
Abstract
Purpose
The ambition of the research group was to develop a sensor-based system that allowed the transfer of results with strain sensors applied to the knee joint. This system was to be validated in comparison to the current static mechanical measurement system. For this purpose, the internal rotation laxity of the knee joint was measured, as it is relevant for anterolateral knee laxity and anterior cruciate ligament (ACL) injury.
Methods
This is a noninvasive measurement method using strain sensors which are applied to the skin in the course of the anterolateral ligament. The subjects were placed in supine position. First the left and then the right leg were clinically examined sequentially and documented by means of an examination form. 11 subjects aged 21 to 45 years, 5 women and 6 men were examined. Internal rotation of the lower leg was performed with a torque of 2 Nm at a knee flexion angle of 30°.
Results
Comparison of correlation between length change and internal knee rotation angle showed a strong positive correlation (r = 1, p < 0.01). Whereas females showed a significant higher laxity vs. males (p = 0.003).
Conclusions
The present study showed that the capacitive strain sensors can be used for reproducible measurement of anterolateral knee laxity. In contrast to the previous static systems, a dynamic measurement will be possible by this method in the future.
Similar content being viewed by others

Introduction
The differentiated diagnosis of rotational laxity of the knee joint is the decisive prerequisite for the correct therapeutic procedure [1]. Until now, the detection of knee laxity has mostly been based on the subjective clinical tests that depend on the examiner. Rotational laxity of the knee joint with anterior cruciate ligament rupture is clinically assessed by the pivot shift test [2]. Because the examination depends on the technique of the examiner, a semi-subjective result is achieved. The commonly used commercially available arthrometers KT 2000 and Rolimeter [3] are able to objectively measure anterior − posterior translation, but the rotational component is not taken into consideration. Moreover, the results can vary depending on the patient's position, the examiner's dominant arm, and involuntary muscle contractions [4]. Even the latest measuring devices such as the "Automatic Knee Arthrometer (AKA)" only measure anterior − posterior translation [5]. The Telos device [6] can only verify varus/valgus laxity translation and anterior − posterior translations. While electromagnetic sensors using the Robotic Knee Test (RKT) System can reliably determine knee rotation, it is a static system with considerable technical effort [7]. According to the clinical experience, the applied high torque often leads to muscular counterstrain of the patient and pain. Moreover, general anesthesia is required for some of these measurements [8]. Because of the complexity, they are rarely applicable in routine clinical diagnosis. Computer navigation [9,10,11,12,13,14] is useful only in the context of surgical procedures. Although it provides reliable results, it is more useful for validation of surgical techniques.
Cadaver studies using amputates [15,16,17] are important for exploring the basics. However, the biomechanical properties of the tissue are altered in the cadaver, so that transferability of the results to in vivo situation is limited. In some cases, clinically intolerable high forces are applied to the knee joint. The force is often transmitted directly through the bone, creating conditions that cannot be reproduced in everyday clinical practice. Nevertheless, these studies are trend setting and important in basic research. Devices from the early days of rotation measurements such as the "Rottometer" [18] showed a high difference between the suggested vs. actual lower leg rotation. Owing to the low frictional connection between the lower leg, ankle joint and foot on the one hand, and the receiving fixation mechanism on the other hand, this bias is favored. In the "rigid" boot of the working group of Tsai [19], this problem was already partially taken into account. Nevertheless, when the knee was in a neutral position, a considerable rotational capacity remained in the joint. Quinn et al. [20] already described in 1991 for the axial examination in internal and external rotation that significantly higher three-dimensional forces and torsional moments act on the knee joint during rotational fixation of the foot and ankle. A validated device developed by the current research group to measure rotational laxity [21,22,23,24,25] takes this fact into account by fixing the talus in a defined dorsal extension and locking the ankle fork. The advantage of the device described here is the possibility of a controlled measurement of the rotation of the lower leg at a defined torque. In addition, it is a purely mechanical and easily transportable device. The sensitivity of most commercially available arthrometers must currently be seen as a weakness in the experimental setup. However, even the current rotational laxity measurement device is a stationary device and thus does not allow laxity measurement under daily physical activity. Therefore, it is the ambition of the research group to develop a sensor-based system that allows the transmission of the results with stretch marks applied to the knee joint and thus also allows mobility of the patient [26]. In the present study, this system was validated in comparison to the current static mechanical measurement system. For validation, the internal rotational laxity of the knee joint was measured, as it is relevant for injuries of the anterolateral ligament complex of the knee and the ACL [27, 28].
