costs) and indirect costs (societal costs due to absence from work) [8].
The main outcome parameters were the difference in short-term costs between the MLPA and TKT strategies, the long-term cost difference, and the overall cost difference.
Short-term costs
The short-term costs consisted of the costs associated with performing MLPA and/or karyotyping and other costs related to the testing process. Direct medical costs of performed tests were calculated as actual volumes of resource use multiplied by the costs per unit of resource. Number and type of tests performed were recorded in the clinical record form or obtained by observation or questionnaire. We used direct observations and measurements of working time, materials, and depreciation costs of equipment to quantify resource use associated with MLPA. Costs per units were obtained from a university hospital’s budgetary and accounting system and were subsequently applied to the resource use observed in a small and large centre. The costs per units reflected the costs of staff, materials, equipment, housing and departmental and hospital overheads.
The other short-term costs consisted of additional diagnostic tests, costs of genetic counseling in case a chromosomal abnormality was detected, and travel costs. Use of additional diagnostic tests was recorded in the case record form. In case of a chromosomal abnormality, we assumed parents visited the hospital twice for genetic counseling [50% of cases by performed by gynecologists (trisomies 13, 18 and 21) and 50% seen by clinical geneticists and social workers (all other chromosomal abnormalities)]. Travel costs per client were based on the average travel distance to hospitals [16]. The unit costs of direct non-medical costs were based on Dutch guidelines [16, 17]. Short-term indirect costs did not occur.
Study-specific costs as well as costs not associated with diagnostic test performance (prenatal test counseling, amniocentesis, ultrasound, sample transport, procedure-related miscarriages) were expected to be independent of the type of diagnostic test, and were therefore excluded from analysis. Given the time horizon no discount rate is used. When necessary, costs were updated to the 2007 price level by using the Dutch Consumer Price Index [18].
Long-term costs
The long-term costs were defined as the costs associated chromosomal abnormalities and consisted of (1) incremental costs for a child having a chromosomal abnormality and (2) costs for parents of the affected child. We first categorized chromosomal abnormalities according to clinical relevance: severe consequences and other chromosomal abnormalities leading to severe fetal morbidity or mortality (category I: includes trisomies 13, 18 and 21); uncertain consequences (including sex chromosomal abnormalities) and de novo balanced chromosomal abnormalities which can lead to 6% mental retardation and/or congenital abnormalities [19] (category II); and no consequences including inherited chromosomal abnormalities and chromosomal abnormalities of known clinical irrelevance (category III). For category I chromosomal abnormalities, we used an incremental lifetime cost of €200.000 per child [20–22], a weighted average of the costs of trisomies 13, 18 and 21 adjusted for the average costs per child. The costs of a category II abnormality were estimated to be 6% of the costs of a child with category I abnormality. Category III abnormalities were considered not to induce extra costs.
Productivity loss due to absence from work in case of a chromosomal abnormality was estimated according to the friction cost method [16]. In case the pregnancy was terminated, both parents were considered to have a sick leave; on average 6 weeks for mothers and 2 weeks’ leave for partners. If the parents decided to continue the pregnancy in case of a severe chromosomal abnormality, the productivity loss exceeded the friction period (22 weeks) and no extra costs beyond the friction period were included. Assuming pregnant women to have on average one child, working 26 h/week and aged of 25–44 years, the productivity loss is €33.60/h lost [18]. Assuming the partner to be male, aged 25–44 years old and working fulltime, his productivity loss is on average €40.86/h lost [18].
Sensitivity analysis
We used a sensitivity analysis to test the robustness of the cost differences. We varied the major assumptions underlying the cost-effectiveness model for the following parameters: (1) proportion of failed MLPA results, according to the 5th and 95th percentiles of the observed failure rate; (2) only samples with clear amniotic fluid are analyzed with MLPA, all other samples with karyotyping; (3) the proportion of terminated pregnancy in case of category I chromosomal abnormalities varies from 70–80%); (4) women are allowed individual choice: 50% of women opts for MLPA and 50% for karyotyping [23]; (5) sample throughput based on a small centre (n = 286) and a large centre (n = 1,153); (6) one nationwide MLPA laboratory; (7) all samples are analyzed with both MLPA and karyotyping. Parameters 1 and 5 are subject to different laboratory practices. Parameter 3 might relate to societal trends, counseling style or the counselor’s medical specialty [24]. Parameters 2, 4, 6, and 7 might change following changes in prenatal diagnostic protocols or guidelines.
