
Summary
Background: A fractional flow reserve (FFRmyo) <0.75 is a well validated parameter for significance of coronary stenoses in cases of normal myocardial function. We used the FFRmyo limit in patients with impaired myocardial perfusion by myocardial infarction and/or hypertension for intermediate stenoses of the LAD for decision to PTCA and checked the indication by clinical follow-up.
Methods: In 20 pts (5 women) with chest pain and visual 50 D% LAD stenoses, the FFRmyo was obtained by using a RADI-Pressure-Wire, the CFR by a densitometric technique (HODGSON), and the geometry of stenosis (minimal lumen diameter and diameter stenosis) by quantitative coronary angiography (QCA). EF and the kinetics of the anterolateral wall (expressed as radial shortening fraction) were measured by laevography.
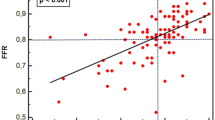
Results: The mean age of our 20 pts. was 59.4 years: 13 of the pts. (65%) had a history of hypertension, 9 (45%) pts. a history of myocardial infarction. The mean diameter stenosis was 50.8%. The mean value of CFR was 2.9. The FFRmyo ranged from 0.66 to 0.90, the mean value was 0.78. The 12 pts. with FFRmyo≥0.75 (60%, group A) were treated with the usual antianginal medications. A PTCA was performed only in patients with FFRmyo<0.75 (N=8 (40%), group B). Except for one pt. with instent restenosis, in the 7 pts. with denovo stenoses stent implantation was performed. Significant differences between the groups A and B were seen only for the total number of myocardial infarctions (8/12 vs. 1/8) and diameter stenosis (48.5% vs. 54.3%). All lesions of group B had a diameter stenosis of 50% or higher. CFR correlated significantly with the radial shortening fraction (r=0.75), minimal lumen diameter (r=–0.51) and diameter stenosis (r=–0.46). FFRmyo correlated with diameter stenosis (r=–0.47) only. All pts. treated with PTCA were primarily free of pain or reduced angina at least 1 CCS stage; only one developed an angina due to a restenosis (74D%) 2 months after PTCA and stent implantation. The pts. of group A did not get worse, nor were they readmitted within 6 to 13 months after catheterization.
Conclusions: Pts. with 50 D% stenoses, impaired myocardial perfusion and FFRmyo<0.75 had a good long-term benefit concerning clinical and angiographic result. No pts. with FFRmyo<0.75 had a D% lower than 50; therefore, the PTCA of intermediate stenoses without quantification must be avoided. CFR is not helpful for a decision to PTCA in such cases, because a normal value of CFR is relevant only.
Zusammenfassung
Fragestellung: Eine fraktionelle Flussreserve (FFRmyo) <0,75 ist ein validierter Parameter für die Relevanz von Koronarstenosen, wenn die Myokardfunktion normal ist. Wir verwendeten den FFRmyo-Grenzwert bei Patienten mit gestörter Myokardperfusion (Myokardinfarkt und/oder Hypertonie) bei 50%-igen LAD-Stenosen als Indikation zur PTCA und überprüften diese Entscheidung nach dem klinischen Follow-Up.
Patienten/Methodik: Wir untersuchten 20 Patienten (5 Frauen) mit visuell 50% LAD-Stenosen. Diese wurden mittels QCA durch den minimalen Stenose-Diameter und den Stenosegrad charakterisiert, die fraktionelle Flussreserve wurde mit dem RADI- Druckmessdraht bei 12mg Papaverin i.c. gemessen. Die CFR wurde densitometrisch bestimmt. Die Vorderwandkinetik wurde durch die relative Radialachsenverkürzung der Anterolateralregion aus dem Laevogramm quantifiziert.
Ergebnisse: Das mittlere Alter aller Patienten war 59 Jahre, 13 Patienten (65%) hatten eine Hypertonie, 9 (45%) eine Infarktanamnese. Der mittlere Stenosegrad war 50,8%. Die koronare Flussreserve betrug im Mittel 2,9, die FFRmyo 0,78 (0,66–0,90). 12 Patienten (60%, Gruppe A) mit FFRmyo≥0,75 wurden konservativ therapiert, die 8 übrigen Patienten (40%, Gruppe B) mit FFRmyo<0,75 erhielten eine PTCA. 1 Patient mit Instent-Restenose wurde ausschließlich mit Ballondilatation behandelt, bei den 7 Patienten mit Denovo-Stenosen wurden Stents implantiert. Signifikante Unterschiede (p<0,05) zwischen den Gruppen A und B gab es bei der Gesamtzahl der Myokardinfarkte (8/12 vs. 1/8) und dem Stenosegrad (48,5% vs. 54,3%), in Gruppe B war dieser stets ≥50%. Die CFR korrelierte signifikant mit der relativen Radialachsenverkürzung (r=0,75), dem Minimaldiameter (r=0,51) und dem Grad der Stenosen (r=–0,46), die FFRmyo nur mit letzterem (r=–0,47). Bei den mit Stent behandelten Patienten erfolgte nach 3–6 Monaten (Mittel 4,7) ein Kontrollkoronarographie. Alle mit PTCA behandelten Patienten wurden primär beschwerdefrei bzw. besserten sich um mindestens 1 CCS-Stadium. Ein Patient entwickelte nach 2 Monaten erneut eine Angina pectoris und zeigte ein 74%ige Instent-Restenose. Die nur medikamentös therapierten Patienten blieben stabil.
Schlussfolgerungen: Auch Patienten mit gestörter Myokardperfusion und nur 50%igen LAD-Stenosen profitieren bei FFRmyo<0,75 und bei optimalem Primärergebnis klinisch von einer PTCA. Unabhängig von der FFRmyo ist ein Stenosegrad ≥50% ein obligatorisches Kriterium für hämodynamisch relevante Stenosen, bei mittelgradigen Einengungen ist dieser Grenzwert nur mittels QCA ausreichend genau bestimmbar. Die CFR ist für eine Entscheidung zur PTCA bei mittelgradigen Stenosen allenfalls bedingt geeignet, da nur ein Normalwert diagnostisch relevant ist.
Similar content being viewed by others


Author information
Authors and Affiliations
Additional information
Eingegangen: 15. April 1999/Akzeptiert: 10. September 1999
Rights and permissions
About this article
Cite this article
Rother, T., Neugebauer, A., Mende, M. et al. Die fraktionelle Flussreserve als Entscheidungskriterium zur Intervention bei Patienten mit 50%-igen Koronarstenosen und gestörter Myokardperfusion. Z Kardiol 89, 307–315 (2000). https://doi.org/10.1007/s003920050490
Issue Date:
DOI: https://doi.org/10.1007/s003920050490