Hypothesis: Capacitive strain sensors can be used for reproducible laxity measurement of the anterolateral knee laxity.
Materials and methods
Measuring system
The measuring system consisted of a capacitive strain sensor connected to a flexible circuit board. The electronics on the circuit board were used for data acquisition and transmission. When the sensor strip is stretched, the distance between the fingers of the strain sensor changes, hence the capacitance changes. Consequently, the strain can be measured via the change in capacitance. The measurement system was taped to the knee, with the sensor attached to the skin in the direction of the anterolateral ligament (ALL) at a knee flexion angle of 30°. The bottom of the sensor (made of silicone) and the bottom of the circuit board (made of FR4), was in contact with the knee surface. Importantly, the sensor was attached to the knee by a crosslinking silicone rubber without prestretching. The crosslinking silicone rubber is an orthopedic product. The measuring system was designed to maintain full functionalities for two full days of examination but in the present study, 7 patients were measured for 90 min for one day. During a patient session the knee rotation angle was recorded and monitored by the sensor extension. In the present study, the change in length of the capacitive strain sensor and the associated change in capacitance, expressed by the capacitance charge times, was measured by internal rotation of the knee joint with a defined torque. Capacitance reading was performed using Texas Instruments CC2652R1 ultra-low-power microcontroller. The capacitance was measured using a TDC (Time to digital converter) embedded in the chip. The working principle of the TDC is to measure the charging time of the capacitor which is proportional to the capacitance value [29]. The sensed value is therefore the capacitance charge time, which is proportional to the sensor elongation. The sensor system was used under the constant supervision of physicians specialized in knee surgery and who are familiar with the use of the device. The reliability of the measurement method was defined as primary endpoint.
Measurements
The subjects were placed in supine position. First the left and then the right leg were clinically examined sequentially and documented by means of an examination form (see attached document). Exclusion criteria were the occurrence of pathological findings of ligamentous pathology in the area of the collateral/cruciate ligaments, previous knee operations or restrictions of the range of motion. There were 11 subjects aged 21 to 45 years, 5 females and 6 males. Subjectively, there were no problems in the knee area in any of the subjects. The Laxitester (Ortema Sports Protection, Markgroeningen, Germany) was validated for quantitative measurement of rotational laxity in the knee joint. This has been performed for ligament stable and unstable knees [23, 24]. Because of the large interindividual differences, a comparison was made between the left and right knee. The subject was then placed in supine position on the Laxitester with the respective leg to be examined in the body axis (Fig. 1). Previously, a calibration was performed to determine the length change of the sensor via the capacitance change.

A Longitudinal positioning of the test person on the couch; B Medial support of the knee and lateral positioning of the capacitive strain sensor; C Alignment of the ankle and knee
The knee circumference was measured for each subject. The length change of the strain sensors was corrected according to the knee circumference in order to obtain comparable nondimensional values. To do this, the length change of the respective strain sensor was divided by the circumference of the knee joint over the middle of the patella.
The study was approved by the responsible ethics committee (approval number 487/16).
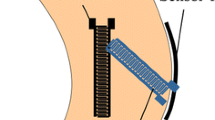
The distal femur rested on a support bench with which a knee joint flexion of 30° was set by height adjustment. The femoral condyles were secured against rotation in the positioning aid by means of a medial post. This also prevented internal rotation and displacement of the femur. The foot was strapped into the holding device without footwear. The second beam was centrally aligned via an adjustable side clamp on the medial and lateral foot edge. In accordance with the above-mentioned previous studies, dorsiflexion was set to 2 Nm using a torquemeter in order to exclude rotational laxity in the ankle joint. The strain sensor was glued in the course of the anterolateral ligament below the lateral epicondyle of the femur to Gerdy’s tubercule. Internal rotation of the lower leg was performed with a torque of 2 Nm at a knee flexion of 30° (Fig. 2).