Statistical analysis
Data were recorded and analyzed by using statistical software (SPSS version 16.0; SPSS, Chicago, Illinois). Observed data described with descriptive statistical measures; medians with range, or mean differences with 95% confidence intervals (CIs). Due to skewness of cost data, the 95% CI of the mean short-term, long-term and overall cost differences between the strategies were obtained with the nonparametric bootstrap method, based on 10,000 bootstrap samples [25]; p value less than 0.05 (two-tailed) was considered statistically significant.
Results
Patients and test results
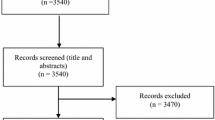
Between March 2007 and October 2008 we included 4,585 consecutively pregnant women. Patient and procedural characteristics are displayed in Table 1. In 4,484/4,585 samples (97.8%) MLPA and karyotyping were concordant, showing normal results in 4,387/4,585 (95.7%) and aneuploidy in 98/4,585 (2.1%). Discordant results were found in 26/4,585 (0.6%) samples, representing an abnormal karyotype undetected by MLPA. All aneuploidies of chromosomes 13, 18, 21 and non-mosaic X and Y were also detected by MLPA. MLPA, by design, could not detect three severe chromosomal abnormalities other than trisomies 13, 18, 21. In 75 cases (1.6%) the MLPA test result failed. Karyotyping failed in one of these 75 cases (0.02%). Diagnostic accuracy of MLPA was comparable (non-inferior) to karyotyping (1.0 95% CI 0.999–1.0). Sensitivity and specificity for the detection of trisomies 13, 18, 21, X and Y were 100% (95% CI 96–100%) and 100% (95% CI 99.9–100%), respectively [11]. There were neither statistical nor clinically relevant differences in HRQoL. Summary physical and mental health scores between people receiving a karyotype or MLPA did not differ (mean difference 0.31; 95% CI −3.06 to 2.44; p 0.82 and mean difference 1.91 95% CI −1.15 to 4.99; p 0.22, respectively) (see Table S1). Therefore, we considered cost-minimization analysis the appropriate framework.
Short-term costs
The test costs of the MLPA test performed in duplicate were €344,60 per sample (65% direct and 35% overhead costs), while the costs of karyotyping was €668,00 per sample (74% direct and 26% overhead costs). Table 2 details the volumes of resource use, unit costs per resource and the total short-term costs.
In the MLPA strategy, 173 subsequent karyotyping were performed because MLPA failed (n = 75) or because MLPA showed a chromosomal abnormality and inheritance patterns needed to be examined (n = 98). Repeat amniocentesis did not occur. MLPA was repeated in 1.6% (5th to 95th percentile 1.3–2.1%) due to an inconclusive result. Five subsequent FISH analyses were done: three because MLPA showed a deletion on a single probe and the laboratory wished to exclude a sub-microscopic deletion, and two for a mosaic chromosome pattern (combined mosaic pattern of Turner and Down syndrome and a mosaic pattern for Turner syndrome and a normal female cell line). In 22 cases in the MLPA strategy and 34 cases in the karyotyping strategy, advanced ultrasound examination was required to exclude other severe congenital abnormalities (e.g. cardiac abnormalities) in the presence of the chromosomal abnormality to support the decision to continue or terminate the pregnancy.
In the karyotyping strategy, 11 subsequent FISH analysis were performed for various reasons; additional information on the grade of mosaicism (mosaic pattern Turner and Down syndrome, mosaic pattern of Turner syndrome) (n = 2), for marker chromosomes (n = 4), de novo unbalanced chromosomal abnormalities (n = 2), a chromosomal abnormality which appeared to be a normal variant (n = 2), and for a mosaic pattern of male and female karyotype which was determined to be a culture artefact (n = 1). In the latter case, biochemical investigation on amniotic fluid was also carried out to determine the testosterone/FSH ratio and karyotyping was repeated in a postnatal sample. In 24 cases parental karyotyping was performed to address the origin of the chromosomal abnormality (inherited or de novo). To assess the consequences of the de novo interstitial deletion, MLPA on subtelomeres and a genomic micro array was carried out. One karyotype failed due to contaminated amniotic fluid (blood and clots). Repeat amniocentesis was offered but the prospective parents declined.
The median short-term costs per sample, i.e. from amniocentesis until the decision to continue or terminate pregnancy, were €344.60 (range €344.60–3.216.08) for the MLPA strategy and €668.00 (range €668.00–4.669.48) for the karyotyping strategy. The short-term costs of the MLPA strategy were on average €315.68 (bootstrap 95% CI €315.63–315.74) lower than the karyotyping strategy (−44.4%).