Positioning of the strain sensor in the course of the ALL and internal rotation of the lower leg with a torque of 2 Nm; the strain sensor was glued in the course of the anterolateral ligament below the lateral epicondyle of the femur to Gerdy’s tubercule
Statistics
Descriptive statistics, linear regression and Spearman's rank correlation were performed. Statistical analysis was performed using SPSS software, version 12.0 (SPSS Inc., Chicago, IL, USA). Basic descriptive statistics were used to describe the patient population. Group differences were tested by age and sex, and measured length change were compared between participants at different rotation angles in 5° increments (10°, 15°, 20°, 25°, 30°, 35°, 40°). Scatter plots were used to evaluate the differences between participants’ values and the variations between different angles. The relationship between the length change and the angle of knee rotation was measured using Spearman's rank correlation to evaluate the monotonic relationship between two variables in non-normal distributed data. The correlation between the change in length and the degree of knee rotation was measured for each side using Spearman's rank correlation coefficient (r) and significance level (p) for all participants, and the collected correlation data of different angles were plotted. Significance was set at 0.05. With a significance level of 5% for two-tailed testing, a power of 80% and an expected difference of 5° with a standard deviation of 4°, 11 subjects were required to obtain a statistically significant difference.
Results
The current study included a total of 11 subjects of which 5 were female and 6 were male. The average age was 28 ± 6 years. Owing to the ethics committee vote, 11 subjects were allowed to participate during the Covid pandemic.
The results obtained from a simplified knee joint model exhibited a reproducible relative capacitance change of 0.01 F for every 5° angle change from 10° through 45° rotation [30].
A significant sex difference was noted in the range of internal rotation of the knee (p = 0.003). The range of rotation was larger in the female participants than in the male participants. As for the measured length changing values, the measurements presented showed an individualized result for each participant, which tended to decrease with increasing internal rotation angle, with no age or sex differences (Figs. 3 and 4). The stiffness of the strain sensor was in the linear range for all measurements [29] and within the first 20% strain of the sensor [30]. Thus, the differences determined do not result from a different strain of the sensor, but from individual differences of the test persons.

Comparison of correlation between length change and internal knee rotation for all participants; the measurements are individualized for each participant for left (A) and right (B) knee. Significances, please see Table 1. All measurements were performed at 30° knee flexion


Box plots comparing the sensor length change on both sides; A, C = left knee; B, D = right knee, Top: differences between sex as groups; Bottom: differences between each participant; Male participants showed more variability in comparison with female participants. All measurements were performed at 30° knee flexion
Correlations between length change of the sensor and degrees of internal knee rotation
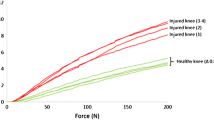
Figure 5 shows an example of the correlations between the change in length (normalized to the knee circumference) and the degree of internal knee rotation for a female and a male subject. In 30° of knee flexion and a torque of 2 Nm female subjects were able to rotate the tibia internally up to 40° and male subjects up to 20°. In female subjects a significant difference between the right and left knee was seen; in male subjects, the difference was not as pronounced.

Comparison of correlation between length change and internal knee rotation angle for a single representative female (A) and male (B) participant. Whereas females showed a higher laxity. Spearman’s correlation coefficient r and significance level p are positioned in the graphs
Spearman's rank correlation
Spearman's rank correlation evaluated the relation of sensor length change and angles of knee internal rotation. The dependent variable length change was regressed on predicting variable knee internal rotation angles and it has significantly predicted length change in all the participants on both sides. Table 1 shows the summary of findings and the reliability. It is evident that some subjects showed hardly any difference in the change in length of the sensor with maximum internal tibial rotation of the knee between the left and right side, while others showed clear differences. This applied to both female and male subjects.
Discussion
With the current work, it was possible to successfully evaluate for the first time a digital novel measurement method of anterolateral rotational laxity of the knee joint in vivo using capacitive strain sensors. The digital device was validated against a proven mechanical measurement system. The achieved precision and adaptability of the sensors showed a highly reliable applicability regarding the length change of the antero-lateral tissue strain for measurement of internal rotational laxity. In this content the importance of structures like the ALL, the anterolateral capsule, the iliotibial band or Kaplan fibers are documented in the recent studies [18, 31,32,33].
The measurement method of the strain sensor was established in vivo especially in the context of invasive blood pressure measurement, but has also been investigated on the cadaveric knee of humans [34, 35]. This measurement method using strain sensors which are applied to the skin in the course of the anterolateral ligament is based on the in vitro measurements on a simplified knee joint model of Zens et al. and on cadaveric knees of humans [26, 30]. Already in this in vitro experimental setup it could be shown that the bone-to-bone displacement was transferred to the skin and was measured there with the strain sensors. This could also be performed on human cadavers with capacitive strain sensors and KT-2000.
Owing to the Covid19 pandemic, the associated isolation, protective measures, the ethics committee to only allowed only 11 subjects. In order to avoid exposure risks, it was just possible to recruit members of the local university staff for the experiments according to the requirements of the ethics committee. To include patients with cruciate ligament pathologies was not approved by the ethics committee. Therefore, a new power calculation was necessary and the reliability of the measurement method was defined as primary endpoint.
The role of rotational laxity and subsequently extraarticular stabilizers was noted as early as 1989 at a meeting of the American Orthopaedic Society for Sports Medicine (AOSSM) at an expert conference [36]. In a current review Garcia-Mansilla et al. noted the importance of the anterolateral complex [27]. And especially in the case of recurrent anterior cruciate ligament ruptures, excessive rotational laxity is evident [21, 37]. The anterolateral soft tissue complex including the capsule, the Kaplan fibers and the IT band as a secondary stabilizer to the anterior cruciate ligament is increasingly understood [38, 39]. Some studies support the importance of the anterolateral ligament in anterior cruciate ligament reconstruction [40, 41].
In the current study, a significant sex-specific difference in internal rotational laxity of the knee joint was found. Previous studies examining hormone activity confirm differing ligament laxity between women and men. Sex differences in the biomechanical properties of tendons and ligaments are significant in the period of life in which the hormonal profile between women and men is significantly different [42].
Similar to the present results, a 2019 meta-analysis, including 76 studies, showed a side-to-side difference in ligament laxity of the knee joint. The asymmetry in laxity between internal and external rotation was significant for all flexion angles, with the largest mean difference at 30°. However, the dominant leg was not considered in this study [43]. By attaching the current strain sensors to the skin in direction of the anterolateral ligament and measuring the strain on the surface of the knee a dynamic and especially real-time measurement of the rotational laxity by a highly elastic strain sensor can be performed for the first time, unlike previous measurement methods (e.g. KT-2000 arthrometer, Rolimeter). Sex-specific studies of knee laxity are predescribed and were also shown in the context of other studies with a significantly higher laxity in women compared to men [44, 45] Thanks to the sensitivity of the sensor, we were able to detect for the first time a higher laxity of the dominant leg when comparing intraindividual differences [46]. Unlike static measurements on the model, however, a dynamic measurement method was used in vivo for the first time in the experimental setup and it was possible to show that the results are comparable to established measurement methods such as the Laxitester and, at the same time significant additional information could be gained [23]. Since the strain sensors are measuring a change in length and not a change in angle, a correction factor for the respective leg circumference was required for the conversion into an angle amount. During the measurements, it was noticed that there was often a significant difference in circumference between the two legs. Despite that, the reliability of the measurements was highly significant as shown in Table 1.