Long-term and total costs
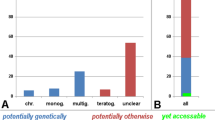
Table 3 displays the main volumes of resource use, the unit costs per resource use and the long-term costs following the decision to continue or terminate pregnancy. Seventy-six pregnancies in the MLPA strategy (72 clinically severe, 4 clinically uncertain, 0 clinically not relevant) and 79 pregnancies in the karyotyping strategy (74 clinically severe, 5 clinically uncertain, 0 clinically not relevant) were terminated (Table S2). In two pregnancies, postnatal karyotyping was carried out to confirm the prenatal diagnosis (mosaic marker chromosome and mosaic Turner).
The median long-term costs per sample, i.e. from the decision to continue or terminate pregnancy onwards, were €0.00 (range €0.00–233,940.00) for the MLPA strategy and €0.00 (range €0.00 to 237,000.08) for the karyotyping strategy (Table 2). The long-term costs of the MLPA strategy were on average €76.42 higher compared to the karyotyping strategy (bootstrap 95% CI €71.32–81.52; +8.6%) per sample.
The total costs, including both short- and long-term costs, were median €344.60 (range €344.60–237,000.08) for the MLPA strategy and €668.00 (range €668.00–238,956.48) for the karyotyping strategy. The total cost difference was €240.13 (bootstrap 95% CI €235.02–€245.23) in favor of MLPA (cost reduction −14.9%).
Sensitivity analysis
Table 4 displays the results of the sensitivity analyses. Total MLPA costs were sensitive to the following parameters: the proportion of women deciding to terminate pregnancy, women allowed individual choice, the level of sample throughput, and performing both MLPA and karyotyping. Except for the combined MLPA and karyotyping strategy, the total costs difference remained in favor of MLPA.
Discussion
We evaluated the cost-effectiveness of two prenatal diagnostic test strategies: MLPA and karyotyping. Diagnostic accuracy of MLPA was comparable to karyotyping and health-related quality of life was equal between strategies. For the complete testing process, the MLPA strategy lead to a 14.9% cost reduction per amniotic fluid sample for women with relatively low-risk indications (−44.4% on the short and +8.6% on the long term).
Our study has several limitations. Firstly, we used the data of the nationwide prospective MAKE study which prioritized karyotyping, since at least 12 ml of amniotic fluid was required. The failure rate of MLPA (1.6%) may be lower when MLPA is applied as stand-alone technique since MLPA requires at least 1–2 ml. Sensitivity analysis, however, showed that variations in failure rate had little impact on the overall cost difference. Secondly, we were unable to measure quality of life for women who decided to continue or terminate pregnancy in case of a chromosomal abnormality and in parents with rare prenatally undetected fetal chromosomal abnormalities. However, diagnostic accuracy was high and comparable; we can speculate that the decision to continue or terminate pregnancy in case of a chromosomal abnormality is the same, regardless of the diagnostic test used. The three severe chromosomal abnormalities undetected by MLPA may result in a decreased quality of life at the individual level but not in differences at the group level. Thirdly, we did not adjust the costs associated with pre-test counseling. We expect that targeted testing reduces complex counseling issues and is therefore less costly. Furthermore, three FISH analysis were done following MLPA to exclude a sub-microscopic deletion. If MLPA is implemented as a stand-alone test to detect trisomies 13, 18, 21 X and Y, our research group advises to neglect the interpretation of the quantification of single probes. Taking this into account, the cost reduction of MLPA compared to karyotyping may be even larger than we estimated. Finally, costs were based on Dutch health care costs, which might differ from costs in other countries. That does not imply that the outcome of MLPA being the strategy with lowest costs is not externally valid for other countries. Hence, overall cost differences between countries do affect the absolute cost differences, but do not affect the ordering of strategies in terms of costs.
Compared to other RAD techniques, MLPA and quantitative fluorescent polymerase chain reaction (QF-PCR) are both suitable techniques for high-throughput testing at lower costs compared to fluorescent in situ hybridization (FISH) [26]. A cost analysis of QF-PCR and revealed that both tests are sensitive to sample throughput and staff skill-mix FISH (2003) [26]. For laboratories with a throughput of 1,000 samples per annum, karyotyping is the most expensive test to perform, with FISH and Q-PCR calculated to incur approximately half the direct test costs of karyotyping [26]. However, these studies did not include long-term costs. Due to differences in methodology, a full comparison with our study is impossible.