The next objective after the successful establishment of the strain sensors for the measurement of rotational laxity should be the use of the dynamic measurement system during activity or in everyday life. Up to now, investigations during rapid changes of direction, stair climbing or one-legged-hopping could only be carried out in the form of extremely time-consuming and error-prone motion tracking measurements on subjects in the laboratory due to a lack of other technical options [47]. The use of a strain sensor that is easy to produce is a unique argument for this application. Here, by integrating the strain sensor into a commercially available knee joint support a completely new possibility could be created to compare the patient's subjective impression of instability during activities such as walking upstairs or the one-legged hop with the objective measured laxity values through the easy-to-use strain sensor system. The possibilities may not be limited to the knee joint, but may also be further developed to examine ligament laxities at the elbow or ankle joint.
Limitations
Due to the ethical regulations during the Corona Pandemic, a relatively large angle difference of 5° was specified for the power calculation. Patients with cruciate ligament pathologies were not included due to the ethical regulations.
Conclusion
The present study shows that capacitive strain sensors can be used for reproducible laxity measurement of the soft tissue complex on the knee. In contrast to previous static systems, a dynamic measurement will be possible by this method in the future.
Data availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
References
Feng J, Cao Y, Tan L, Liang J, He C, He J, Wu S (2022) Anterior cruciate ligament reconstruction with lateral extra-articular tenodesis reduces knee rotation laxity and graft failure rate: a systematic review and meta-analysis. J Ortho Surg. https://doi.org/10.1177/10225536221095969
Katz JW, Fingeroth RJ (1986) The diagnostic accuracy of ruptures of the anterior cruciate ligament comparing the lachman test, the anterior drawer sign, and the pivot shift test in acute and chronic knee injuries. Am J Sports Med 14:88–91. https://doi.org/10.1177/036354658601400115
Schuster AJ, McNicholas MJ, Wachtl SW, McGurty DW, Jakob RP (2004) A new mechanical testing device for measuring anteroposterior knee laxity. Am J Sports Med 32:1731–1735. https://doi.org/10.1177/0363546504267050
Daniel DM, Stone ML, Sachs R, Malcom L (1985) Instrumented measurement of anterior knee laxity in patients with acute anterior cruciate ligament disruption. Am J Sports Med 13:401–407. https://doi.org/10.1177/036354658501300607
Niu X, Mai H, Wu T, Jiang Y, Duan X, Liu M, Liu J, Ding L, Ao Y (2022) Reliability of a novel automatic knee arthrometer for measuring knee laxity after anterior cruciate ligament ruptures. Orthop J Sports Med. https://doi.org/10.1177/23259671211051301
Jardin C, Chantelot C, Migaud H, Gougeon F, Debroucker MJ, Duquennoy A (1999) reliability of the kt-1000 arthrometer in measuring anterior laxity of the knee: Comparative analysis with telos of 48 reconstructions of the anterior cruciate ligament and intra- and interobserver reproducibility. Rev Chir Orthop Reparatrice Appar Mot 85:698–707
Bull AM, Andersen HN, Basso O, Targett J, Amis AA (1999) Incidence and mechanism of the pivot shift. An in vitro study. Clin Orthop Relat Res 363:219–231
Hoshino Y, Kuroda R, Nagamune K, Yagi M, Mizuno K, Yamaguchi M, Muratsu H, Yoshiya S, Kurosaka M (2007) In vivo measurement of the pivot-shift test in the anterior cruciate ligament—deficient knee using an electromagnetic device. Am J Sports Med 35:1098–1104. https://doi.org/10.1177/0363546507299447
Bignozzi S, Zaffagnini S, Lopomo N, Fu FH, Irrgang JJ, Marcacci M (2010) Clinical relevance of static and dynamic tests after anatomical double-bundle acl reconstruction. Knee Surg Sports Traumatol Arthrosc 18:37–42. https://doi.org/10.1007/s00167-009-0853-6
Lane CG, Warren RF, Stanford FC, Kendoff D, Pearle AD (2008) In vivo analysis of the pivot shift phenomenon during computer navigated acl reconstruction. Knee Surg Sports Traumatol Arthrosc 16:487–492. https://doi.org/10.1007/s00167-008-0504-3
Lopomo N, Zaffagnini S, Bignozzi S, Visani A, Marcacci M (2010) Pivot-shift test: analysis and quantification of knee laxity parameters using a navigation system. J Orthop Res 28:164–169. https://doi.org/10.1002/jor.20966
Lopomo N, Bignozzi S, Martelli S, Zaffagnini S, Iacono F, Visani A, Marcacci M (2009) Reliability of a navigation system for intra-operative evaluation of antero-posterior knee joint laxity. Comput Biol Med 39:280–285. https://doi.org/10.1016/j.compbiomed.2009.01.001
Caracciolo G, Yanez R, Silvestre R, De la Fuente C, Zamorano H, Ossio A, Stromback L, Abusleme S, Carpes FP (2021) Intraoperative pivot-shift accelerometry combined with anesthesia improves the measure of rotatory knee instability in anterior cruciate ligament injury. J Experim Orthop 8:80. https://doi.org/10.1186/s40634-021-00396-1
Kümmerlin J, Fabro HK, Pedersen PH, Jensen KK, Pedersen D, Andersen MS (2022) Measuring knee joint laxity in three degrees-of-freedom in vivo using a robotics- and image-based technology. J Biomech Eng. https://doi.org/10.1115/1.4053792
Csintalan RP, Ehsan A, McGarry MH, Fithian DF, Lee TQ (2006) Biomechanical and anatomical effects of an external rotational torque applied to the knee: a cadaveric study. Am J Sports Med 34:1623–1629. https://doi.org/10.1177/0363546506288013
Diermann N, Schumacher T, Schanz S, Raschke MJ, Petersen W, Zantop T (2009) Rotational instability of the knee: internal tibial rotation under a simulated pivot shift test. Arch Orthop Trauma Surg 129:353–358. https://doi.org/10.1007/s00402-008-0681-z
Colombet P, Robinson J, Christel P, Franceschi J-P, Djian P (2007) Using navigation to measure rotation kinematics during acl reconstruction. Clin Orthop Relat Res. https://doi.org/10.1097/BLO.0b013e31802baf56
Almquist PO, Arnbjörnsson A, Zätterström R, Ryd L, Ekdahl C, Fridén T (2002) Evaluation of an external device measuring knee joint rotation: an in vivo study with simultaneous roentgen stereometric analysis. J Orthop Res 20:427–432. https://doi.org/10.1016/S0736-0266(01)00148-6
Tsai AG, Musahl V, Steckel H, Bell KM, Zantop T, Irrgang JJ, Fu FH (2008) Rotational knee laxity: reliability of a simple measurement device in vivo. BMC Musculoskel Disord 9:35. https://doi.org/10.1186/1471-2474-9-35
Quinn TP, Mote CD, Skinner HB (1991) The effect of ankle constraint on the torsional laxity of the knee during internal-external rotation of the foot. J Biomech 24:511–525. https://doi.org/10.1016/0021-9290(91)90285-U
Mayr HO, Hellbruegge G, Haasters F, Ipach B, Schmal H, Prall WC (2021) Laxity measurement of internal knee rotation after primary anterior cruciate ligament rupture versus rerupture. Arch Orthop Trauma Surg. https://doi.org/10.1007/s00402-021-04269-1
Mayr HO, Reinhold M, Hube R, von Roth P, Bernstein A, Suedkamp N, Stoehr A (2014) Rotational laxity and collateral ligament laxity following total knee arthroplasty with rotating platform. Int Orthop 38:1379–1386. https://doi.org/10.1007/s00264-014-2308-z