Costs differences were insensitive to variations in failure rate, or using MLPA on contaminated amniotic fluid samples. However, the costs of MLPA proved sensitive to the proportion of terminated pregnancies and therefore to societal trends, but this is unlikely to affect the overall cost difference. Furthermore, the costs of the MLPA strategy were sensitive to sample throughput as well as the concentration of MLPA analyses in one nationwide centre. This shows that the costs and cost differences depend on the way care is organized. Since the impact of concentration on costs was larger than the impact of higher throughput, we recommend the use of one (or several) nationwide MLPA laboratories. Our study also shows that a combined strategy of MLPA followed by karyotyping is rather inefficient. Costs are considerably increased without any gain in diagnostic accuracy or health-related quality of life compared to the karyotyping only strategy.
The provision of a rapid, unambiguous and a low cost result is an incentive to implement MLPA. Successful implementation, however, also requires the support of pregnant women. If one supports individualized choice for principle or other reasons [27], one could argue that the decision to either obtain as much cytogenetic information as possible versus a rapid but specific result on the most common chromosomal abnormalities is most appropriately made by individuals who will bear the responsibility for raising the child. Our study shows that allowing individualized choice—assuming that 50% chooses karyotyping and 50% chooses MLPA [23]—also has large impact on costs, reducing the cost difference of €240 per sample to €83 per sample). While individual choice as strategy is less efficient than a uniform strategy in which every patient would receive MLPA, the overall cost reduction is still in favor of MLPA over the current karyotyping strategy. One could argue that offering a choice between the tests meets most individual needs and wishes, and thereby might outweigh the cost difference. In a discrete choice experimentation [28], women valued the comprehensive information of karyotyping at £791 and the simple and quick information of a Down only test at £690. This supports our idea that the option to choose may outweigh the previously mentioned efficiency loss of €240 per sample to €83 per sample.
Conclusion
In summary, MLPA is able to detect trisomies 13, 18, 21, X and Y with comparable diagnostic accuracy [10, 29, 30] and without adverse effect on quality of life at considerably lower costs for the complete testing process. We conclude that MLPA is the preferred strategy and recommend substitution of karyotyping for MLPA for relatively low-risk indications. Future research should be done to evaluate which RAD technique delivers best ‘value for money’, to estimate the cost-effectiveness of this RAD technique on chorionic villus biopsy, and to evaluate the most advantageous organization for the optimal RAD technique.
This study was approved by the medical review ethics committee of the Onze Lieve Vrouwe Gasthuis (reference number 06032).
References
Ogilvie CM, Lashwood A, Chitty L et al (2005) The future of prenatal diagnosis: rapid testing or full karyotype? An audit of chromosome abnormalities and pregnancy outcomes for women referred for Down’s syndrome testing. BJOG 112:1369–1375
Nagel HT, Knegt AC, Kloosterman MD et al (2007) Prenatal diagnosis in the Netherlands, 1991–2000: number of invasive procedures, indications, abnormal results and terminations of pregnancy. Prenat Diagn 27:251–257
Tabor A, Madsen M, Obel EB et al (1986) Randomised controlled trial of genetic amniocentesis in 4606 low-risk women. Lancet 1:1287–1293
Los FJ, van Den Berg C, Wildschut HI et al (2001) The diagnostic performance of cytogenetic investigation in amniotic fluid cells and chorionic villi. Prenat Diagn 21:150–158
van Zwieten MCB, Willems DL, Litjens LL et al (2005) How unexpected are unexpected findings in prenatal cytogenetic diagnosis? A literature review. Eur J Obstet Gynecol Reprod Biol 120:15–20
Leung WC, Lau ET, Lao TT, Tang MH (2004) Rapid aneuploidy screening (FISH or QF-PCR): the changing scene in prenatal diagnosis? Expert Rev Mol Diagn 4:333–337
Slater HR, Bruno DL, Ren H et al (2003) Rapid, high throughput prenatal detection of aneuploidy using a novel quantitative method (MLPA). J Med Genet 40:907–912
Gold MR, Siegel JE, Russell LB, Weinstein MC (1996) Cost-effectiveness in health and medicine. Oxford University Press, New York
Boormans EM, Birnie E, Wildschut HI et al (2008) Multiplex ligation-dependent probe amplification versus karyotyping in prenatal diagnosis: the MAKE study. BMC Pregnancy Childbirth 8:18