Mayr HO, Hoell A, Bernstein A, Hube R, Zeiler C, Kalteis T, Suedkamp NP, Stoehr A (2011) Validation of a measurement device for instrumented quantification of anterior translation and rotational assessment of the knee. Arthrosc J Arthrosc Relat Surg 27:1096–1104. https://doi.org/10.1016/j.arthro.2011.02.034
Branch TP, Mayr HO, Browne JE, Campbell JC, Stoehr A, Jacobs CA (2010) Instrumented examination of anterior cruciate ligament injuries: minimizing flaws of the manual clinical examination. Arthrosc J Arthrosc Relat Surg 26:997–1004. https://doi.org/10.1016/j.arthro.2010.01.019
Mayr HO, Bruder S, Hube R, Bernstein A, Suedkamp NP, Stoehr A (2018) Single-bundle versus double-bundle anterior cruciate ligament reconstruction—5-year results. Arthrosc J Arthrosc Relat Surg 34:2647–2653. https://doi.org/10.1016/j.arthro.2018.03.034
Zens M, Niemeyer P, Bernstein A, Feucht MJ, Kühle J, Südkamp NP, Woias P, Mayr HO (2015) Novel approach to dynamic knee laxity measurement using capacitive strain gauges. Knee Surg Sports Traumatol Arthrosc 23:2868–2875. https://doi.org/10.1007/s00167-015-3771-9
Garcia-Mansilla I, Zicaro JP, Martinez EF, Astoul J, Yacuzzi C, Costa-Paz M (2022) Overview of the anterolateral complex of the knee. World J Clin Cases 10:8474–8481. https://doi.org/10.12998/wjcc.v10.i24.8474
Morgan AM, Bi AS, Kaplan DJ, Alaia MJ, Strauss EJ, Jazrawi LM (2022) An eponymous history of the anterolateral ligament complex of the knee. Knee Surg Relat Res 34:45. https://doi.org/10.1186/s43019-022-00172-0
Sheeja Prakash K, Mayr HO, Agrawal P, Agarwal P, Seidenstuecker M, Rosenstiel N, Woias P, Comella LM (2022) Batch fabrication of a polydimethlysiloxane based stretchable capacitive strain gauge sensor for orthopedics. Polymers 14:2326. https://doi.org/10.3390/polym14122326
Zens M, Niemeyer P, Ruhhammer J, Bernstein A, Woias P, Mayr HO, Südkamp NP, Feucht MJ (2015) Length changes of the anterolateral ligament during passive knee motion: a human cadaveric study. Am J Sports Med 43:2545–2552. https://doi.org/10.1177/0363546515594373
Liu A, Cui W, Yang W, Li C, Yan S, Xin Z, Wu H (2022) Anterior tibial subluxation of lateral compartment is associated with high-grade rotatory instability for acute but not chronic anterior cruciate ligament injuries: an magnetic resonance imaging case-control study. Arthroscopy 38:2852–2860. https://doi.org/10.1016/j.arthro.2022.04.012
Xu J, Qiao Y, Han K, Xu C, Dong S, Zhao J (2022) Modified lemaire lateral extra-articular tenodesis with the iliotibial band strip fixed on the femoral cortical surface reduces laxity and causes less overconstraint in the anterolateral lesioned knee: a biomechanical study. Arthroscopy. https://doi.org/10.1016/j.arthro.2022.06.016
Athanasiou V, Panagopoulos A, Kouzelis A, Kokkalis ZT, Lakoumentas J, Katsanos K, Gliatis J (2022) A review of current concepts of the anterolateral complex of the knee. Orthop Rev (Pavia) 14:38651. https://doi.org/10.52965/001c.38651
Bingger P, Zens M, Woias P (2012) Highly flexible capacitive strain gauge for continuous long-term blood pressure monitoring. Biomed Microdevices 14:573–581. https://doi.org/10.1007/s10544-012-9636-9
Zens M, Niemeyer P, Bernstein A, Feucht MJ, Kuhle J, Sudkamp NP, Woias P, Mayr HO (2015) Novel approach to dynamic knee laxity measurement using capacitive strain gauges. Knee Surg Sports Traumatol Arthrosc 23:2868–2875. https://doi.org/10.1007/s00167-015-3771-9
Ferretti A (2014) Extra-articular reconstruction in the anterior cruciate ligament deficient knee: a commentary. Joints 2:41–47
Nazzal EM, Keeling LE, Ryan PM, Herman ZJ, Hughes JD (2023) The role of lateral extra-articular tenodesis in anterior cruciate ligament reconstruction and treatment of rotatory knee instability: a scoping review. Curr Rev Musculoskelet Med. https://doi.org/10.1007/s12178-023-09832-4
Littlefield CP, Belk JW, Houck DA, Kraeutler MJ, LaPrade RF, Chahla J, McCarty EC (2021) The anterolateral ligament of the knee: an updated systematic review of anatomy, biomechanics, and clinical outcomes. Arthroscopy 37:1654–1666. https://doi.org/10.1016/j.arthro.2020.12.190
Sabatini L, Capella M, Vezza D, Barberis L, Camazzola D, Risitano S, Drocco L, Masse A (2022) Anterolateral complex of the knee: state of the art. World J Orthop 13:679–692. https://doi.org/10.5312/wjo.v13.i8.679
Kunze KN, Manzi J, Richardson M, White AE, Coladonato C, DePhillipo NN, LaPrade RF, Chahla J (2021) Combined anterolateral and anterior cruciate ligament reconstruction improves pivot shift compared with isolated anterior cruciate ligament reconstruction: a systematic review and meta-analysis of randomized controlled trials. Arthroscopy 37:2677–2703. https://doi.org/10.1016/j.arthro.2021.03.058
Geeslin AG, Chahla J, LaPrade RF (2022) Combined anterior cruciate ligament and lateral extra-articular reconstruction. Arthrosc J Arthrosc Relat Surg 38:2600–2601. https://doi.org/10.1016/j.arthro.2022.07.001
Renstrom P, Ljungqvist A, Arendt E, Beynnon B, Fukubayashi T, Garrett W, Georgoulis T, Hewett TE, Johnson R, Krosshaug T et al (2008) Non-contact acl injuries in female athletes: an international olympic committee current concepts statement. Br J Sports Med 42:394–412. https://doi.org/10.1136/bjsm.2008.048934
Ferle M, Guo R, Hurschler C (2019) The laxity of the native knee: a meta-analysis of in vitro studies. J Bone Joint Surg Am 101:1119–1131. https://doi.org/10.2106/JBJS.18.00754
Beynnon BD, Tourville TW, Hollenbach HC, Shultz S, Vacek P (2022) Intrinsic risk factors for first-time noncontact acl injury: a prospective study of college and high school athletes. Sports Health 2022:19417381221121136. https://doi.org/10.1177/19417381221121136
Park HS, Wilson NA, Zhang LQ (2008) Gender differences in passive knee biomechanical properties in tibial rotation. J Orthop Res 26:937–944. https://doi.org/10.1002/jor.20576
Ellison TM, Flagstaff I, Johnson AE (2021) Sexual dimorphisms in anterior cruciate ligament injury: a current concepts review. Orthop J Sports Med. https://doi.org/10.1177/23259671211025304
Sigurethsson HB, Karlsson J, Snyder-Mackler L, Briem K (2021) Kinematics observed during acl injury are associated with large early peak knee abduction moments during a change of direction task in healthy adolescents. J Orthop Res 39:2281–2290. https://doi.org/10.1002/jor.24942
Acknowledgements
The German Research Foundation (DFG) is acknowledged for funding this project (grant number: 222567169). Melanie Lynn Hart is acknowledged for supervising the manuscript as a native English speaker.
Funding
Open Access funding enabled and organized by Projekt DEAL. Deutsche Forschungsgemeinschaft (222567169).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest with regard to the current study.
Ethical approval
Ethics approval was given on December 7, 2021, by the Ethics Committee of Freiburg University Germany with number 487/16.
Informed consent
Each subject was informed about the research project and signed a declaration of consent.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mayr, H.O., Rosenstiel, N., Prakash, K.S. et al. Digital measurement of anterolateral knee laxity using strain sensors. Arch Orthop Trauma Surg 143, 6719–6729 (2023). https://doi.org/10.1007/s00402-023-05024-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-023-05024-4