Boormans EM, Birnie E, Oepkes D et al (2010) Comparison of multiplex ligation-dependent probe amplification and karyotyping in prenatal diagnosis. Obstet Gynecol 115:297–303
Dutch Society of Human Genetics (2003) Quality in clinical cytogenetics conditions, standards and tests. NVHG, Amsterdam
Aaronson NK, Muller M, Cohen PD et al (1998) Translation, validation, and norming of the Dutch language version of the SF-36 Health Survey in community and chronic disease populations. J Clin Epidemiol 51:1055–1068
Harris RA, Washington AE, Nease RF Jr, Kuppermann M (2004) Cost utility of prenatal diagnosis and the risk-based threshold. Lancet 363:276–282
Petrou S (2001) Methodological limitations of economic evaluations of antenatal screening. Health Econ 10:775–778
Shackley P (1996) Economic evaluation of prenatal diagnosis: a methodological review. Prenat Diagn 16:389–395
Oostenbrink JB, Boumans CAM, Koopmanschap MA, Rutten FFH (2004) Handleiding voor kostenonderzoek, methoden en standaard kostprijzen voor economische evaluaties in de gezondheidszorg. College voor zorgverzekeringen, Diemen
van Loenen AC (2004) Farmacotherapeutisch kompas: medisch farmacotherapeutische voorlichting. College voor zorgverzekeringen, Amstelveen
Statistics Netherlands (2008) StatLine, Den Haag: Statistics Netherlands. http://www.statline.cbs.nl. Accessed at 29 June 2009
Warburton D (1991) De novo balanced chromosome rearrangements and extra marker chromosomes identified at prenatal diagnosis: clinical significance and distribution of breakpoints. Am J Hum Gen 49:995–1013
Waitzman NJ, Roman PS, Scheffler RM (1994) Estimates of the costs of birth defects. Inquiry 31:188–205
Leschot NJ, Verjaal M, Treffers PE (1985) A critical analysis of 75 therapeutic abortions. Early Hum Dev 10:287–293
Leschot NJ, Kanhai HHH, van Asperen CJ et al (1990) An evaluation of 75 terminations of pregnancy based on abnormal laboratory findings at first trimester CVS. Clin Genet 38:211–217
Boormans E, Birnie E, Bilardo C et al (2009) Karyotyping or rapid aneuploidy detection in prenatal diagnosis? The different views of users and providers of prenatal care. BJOG 116:1396–1399
Hall S, Marteau TM, Limbert C et al (2001) Counselling following the prenatal diagnosis of Klinefelter syndrome: comparisons between geneticists and obstetricians in five European countries. Community Genet 4:233–238
Barber JA, Thompson SG (2010) Analysis of cost data in randomized trials: an application of the nonparametric bootstrap. Stat Med 19:3219–3236
Grimshaw GM, Szczepura A, Hultén M et al (2003) Evaluation of molecular tests for prenatal diagnosis of chromosome abnormalities. Health Technol Assess 7:1–146
Kassirer JP (1994) Incorporating patients’ preferences into medical decisions. NEJM 330:1895–1896
Ryan M, Diack J, Watson V, Smith N (2005) Rapid prenatal diagnosis for Down syndrome only or longer wait for full karyotype: the views of pregnant women. Prenat Diagn 25:1206–1211
van Opstal D, Boter M, de Jong D, van den Berg C, Brüggenwirth HT, Wildschut HIJ et al (2009) Rapid aneuploidy detection with multiplex ligation-dependent probe amplification: a prospective study of 4000 amniotic fluid samples. Eur J Hum Gen 17:112–121
Kooper AJA, Faas BHW, Kater-Baats E, Feuth T, Janssen JC, van der Burgt I et al (2008) Multiplex Ligation-dependent Probe Amplification (MLPA) as a stand-alone test for rapid aneuploidy detection in amniotic fluid cells. Prenat Diagn 28:1004–1010
Acknowledgments
This study was supported by an unconditional grant 945-27-047 from ZonMW, The Netherlands Organization for Health Research and Development, The Hague, The Netherlands.
Conflict of interest
The authors declare no conflict of interest.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Additional information
On behalf of the MLPA and karyotyping (MAKE) study group. Members of the MAKE study group are given in the Appendix.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Appendix
Appendix
The members of the MAKE study group are: S.L. Bhola, C.M. Bilardo, E. Birnie, E.M.A. Boormans, K. Bouman, J. Creemers, R.J. Galjaard, A.T.T.J. Go, M.J.V. Hoffer, A.C. Knegt, J.M.M. van Lith, M.V.E. Macville, J.G. Nijhuis, D. Oepkes, A.C.C. van Oppen, R. Suijkerbuijk, G.H. Schuring-Blom, A. Smits, H.I.J. Wildschut.
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Boormans, E.M.A., Birnie, E., Hoffer, M.J.V. et al. Economic evaluation of multiplex ligation-dependent probe amplification and karyotyping in prenatal diagnosis: a cost-minimization analysis. Arch Gynecol Obstet 285, 67–75 (2012). https://doi.org/10.1007/s00404-011-1921-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-011-1921-y